
Abstract
Objective:
The ketogenic diet (KD) is a high-fat and restricted carbohydrate diet for treating severe childhood epilepsy. In infants, breast milk is usually fully replaced by a ketogenic formula. At our center, mothers are encouraged to include breastfeeding into the KD if still breastfeeding. This retrospective study describes achievement and maintenance of ketosis with or without inclusion of breast milk.
Methods:
Data were retrieved from a prospective longitudinal database of children treated with KD for epilepsy analyzing infants <1 year of age. The time to achieve clinically relevant ketosis (≥2 mmol/L beta-hydroxybutyrate) was compared with and without inclusion of breast milk into standard KD. Ketosis, nutritional intakes, effectiveness, adverse effects, and successful continuation of breastfeeding were evaluated.
Results:
A total of 79 infants were eligible for analysis. In 20% (16), breast milk was included. Infants with breast milk included into the KD achieved relevant ketosis in 47 hours (interquartile range [IQR] 24–95) compared with 41 hours (IQR 22–70; p = 0.779) in infants with standard KD. Beta-hydroxybutyrate at day 2 was 3.1 mmol/L (IQR 0.5–4.9) and 3.8 mmol/L (IQR 2.2–4.9). Infants with breast milk included received higher amounts of carbohydrates at baseline and calories at 3 months. Seizure freedom and adverse effects showed no relevant differences. No infections occurred in infants receiving breast milk. In two infants, KD was initiated with breast-feds after bottle-feeding KD formula. In 31%, breastfeeding was continued after the KD, and in 25%, inclusion of breast milk and breastfeeding was maintained until complete weaning. Before discharge from hospital, the amount of breast milk included was median 90 mL/day (IQR 53–203) equivalent to median 9% (IQR 6–15).
Conclusions:
Appropriate ketosis was achieved in most infants and maintained within 48 hours. Incorporation of breast milk into KD is feasible, safe, and effective.
Introduction
The ketogenic diet (KD) is a high-fat, low-carbohydrate diet1,2 used for the therapy of drug-resistant childhood epilepsy. 3 With increasing knowledge on the high efficiency of the neonatal brain to metabolize ketone bodies4,5 and availability of specialized ketogenic infant formulas, the KD is increasingly used for the management of intractable epilepsy already in the first year of life.6–9
Exclusive breastfeeding is the optimal form of nutrition during infancy, either exclusively during the first 6 months of life or as central part of a mixed diet later on. To induce and maintain ketosis in KD, only a restricted amount of carbohydrates is tolerated and breast feeding is usually fully replaced by a specialized high-fat ketogenic formula. 10 In view of the considerable physical11–17 and mental 18 health advantages of mother's milk, it nevertheless seems desirable to allow for incorporation of breastfeeding into the KD, the more in a group of patients particularly vulnerable to physical and mental comorbidities.19,20
Until now, there are three case series on the inclusion of breast milk into KD.21–23 At our center, both KD with and without inclusion of mother's milk are well established. Studies that directly compared the effectiveness of a KD with and without breast milk are still lacking. The objective of our study was to retrospectively analyze the feasibility, effectiveness, and safety of a KD regimen that includes breast milk compared to standard KD without breastfeeding in infants younger than 1 year of age.
Methods
Study design
This study is a retrospective database analysis of infants with childhood epilepsy that were treated with a KD at our clinic (Department of Pediatrics, Medical University of Vienna, Austria; September 1999 to December 2018). The KD program at the study center was started in 1999 in toddlers and older children. From 2006 onward, when a readymade ketogenic formula was available in Europe, infants younger than 1 year of age were also included. The study compared conventional KD without breastfeeding with a KD that permitted ingestion of breast milk. Eligible participants were infants <12 months of age fed with an exclusive or mixed liquid diet, but without parenteral nutrition. The primary outcome was time to achieve clinically relevant ketosis. Important secondary outcomes were treatment responder rate and seizure freedom at 3 months and last follow-up visit and the z-score of weight and height after 3 months. Moreover, continuation of breastfeeding, nutritional intake, growth, and adverse effects were analyzed.
