
Abstract
Background/Objectives:
Early breastfeeding initiation is strongly recommended. Reasons for delayed breastfeeding initiation often include intrapartum interventions such as induction of labor, opioid pain medication administration, epidural analgesia, and caesarean birth. The majority of existing studies examining the timeliness of breastfeeding initiation are from low- or middle-income countries. The objective of this study is to examine intrapartum interventions on the time to breastfeeding initiation in a cohort of mothers from a high-income country.
Materials and Methods:
A cohort of 1,277 new mothers was recruited within 24 hours after birth from 4 hospitals in Hong Kong from 2011 to 2012. Participants completed a self-administered questionnaire immediately after recruitment. The rates of intrapartum interventions and the time to the first breastfeed were collected from participants' hospital record.
Results:
Among participants, 575 (45.5%) initiated breastfeeding within 1 hour of birth and the median time to the first breastfeed was 1.5 hours. The use of opioid pain medication (adjusted hazard ratio [aHR]: 0.78, 95% confidence interval [CI]: 0.67–0.91), assisted vaginal birth (aHR: 0.74, 95% CI 0.56–0.97), and caesarean section (aHR: 0.30, 95% CI 0.25–0.36) were associated with delayed breastfeeding, whereas epidural analgesia and induction of labor had no effect on breastfeeding initiation. Natural birth (i.e., no intrapartum interventions) was also significantly associated with early breastfeeding initiation (aHR: 1.75, 95% CI 1.54–1.99).
Conclusions:
Breastfeeding initiation was delayed in participants who had a caesarean birth and who received opioid pain medication. These women may require additional support to initiate breastfeeding soon after birth.
Introduction
The importance of early breastfeeding initiation has been widely recognized. In 1989, the World Health Organization (WHO) and the United Nations Children's Fund (UNICEF) outlined 10 steps for hospitals to promote successful breastfeeding. 1 One of the 10 steps (step 4) recommends that new mothers initiate breastfeeding within the first half hour after birth. In low-income countries, early breastfeeding initiation is associated with a reduction in neonatal mortality, 2 while in high-income countries, it is associated with longer breastfeeding duration. 3 One study found that new mothers who initiated breastfeeding within the first hour after birth breastfed for ∼5 weeks longer than mothers who initiated after the first hour. 4 Globally, only 42% of infants are breastfed within the first hour of life. 5
Reasons for delayed initiation of breastfeeding vary, and include intrapartum interventions such as induction of labor, opioid pain medication administration, epidural analgesia, and caesarean birth. However, studies examining the association between intrapartum interventions and early initiation of breastfeeding have shown inconsistent findings. One study found that the use of epidural analgesia and pethidine during labor was associated with delayed initiation of breastfeeding, 6 but another found no association between these factors. 7 A recent systematic review of the effect of hospital practices on the time to breastfeeding initiation only included studies from low- or middle-income countries. 8 However, birthing practices differ among low-, middle-, and high-income countries. In low-income countries, fewer mothers give birth in health care facilities 9 and maternal and neonatal mortality rates are much higher than high-income countries.10,11 Therefore, promoting early breastfeeding initiation is vitally important to child survival, an issue that is not as prevalent in high-income countries. One recent study in Singapore, a high-income country, found that operative birth was associated with delayed breastfeeding initiation, but found no association between pethidine administration and epidural analgesia with breastfeeding initiation. 12 However, the main focus of the Singapore study was on skin-to-skin contact and there is no other recent research on the time to breastfeeding initiation in high-income countries. Therefore, the objective of the study was to examine the effect of intrapartum interventions on the time to breastfeeding initiation in a cohort of Hong Kong mothers intending to breastfeed.
Methods
Study design, participants, and setting
We conducted a multicenter prospective longitudinal cohort study. The study methods are described in more detail elsewhere. 13 Participants were recruited from the postnatal obstetric units of four geographically distributed public hospitals in Hong Kong from 2011 to 2012. Hong Kong has 8 public and 11 private hospitals that provide obstetric services. Public hospitals provide high-quality free antenatal and postnatal care to all residents and Hong Kong is a global leader in maternal and child health outcomes. 14 In 2017, two-thirds (67%) of all births in Hong Kong were in public hospitals. 15 None of the study hospitals was designated as baby friendly at the time of participant recruitment and the breastfeeding initiation rate of mothers who gave birth in Hong Kong public hospitals at the time of this study was 80.6%. 16 Study inclusion criteria were as follows: at least 18 years of age, Cantonese speaker, lived in Hong Kong for at least 1 year, no serious medical or obstetrical complications, singleton pregnancy, and intended to breastfeed. In addition, the baby was required to be at least 37 weeks of gestational age, be with a birth weight of at least 2,500 g, have 5-minute Apgar score of at least 8, and have no severe congenital disorders or medical complications. Infants who were admitted to the Neonatal Intensive Care Unit or who were placed in the Special Care Baby Unit for more than 48 hours were excluded.
