
Abstract
Background and Objectives:
The breast undergoes extensive physiologic changes during pregnancy/lactation. We aimed to review the ultrasound (US) imaging characteristics of breast lesions during pregnancy/lactation and to demonstrate ultrasonography as an excellent imaging modality in this patient population.
Materials and Methods:
We performed a retrospective study involving 195 patients with 206 pathologically confirmed breast lesions during pregnancy/lactation over the period of January 2010 to December 2018; 51 were diagnosed with breast cancer, including 50 invasive ductal carcinomas and 1 low malignant potential phyllodes tumor, whereas 144 were diagnosed with 155 benign lesions, including 103 mastitis/abscesses, 45 fibroadenomas, 2 intraductal papillomas, 2 sclerosing lesions, and 3 benign phyllodes tumors. The patients' age, lesion diameter, and US characteristics were analyzed.
Results:
The breast lesions of patients during pregnancy/lactation were compared with those during nonpregnancy/lactation. Patients with breast cancer or fibroadenomas during pregnancy/lactation were younger than those during nonpregnancy/lactation. The average lesion diameter was significantly higher among pregnant/lactating patients compared with controls of childbearing age for fibroadenomas, but not for malignant lesions. The fibroadenomas and mastitis/abscesses during pregnancy/lactation usually have higher BI-RADS categories than those during nonpregnancy/lactation.
Conclusions:
The imaging features of breast cancer during pregnancy/lactation did not differ much from those of nonpregnancy/lactation; however, some benign lesions had suspicious sonographic features, and US-guided core biopsies were necessary for differentiating benign from malignant lesions.
Introduction
The breast is a dynamic organ that undergoes substantial changes throughout a woman's life, especially during pregnancy/lactation. The clinical and radiological detection and evaluation of breast masses during pregnancy/lactation are complicated by the increased volume and firmness of the breasts with elevations in hormone levels.1–6 In addition, a delay in diagnosis secondary to the lack of awareness is also an important factor responsible for the advanced stage and poor prognosis of pregnancy-associated and postpartum breast cancers.7,8
Ultrasound (US) could be vital during this period because it lacks ionizing radiation, does not use gadolinium-based contrast agents, and can detect most masses.9,10 The differential diagnosis of a breast mass during pregnancy/lactation includes breast cancer and benign lesions such as fibroadenomas, mastitis, and fibrocystic changes. 11
In this work, we aimed to review the US characteristics of breast lesions during pregnancy/lactation and emphasize the value of US as an appropriate and effective method of evaluating breast disorders in this patient population.
Materials and Methods
We reviewed the US and pathology records of 195 patients (including 4 during pregnancy and 191 during lactation) with 206 breast lesions during pregnancy/lactation and who were referred to the Shanghai Cancer Center, Fudan University, Shanghai, China, between January 2010 and December 2018. All lesions were evaluated through US examination and categorized in accordance with the Ultrasound Breast Imaging Reporting and Data System (US BI-RADS). We randomly selected 100 breast cancer and 100 fibroadenoma cases during nonpregnancy/lactation as control cases. Final diagnoses were confirmed through histopathological examination using core needle biopsy or surgery. The experimental protocol was approved by the Ethics Committee of the Shanghai Cancer Center.
Statistical analyses were performed using SPSS version 22.0 for Windows (IBM, Armonk, NY). Independent two-sample t-test was conducted to analyze categorical variables, and p < 0.05 was considered significant. The Mann–Whitney U test was conducted to analyze the statistical significance of US BI-RADS categories of breast cancers and fibroadenomas diagnosed during pregnancy/lactation.
Results
A total of 195 patients with 206 pathologically confirmed breast lesions were included in this study. Among all patients, 51 (26.2%) were diagnosed with 51 (24.8%) breast cancer lesions, including 50 invasive ductal carcinomas and 1 low malignant potential phyllodes tumor, whereas 144 (73.8%) were diagnosed with 155 (75.2%) benign lesions, including 103 mastitis/abscesses, 45 fibroadenomas, 2 intraductal papillomas, 2 sclerosing lesions, and 3 benign phyllodes tumors.