Ketogenic diet
The KD was initiated without prior fasting or fluid restriction. 24 Nursing mothers were invited to include their breast milk into the KD. Before initiation of the diet, a thorough neurologic and pediatric examination, video-electroencephalogram, and fasting blood samples were obtained. After consent, the KD was calculated by a trained nutritionist using a computer-based algorithm (Supplementary Fig. S1). The KD was started at a fat/nonfat ratio of 1:1. 24 A ketogenic formula (Ketocal®; Nutricia Metabolics, Erlangen, Germany; fat/nonfat ratio of 3:1 or 4:1) was therefore mixed with either conventional infant formula (fat/nonfat ratio of 0.4:1) or expressed breast milk. For mature breast milk, an average amount of fat, proteins, and carbohydrates was used for calculation (100 mL containing 75 calories, 4.03 g of fat, 1.13 g of proteins, and 7 g of carbohydrates, equating to a fat/nonfat ratio of 0.4–0.6:1).25,26 To optimize the fat content and to maximize the amount of breast milk, mothers were encouraged to provide pumped hind milk. The amounts of ketogenic formula were then increased stepwise to reach a fat:nonfat ratio of 3:1 (maximum)—depending on beta-hydroxybutyrate levels (2–5 mmol/L). When beta-hydroxybutyrate levels were lower or within this range, fat/nonfat ratio was increased on a daily basis in both groups. After reaching stable ketosis, the fat:nonfat ratio was lowered while maintaining ketosis to allow for a maximum amount of ingested breast milk (or formula milk). In the breastfeeding group, transition from pumped mother's milk to breastfeeding was encouraged. In this study, infants were breastfed after bottle-feeding the calculated amount of ketogenic formula. Plasma glucose, beta-hydroxybutyrate, and urine ketone levels were measured three times a day while KD was established. At home, urine ketone levels, seizures, nutrition, and adverse effects were documented in a patient's diary. At each outpatient visit, a thorough pediatric, neurological, and nutritional analysis was performed. Nutritional parameters (fluids, total calories, protein, lipid, and carbohydrate intake) and growth parameters (weight, height, and cranial circumference) were assessed. At outpatient visits, blood analyses included fasting plasma glucose and beta-hydroxybutyrates according to a standardized protocol.3,9,27 Outpatient visits were performed after 1 month and after 3, 6, and 12 months after KD start. For infants not receiving the KD at 3 months, last follow-up on the KD was taken for analysis.
The clinical data of infants with inclusion of breast milk into their KD are displayed in Supplementary Table S1. A detailed individual prescription of a KD that includes breast milk is given in Supplementary Table S2.
Data collection
Data were retrieved from a database of pediatric patients treated with KD. Patients were prospectively enrolled and data entered from medical records and patient's diaries (collected at 1, 3, 6, and 12 months after KD start). The time to clinically relevant ketosis was defined as time (hours) until ≥2 mmol/L blood beta-hydroxybutyrate 27 was reached. The data with statistical analysis are reported in the text (see Results section) and the time course of beta-hydroxybutyrate blood levels (first 5 days and at 1 and at 3 months of therapy) was plotted and reported with the proportion of infants with clinically relevant ketosis (≥2 mmol/L beta-hydroxybutyrate) in Figure 1. The baseline characteristics were recorded as shown in Table 1. Nutritional parameters and growth were documented as shown in Table 3. The z-score differences from initiation of KD to the end of study were calculated and reported in the text (Results section). The effectiveness of therapy is shown in Table 2. Treatment response was defined as a seizure reduction >50% compared to baseline (seizure count through 3 months before initiation of the KD), seizure freedom was defined 100% seizure reduction compared to baseline, if maintained through to the last follow-up visit. Adverse effects were recorded using an adverse effects diary and recorded as shown in Table 4. Low fluid intake was defined as intake 30% below recommendations, 28 growth deficit as a z-score loss of body weight of > −0.8 and excessive weight gain as z-score increase of >1.6. A sample of a prescription of a typical patient's KD that included breast milk is shown with the amounts of breast milk in Supplementary Table S2. For data entry into the database parental consent was obtained. Data collection and analysis were approved by the Ethics Committee of the Medical University of Vienna (EK.-Nr. No. 1391/2013; EK-Nr. 1591/2019).