Data collection
A research nurse recruited mother-and-infant pairs from the study hospitals, usually within the first 24 hours after birth. A self-administered questionnaire was completed by each participant. The questionnaire collected information on basic sociodemographic characteristics, breastfeeding intentions and experience, family members' infant feeding preferences, and attendance at antenatal childbirth and breastfeeding classes. Detailed maternal and neonatal data, the time of breastfeeding initiation, and in-hospital feeding data were retrieved from the medical records. In-hospital feeding data were collected for the first 48 hours after birth as majority of the mothers were discharged after 48 hours postpartum. Participants were followed up to 12 months postpartum, or until breastfeeding stopped. However, only data collected during the postpartum hospital admission are reported here.
Study variables
The outcome variable was the time to breastfeeding initiation after birth, measured in hours. Two outcomes were assessed: breastfeeding initiation within the first hour after birth (yes/no) and the overall time to the initiation of the first breastfeed. Breastfeeding initiation was defined as the time that the baby was first put to the breast. These data were extracted from the medical record by the research nurse and reconfirmed with the participant. We examined a number of predictor variables, including gestational age, birth weight, time of birth, induction of labor, opioid pain medication, epidural analgesia, mode of birth, and whether the participant had a natural birth. Gestational age was categorized as early term (37 to <39 weeks) and term (≥39 weeks) and the time of birth was categorized according to the nursing staff shift timing in the study hospitals. Intrapartum epidural analgesia for the majority of participants (96%) consisted of an opioid medication (e.g., either fentanyl or morphine and a local anesthetic), whereas intramuscular opioid pain relief medication was normally pethidine. Pethidine is a synthetic opioid, which is the most widely used opioid for pain relief during labor. 17 Participants were categorized as having a natural birth if they had a spontaneous vaginal birth without labor induction and pain-relieving medications. We also adjusted for other covariates that are known to affect breastfeeding initiation in this population 18 (e.g., maternal age, maternal educational, household income, parity, attendance at antenatal education classes, previous breastfeeding experience, and exclusive breastfeeding intentions) and the study site.
Data analysis
Descriptive statistics were used to summarize the sample characteristics. Bivariable and multivariable logistic regression were used to compute the unadjusted and adjusted odds ratios (aORs) of the factors associated with breastfeeding initiation within 1 hour after birth. Hosmer-Lemeshow tests were used to assess the goodness of fit of the logistic models. Variance Inflation Factor (VIF) test was used to detect multicollinearity between variables. Kaplan-Meier curves were constructed to examine the association between natural birth and the time of the first breastfeed and the Log-rank test was used to detect group differences. Bivariable and multivariate Cox proportional hazards regression were used to assess the association between the predictor variables and time to breastfeeding initiation. We tested the proportional hazards assumption by using log–log plots of estimated survival curves. In both the multivariable logistic regression and Cox proportional hazards models, we adjusted for all of the predictor variables and the previously identified covariates. Data analysis was conducted using Stata version 14.2 (Stata Corp., College Station, TX). A 95% confidence interval (CI) and .05 level of significance were used throughout the study.
Ethical approval
Ethical approval was obtained from the Institutional Review Board of the University of Hong Kong/Hospital Authority Hong Kong West Cluster and all participating hospitals. Informed written consent was obtained from all participants.
Results
In total, 1,277 mother-infant pairs were recruited from the 4 participating study hospitals. Fourteen participants who received general anesthesia during labor were excluded. The use of general analgesia significantly delays breastfeeding initiation as breastfeeding should only be started when the mother is fully awake and not overly sedated. 19 Finally, 1,263 mother-infant pairs were included in this analysis. Although we do not have precise data on study participation rates, based on the monthly birth rates at the four study sites, 20 the breastfeeding initiation rate in public hospitals at the time of the recruitment (76%), 21 and the proportion of ineligible participants, 16 we estimate that we recruited between 33% and 42% of all eligible participants in the four hospitals during the study period (Supplementary Table S1).