The patients were from ages 21 to 45 years (mean age: 31.7 ± 4.7 years). Lesion diameters ranged from 5 to 150 mm (mean diameter: 31.5 ± 19.4 mm). Three unmeasurable lesions were excluded. Patients with breast cancer were older than those with mastitis/abscesses, fibroadenomas, and phyllodes tumor (p < 0.05). Moreover, the diameter of breast cancer lesions was larger than that of mastitis/abscesses, fibroadenomas, and sclerosing lesions (p < 0.05). However, the diameter of phyllodes tumor was larger than that of breast cancer, mastitis/abscesses, fibroadenomas, intraductal papillomas, and sclerosing lesions (p < 0.05). The results are summarized in Table 1.
Age and Diameter Information of Breast Lesions Diagnosed During Pregnancy and Lactation
p < 0.05 versus malignant.
p < 0.05 versus phyllodes tumor.
The ages and diameters of the randomly selected 100 breast cancer and 100 fibroadenoma cases during nonpregnancy/lactation were compared with those of the 51 breast cancer and 45 fibroadenoma cases during pregnancy/lactation, respectively. Patients with breast cancer or fibroadenomas during pregnancy/lactation were younger than those during nonpregnancy/lactation. However, the diameter data were contrary to the age data (p < 0.05). The results are summarized in Table 2. Given that the nonpregnancy/lactation group included some patients who were not of the childbearing age, the statistical results might have deviations. Hence, we selected patients within the same age range as those in the pregnancy/lactation group (21–45 years), including the 33 breast cancer and 61 fibroadenoma cases. The diameter of the fibroadenoma group showed statistical difference. The results are summarized in Table 3.
Age and Diameter Comparisons of Breast Cancer and Fibroadenomas Diagnosed During Pregnancy/Lactation (+) and Nonpregnancy/Lactation (−)
p < 0.05 intragroup comparison.
Age and Diameter Comparisons of Breast Cancer and Fibroadenomas Diagnosed During Pregnancy/Lactation (+) and Nonpregnancy/Lactation (−) (Childbearing Period)
p < 0.05 intragroup comparison.
Table 4 shows the US BI-RADS categories of all lesions. To determine whether breast lesions during pregnancy/lactation had higher categories than those during nonpregnancy/lactation, the categories of breast cancer and fibroadenomas detected during pregnancy/lactation and nonpregnancy/lactation were compared (Table 5). US BI-RADS category 6 breast cancer cases were excluded. Given the rarity of mastitis/abscess cases during nonpregnancy/lactation, fibroadenomas during nonpregnancy/lactation were still used as a control sample. In the malignant group, the US BI-RADS rank difference was not statistically significant. However, in the fibroadenoma and mastitis/abscess group, the US BI-RADS rank difference was statistically significant (p < 0.05, two tailed), suggesting that fibroadenomas and mastitis/abscesses during pregnancy/lactation usually have higher categories than those during nonpregnancy/lactation.
The Ultrasound Breast Imaging Reporting and Data System Category of All the Lesions During Pregnancy/Lactation
US BI-RADS, Ultrasound Breast Imaging Reporting and Data System.
The Ultrasound Breast Imaging Reporting and Data System Category Difference Between Pregnancy/Lactation (+) and Nonpregnancy/Lactation (−) (Childbearing Period)
p < 0.05 versus fibroadenomas during nonpregnancy/lactation (childbearing period).
US BI-RADS, Ultrasound Breast Imaging Reporting and Data System.
The properties (cystic, solid, or mixed), shapes (regular or irregular), and calcification status (with or without) of lesions during pregnancy/lactation and nonpregnancy/lactation were evaluated (Table 6). Breast lesions during pregnancy/lactation were more complicated and diverse (Figs. 1–6) compared with those during nonpregnancy/lactation (Figs. 7 and 8). The imaging features of breast cancer during nonpregnancy/lactation did not significantly differ from those during nonpregnancy/lactation; however, some benign lesions had suspicious sonographic features and were more likely to be irregular and have calcification.
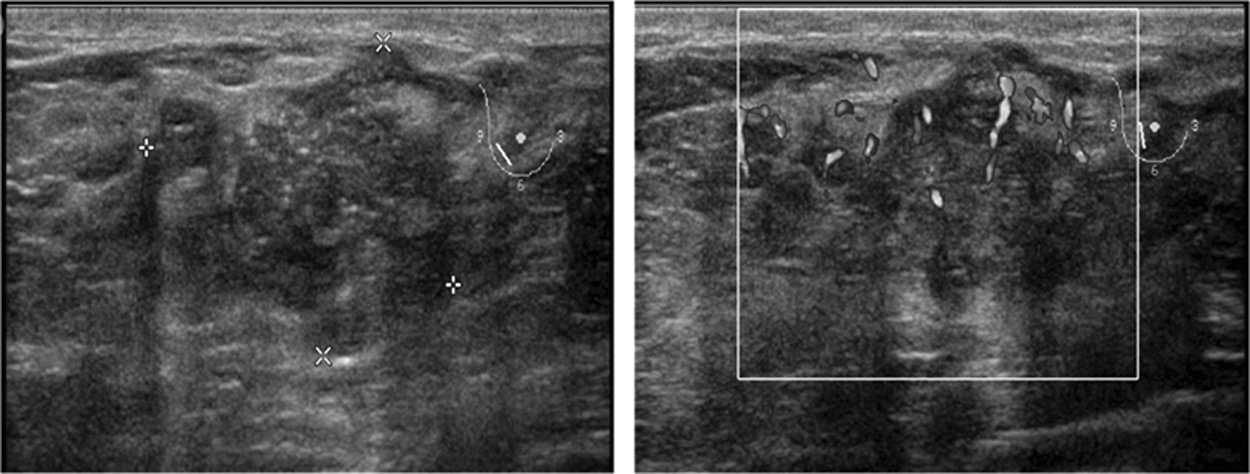
Breast cancer lesion (28 × 22 mm) during lactation in a 42-year-old woman. The tumor appeared as an irregular, poorly defined solid mass with microcalcification. CDFI revealed abundant blood flow in the tumor. CDFI, color Doppler flow imaging.
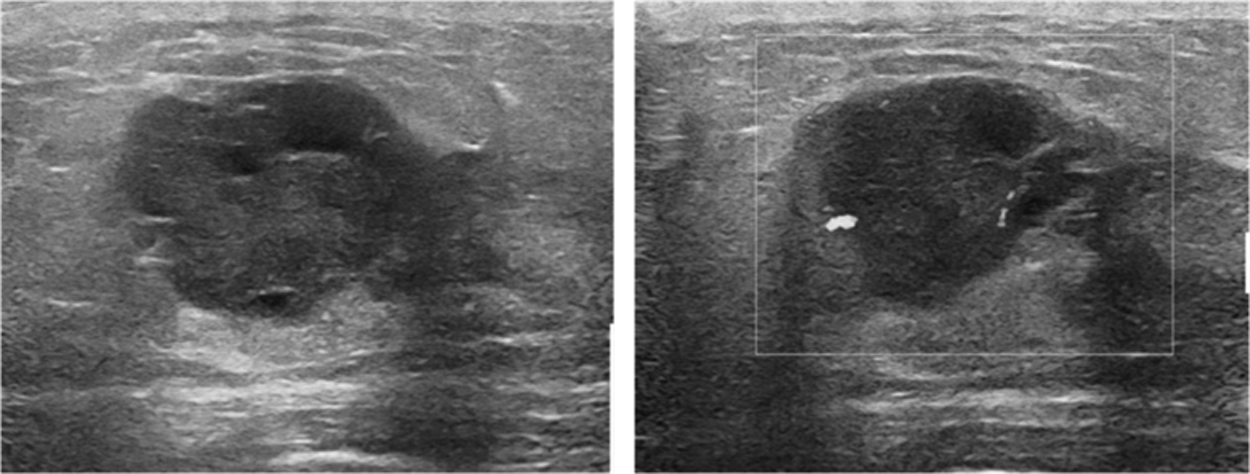
Breast cancer lesion (27 × 21 mm) during lactation in a 34-year-old woman. The tumor appeared as an irregular, well-defined mixed mass. CDFI revealed minimal blood flow in the tumor.