The characteristics of the sample are presented in Table 1. Almost 70% of participants were 30 years of age or older, over one-half had completed secondary education, 47.1% had a monthly family income of greater than $30,000 (∼$3,800 USD), and the majority (78.2%) planned to exclusively breastfed. Almost 20% of participants received intramuscular opioid for pain relief in labor, only 4.3% received epidural analgesia, and labor was induced in 28.0% of participants. Approximately one-half of the participants (50.8%) had a natural birth and 15.6% gave birth by caesarean section. Less than one-half of participants (n = 575; 45.5%) initiated breastfeeding within the first hour after birth and the median time to the first breastfeed was 1.5 hours.
Characteristics of Study Participants
1 USD = 7.78 HKD.
Table 2 shows the unadjusted and adjusted associations between antenatal and intrapartum variables, breastfeeding initiation within the first hour, and the time to initiation of the first breastfeed. Results from the adjusted logistic regression analysis show that participants who gave birth from 0700 to 1359 hours had 38% higher odds (aOR = 1.38; 95% CI: 1.001–1.91) of breastfeeding initiation within 1 hour after birth and those giving birth from 1400 to 2059 hours had almost a 60% higher odds (aOR = 1.59; 95% CI: 1.14–2.21) of breastfeeding within the first hour. Opioid pain medication administration (aOR = 0.69; 95% CI: 0.48–0.98), assisted vaginal birth (aOR = 0.51; 95% CI: 0.28–0.90), and caesarean section (aOR = 0.06; 95% CI: 0.03–0.10) were all significantly associated with delayed breastfeeding initiation. Gestational age, birth weight, induction of labor, and epidural analgesia were not significantly associated with early breastfeeding initiation. The goodness-of-fit test for the logistic regression model produced a p value of 0.73, indicating that the model fit the data. VIF values ranged from 1.03 to 6.04, which showed no evidence of multicollinearity.
Unadjusted and Adjusted Associations Between Intrapartum Factors and the Timing of Breastfeeding Initiation in Hong Kong Mothers, 2011–2012
Adjusted for maternal age, maternal educational, household income, parity, antenatal childbirth class(es) attendance, antenatal breastfeeding class attendance, previous breastfeeding experience, intention to exclusively breastfeed, study site, and all variables list in the above table.
CI, confidence interval; HR, hazard ratio; OR, odds ratio.
The unadjusted and adjusted effects of antenatal and intrapartum factors on the time to the initiation of the first breastfeed are also shown in Table 2. In the fully adjusted model, when compared with participants giving birth during the night time (2100–0659), mothers who gave birth from 0700 to 1359 hours were 16% more likely to initiate breastfeeding earlier (adjusted hazard ratio [aHR] = 1.16; 95% CI: 1.004–1.33). Similar to the findings from the logistic regression models, participants who received opioid pain medication (aHR = 0.78; 95% CI: 0.67–0.91) and who had an assisted vaginal birth (aHR = 0.74; 95% CI: 0.57–0.97) or a caesarean section (aHR = 0.30; 95% CI: 0.25–0.36) were more likely to initiate breastfeeding later, while gestational age, birth weight, induction of labor, and epidural analgesia were not associated with the timing of breastfeeding initiation. The log–log plot for the Cox regression model showed that there was no violation of the proportional-hazards assumption.
Figure 1 shows the Kaplan–Meier curves of the time to first breastfeed by whether or not participants experienced a natural birth. Participants who had a natural birth initiated breastfeeding earlier than participants who received any intrapartum intervention (p < 0.001) and the median time to the first breastfeeding was 1 and 2 hours, respectively. In the fully adjusted analysis, natural birth was strongly associated with breastfeeding initiation within the first hour (aOR = 2.69; 95% CI: 2.03–3.56) and with an increased likelihood of earlier breastfeeding initiation (aHR = 1.75, 95% CI: 1.54–1.99) (data not shown).