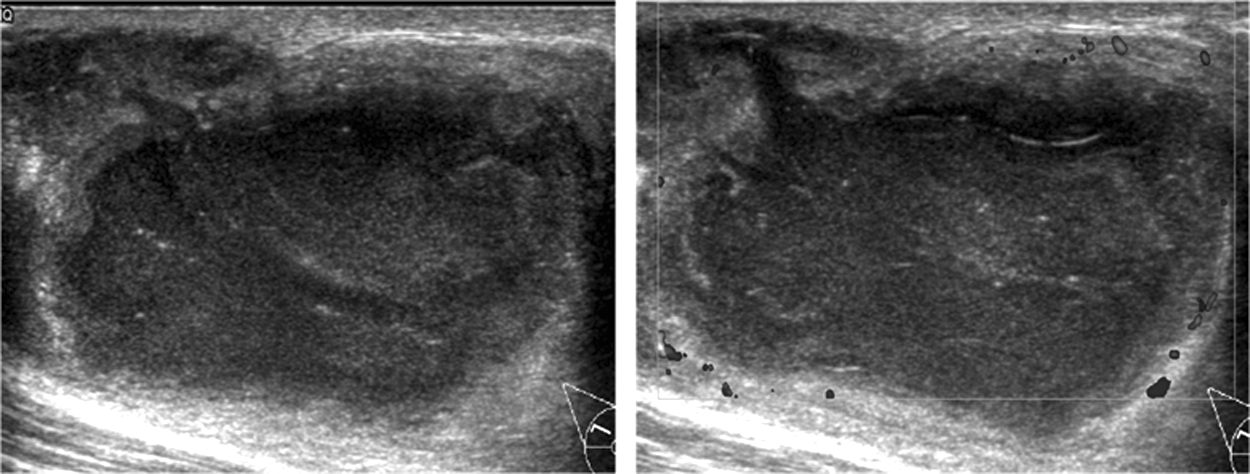
Mastitis/abscesses (47 × 26 mm) during lactation in a 29-year-old woman. The lesion appeared as an irregular, well-defined cystic mass filled with dot echoes. CDFI revealed minimal blood flow around the cyst.
Mastitis/abscesses (28 × 14 mm) during lactation in a 40-year-old woman. The cyst appeared as an irregular, ill-defined mixed mass. CDFI revealed minimal blood flow around the mass.

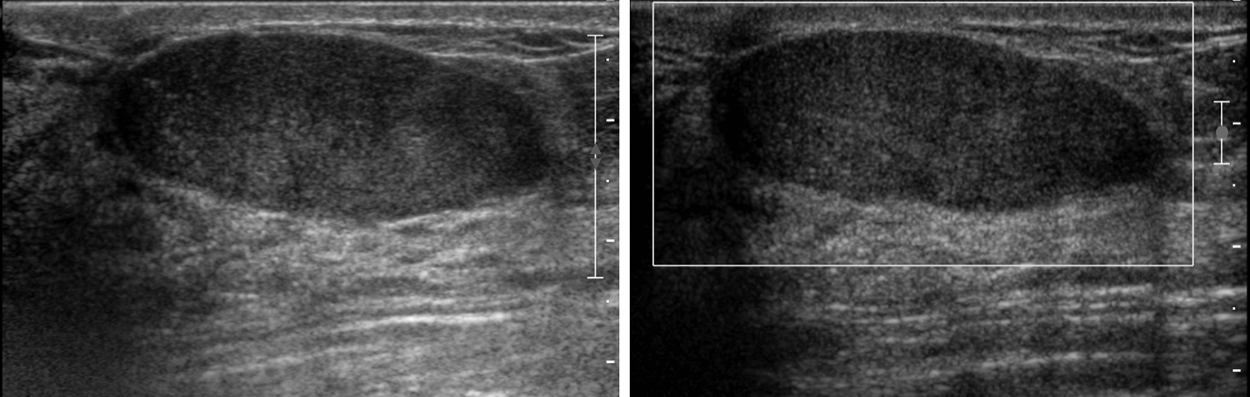
Fibroadenomas (23 × 13 mm) during pregnancy in a 29-year-old woman. The lesion appeared as a regular, well-defined solid mass. CDFI revealed abundant blood flow in the mass.
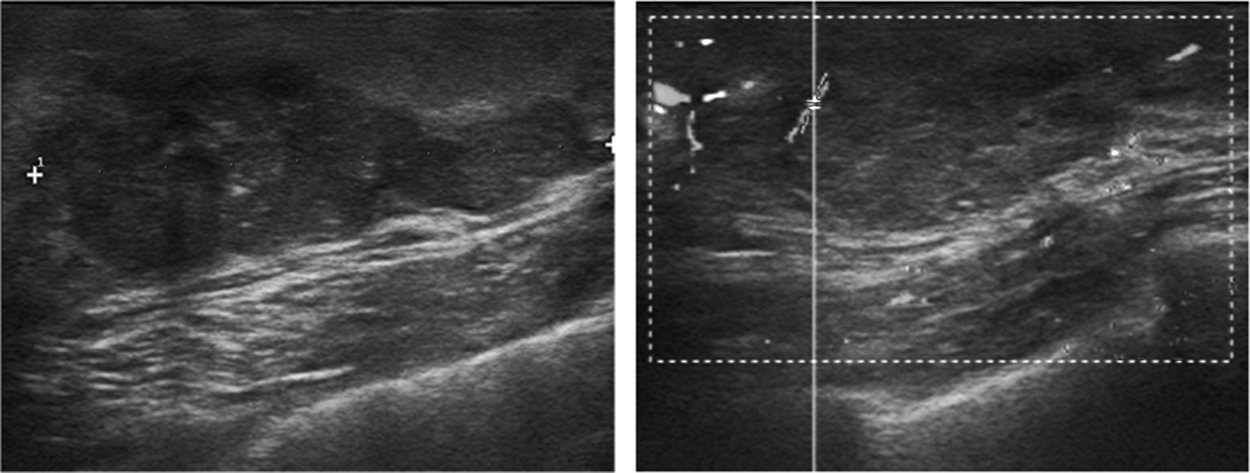
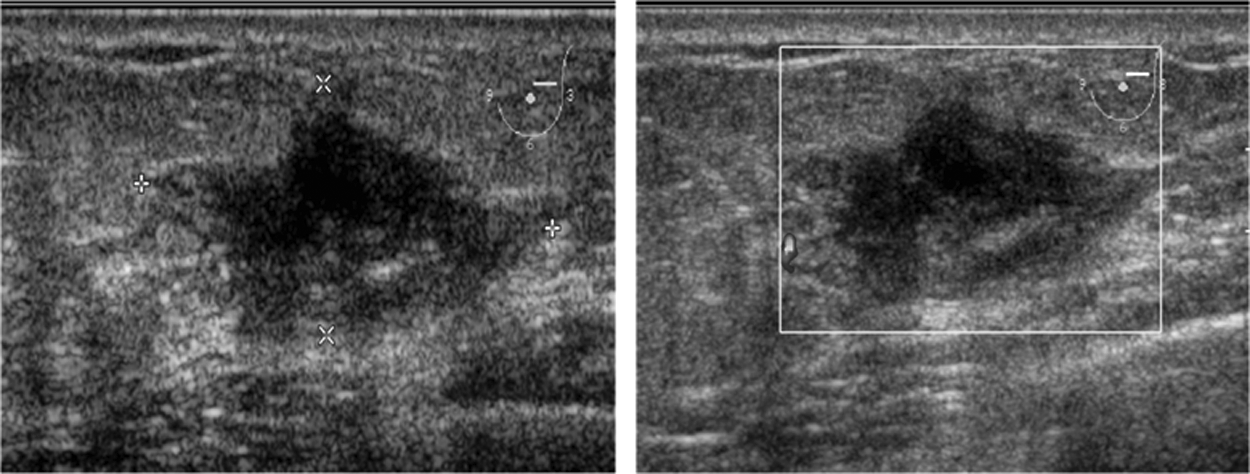
Fibroadenomas (45 × 13 mm) during lactation in a 25-year-old woman. The lesion appeared as an irregular, poorly defined solid mass. CDFI revealed minimal blood flow in the mass.