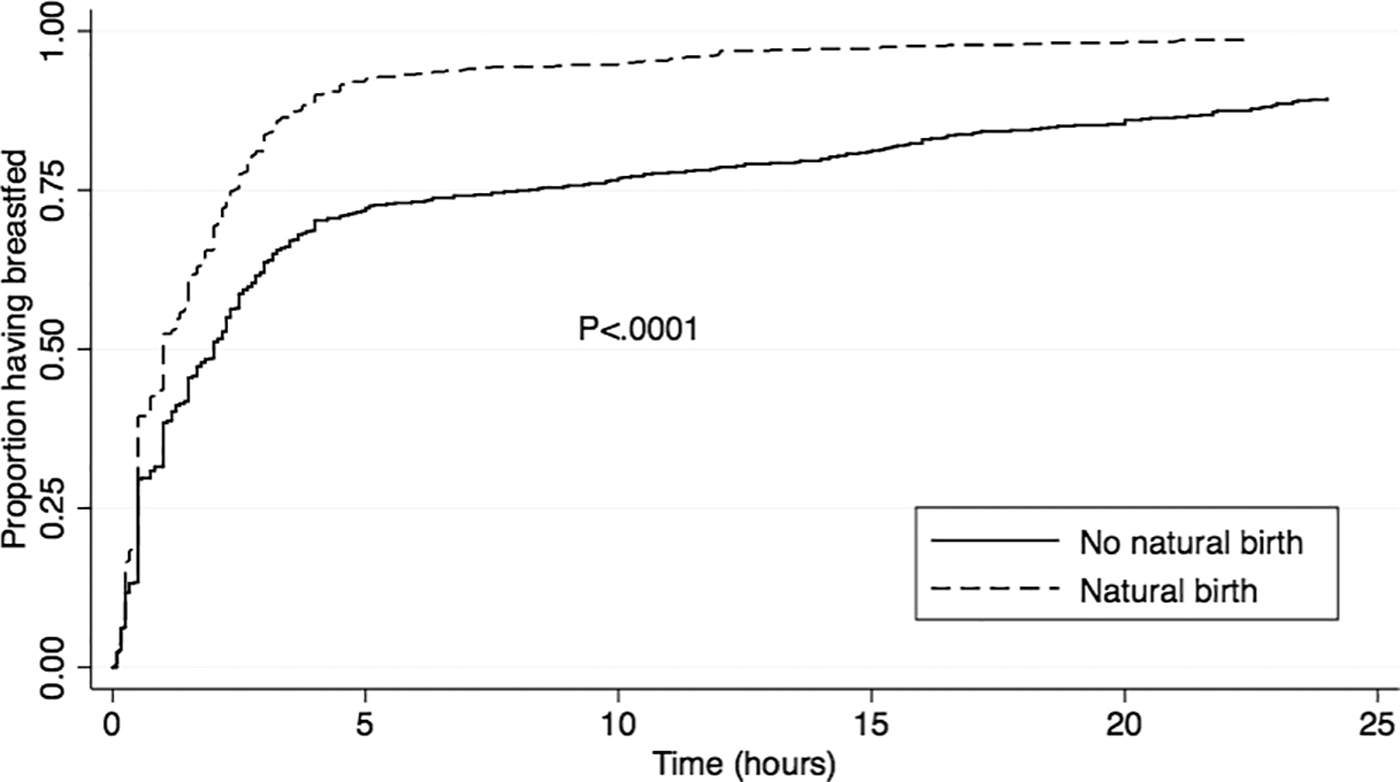
Kaplan-Meier curves of the time to breastfeeding initiation by type of birth.
Discussion
In our study, participants who received opioid medication and who underwent a caesarean section had 31% and 94% lower odds of breastfeeding within the first hour after birth, respectively. Conversely, participants experiencing a natural birth without intrapartum interventions were ∼2 to 3 times more likely to initiate breastfeeding earlier. Gestational age, birth weight, induction of labor, and epidural analgesia did not affect the timing of breastfeeding.
The use of opioid medications for labor pain relief is prevalent, with previous studies reporting that 25–30% of laboring women receive pethidine or similar medications.22,23 Although <20% of participants in this study received opioid pain relief, the drug administered was pethidine (meperidine). While opioid medications can provide pain relief to women in labor, 24 research has shown that meperidine is associated with suboptimal breastfeeding practices, such as delayed suckling behavior of newborns and early breastfeeding cessation. 25 When compared with other opioids such as morphine, the maternal and neonatal half-life of the active meperidine metabolite normeperidine are prolonged.26,27 This results in central nervous system 27 and respiratory depression 28 and interferes with breastfeeding initiation and continuation in the first few days after birth.29,30 Although ACOG recommends that in hospital settings, pharmalogic pain relief should be available if women desire it, 31 they, along with other perinatal professional groups, specifically recommend against the use of pethidine for obstetrical analgesia,31,32 although its use is still common globally. 33
Caesarean birth has also been identified as a predictor of delayed breastfeeding initiation, 34 suboptimal newborn breastfeeding behaviors, 35 and shorter breastfeeding duration. 36 Globally, rates of caesarean section have increased substantially over the past several decades, with rates ranging from 25% in Europe, 32% in the United States, and 40% in Latin America. 37 Although the rate of cesarean birth in this sample was only 15.6%, it was strongly associated with delayed breastfeeding initiation. Operative birth lowered the odds of breastfeeding within the first hour after birth by 96%. In practice, this means that very few mothers who had a cesarean were able to breastfeed within the first hour.