Breast cancer lesions (35 × 17 mm) during nonpregnancy/lactation in a 60-year-old woman. The tumor appeared as an irregular, poorly defined solid mass. CDFI revealed abundant blood flow in the tumor.
Fibroadenomas (44 × 16 mm) during nonpregnancy/pregnancy in a 49-year-old woman. The lesion appeared as a regular, well-defined solid mass. CDFI revealed undetectable blood flow in the mass.
The Ultrasound Characteristics of Breast Lesions During Pregnancy/Lactation (+) and Nonpregnancy/Lactation (−) (Childbearing Period)
Discussion
The lactating breast presents special problems for breast US imaging due to hypertrophic changes. Similar to nonpregnant/lactating patients, most pregnant/lactating patients are found to have benign disease upon breast imaging. Pregnant and lactating patients who present for breast imaging should first be subjected to US. 9
Previous studies that described the accuracy of breast imaging in this population included a small number of patients and case reports.12–17 Our study retrospectively analyzed 195 patients with 51 malignant and 155 benign lesions that were diagnosed over a period of 9 years. In addition, this work compared the age, lesion diameters, US characteristics, and BI-RADS category in patients who were not pregnant/lactating. The results will present more useful information for radiologists in clinical practice compared with a simple description of breast lesions during pregnancy and lactation.
Women with lesions during pregnancy/lactation were younger and had larger lesion diameters than those with breast cancer or fibroadenomas during nonpregnancy/lactation. The lesion characteristics of the two groups significantly differed and might be attributed to the rapid growth of lesions in response to increased hormone levels and severity of symptoms. When the bias originating from patients of nonchildbearing age was excluded, differences in the breast cancer lesion diameters of pregnant/lactating and nonpregnant/lactating groups were no longer statistically significant. This result might be attributed to the wide range of tumor diameters of patients with breast cancer during lactation.
The US BI-RADS ranks of benign lesions during pregnancy/lactation were higher than those of lesions during nonpregnancy/lactation because of two possible reasons. First, the common characteristics of benign lesions became nonspecific with the thickening of mammary glands and the change in acoustic condition. Second, the cancer incidence in the study institution, given that it specializes in cancer, may be higher than that in other general hospitals. Thus, doctors would assign high ranks in cases to avoid missed diagnoses.
Although breast cancer during pregnancy/lactation showed typical malignant characteristics, more benign lesions during this period had suspicious sonographic features (irregular and calcification) than pregnancy/lactation. For example, fibroadenomas may occasionally become infarcted during pregnancy/lactation secondary to rapid growth outpacing the vascular supply. Infarcted fibroadenomas may differ from typical fibroadenomas and present as tender nonmobile masses. Microcalcifications secondary to gestational or secretory hyperplasia can be seen in US, although more clearly in mammography, making fibroadenomas during pregnancy/lactation more conspicuous. This finding usually induces a higher BI-RADS category rank. Therefore, a meticulous follow-up or US-guided core biopsies are necessary to differentiate benign from malignant lesions.
Our study is limited by several factors. First, as mentioned above, higher incidences of cancer during pregnancy/lactation might have been recorded in the study institution than in general hospitals. Second, the pathology result was taken as the gold standard, and data might be incomplete for some patients, including those who were under follow-up observation or receiving anti-inflammatory therapy and did not demonstrate progression or recovery. Third, the breast lesions included in our study were detected via US only. Thus, some breast cancer cases that could only be correctly diagnosed through mammography might have been incorrectly categorized.
Conclusions
Various breast lesions during pregnancy/lactation were detected, and imaging of these lesions revealed variable findings. In pregnant or lactating patients, avoiding a delay in diagnosis of breast cancer is the most urgent task of radiologists. Although benign breast lesions during pregnancy/lactation may have suspicious malignant sonographic features and/or higher BI-RADS scores, breast US is an important imaging modality for the diagnosis and differentiation of benign and malignant lesions. When imaging results are suspicious, a biopsy should be performed to obtain a pathological diagnosis.
Footnotes
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
No funding was received.