We found no association between the epidural analgesia and labor induction and breastfeeding initiation. A recent review of 23 studies found that the effect of an epidural during labor on breastfeeding was mixed, with only around one-half of the studies (n = 12) reporting that epidural negatively affected breastfeeding. 38 However, in contrast to other countries where the use of epidural or spinal analgesia during labor is more common, 39 only 4.3% of participants in our sample received an epidural. Another systematic review of 38 studies showed that the use of epidural analgesia was associated with a longer second stage of labor and a greater risk of instrumental or caesarean birth. 40 One possible explanation for the inconsistency in various study findings of the effect of epidural analgesia on breastfeeding is that there may be unmeasured confounding factors in women receiving epidural analgesia, especially in settings similar to our study where epidural analgesia is not widely used.
We also found no association between labor induction and the timeliness of breastfeeding initiation, and the existing evidence on the association between Oxytocin use during childbirth is mixed. 41 One study found that when labor is electively induced, breastfeeding initiation rates decrease, suggesting that maternal motivation may be a confounding factor. 42 Although almost 30% of participants in our study had labor induced, in Hong Kong public hospitals, labor induction is only performed in cases with a clear medical indication, including late-term pregnancy, fetal indications, premature rupture of membrane, and maternal complications. 43 Because only healthy mother-infant pairs were recruited into this study, mothers with more adverse perinatal and neonatal outcomes, who required induction, would likely have been excluded and may explain why we found no effect. Similar to epidural analgesia, future studies should try to differentiate the effects of labor induction on breastfeeding versus the conditions that necessitate the induction of labor.
We also found that participants who gave birth during the day or evening were more likely to initiate breastfeeding earlier. We hypothesize that this may be related to fewer available nursing and midwifery staff in the obstetrics units to help mothers initiate breastfeeding during the night shift. This finding is also consistent with other studies reporting an association between night time and weekend birth and early neonatal death.44,45
To our knowledge, this study is one of few studies in high-income countries that have examined factors affecting the timing of breastfeeding initiation. We also examined the effect of natural birth on breastfeeding initiation, something that few other studies have done. Early breastfeeding initiation is strongly associated with breastfeeding duration, so it is important to examine the effect of intrapartum interventions. The major variables in this study, for example, medication use, birth data, and the time of breastfeeding initiation, were obtained from the medical records, thereby increasing the accuracy of the data. Furthermore, as all the data were collected during recruitment in early postpartum period, loss to follow-up was not a concern. We recruited only healthy mother-infant pairs, thus limiting the potential effect of adverse maternal and child health outcomes on breastfeeding initiation.
This study had several limitations. First, there were low rates of some intrapartum interventions in this sample. Only 4.3% and 15.6% participants had epidural analgesia and a Caesarean section, respectively. Although low intervention rates are beneficial for pregnant women, it may have limited our ability to detect associations between the intrapartum interventions and breastfeeding initiation. In particular, epidural analgesia rates were <5% in our sample. Furthermore, we assessed the effect of several intrapartum interventions and many participants likely received multiple intrapartum interventions, thereby complicating the determination of the effect of individual interventions. We also did not have data on skin-to-skin contact after birth, so we were unable to assess if intrapartum interventions impeded immediate skin-to-skin and how this may have affected the timing of breastfeeding initiation. Moreover, our sample was not population based and selection bias may have occurred. The participants in this study had higher maternal education and family income when compared with a previous population-based study. 16 Furthermore, our recruitment was limited to mothers who intended to breastfeed and our participants may have been more motivated to initiate breastfeeding as early as possible after birth. Therefore, the study results may not be generalizable to the larger population.
Conclusion
In a sample of mothers who gave birth to healthy full-term infants, less than one-half of the participants initiated breastfeeding within the first hour. Promotion and support for early breastfeeding initiation should be strengthened in hospitals. Breastfeeding initiation was delayed in participants who had a caesarean birth or who received opioid pain medication, and natural birth was associated with earlier breastfeeding initiation. New mothers who receive intrapartum interventions may need more breastfeeding support to ensure they start breastfeeding after birth as soon as it is safe and feasible. Further research is needed to explore the associations between individual and multiple intrapartum interventions and the time of breastfeeding initiation.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Health and Medical Research Fund (grant 05060721) from the Food and Health Bureau, the Government of the Hong Kong Special Administration Region, the University of Hong Kong (grant 10207306), the University of Hong Kong Strategic Research Theme of Public Health, and the School of Nursing, the University of Hong Kong.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.