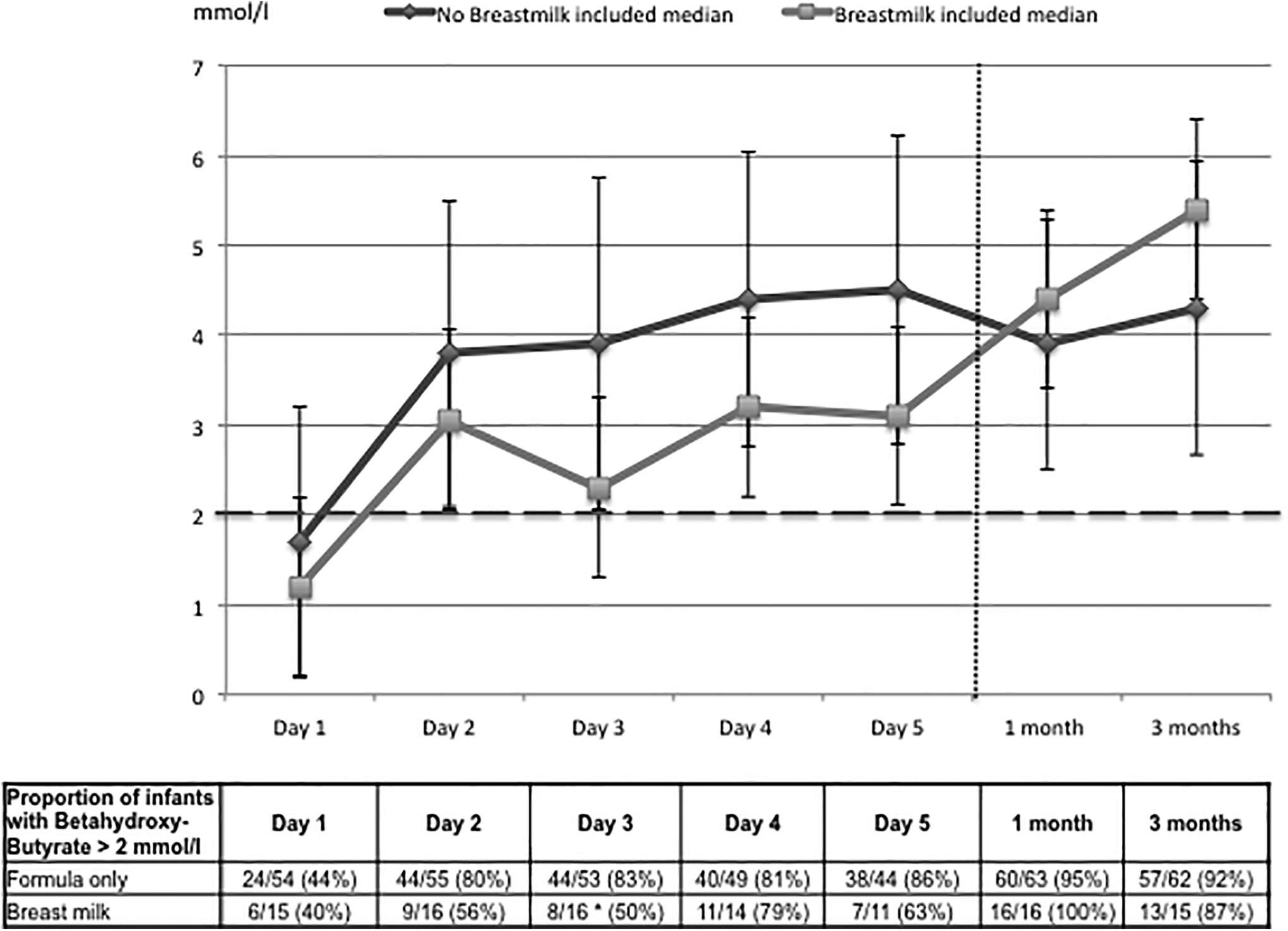
Ketone levels and relevant ketosis (mmol/L). The time course of ketosis is shown as the trajectories of the serum beta-hydroxybutyrate levels (day 1 to 5 and at 1 and 3 months; median and standard deviation) and the percentage of infants achieving a clinically relevant ketosis (>2 mmol/L beta-hydroxybutyrate) (p = 0.008 at day 3). *p < 0.01, tested using the chi-square test.
Baseline Characteristics
Categorical data are presented as numbers with percentages in parentheses (tested using the chi-square test). Continuous data are presented as the median and interquartile range in squared brackets (tested using the k-sample median test).
AEDs, antiepileptic drugs; KD, ketogenic diet.
Effectiveness
Categorical data are presented as numbers with percentages in parentheses (tested using the chi-square test), and the odds ratio between groups with 95% CIs in parentheses.
Data of one patient missing.
Data of two patients missing.
CI, confidence interval.
Nutritional Parameters
Continuous data are presented as medians with interquartile range in squared brackets (tested using the k-sample median test) and median estimator between groups (Hodges–Lehman) with 95% CIs in parentheses.
p < 0.05.
p < 0.01.
CI, confidence interval.
Adverse Effects
Data are presented as numbers with percentages in parentheses (tested using the chi square test).
During the first week of the KD.
During the first 3 months of the KD.
KD, ketogenic diet.
Data analysis
Statistic data description was used as appropriate (frequency, median, interquartile range [IQR], range). For comparisons between groups, medians, odds ratios, confidence intervals, and Pearson's chi-square, k-sample median test and the median difference estimator (Hodge–Lehman) were used as appropriate. For infants not receiving the KD at 3 months, the last follow-up visit on the KD was used for analysis. Data analysis was performed using the IBM Statistical Package for Social Science (SPSS Statistics Version 25). The significance level was set at p ≤ 0.05. The hypothesis to be investigated was that the time to achieve clinically relevant ketosis was similar in infants in whom breast milk was continued during treatment with a KD compared with infants treated with KD alone.
Results
Patient characteristics
A total of 201 children were screened and 83 patients ≤1 year of age were identified. Four infants were excluded (KD started while receiving parenteral nutrition). The whole final cohort consisted of 79 participants. The age when the KD was started was 6.2 months (median; IQR: 4.4–8.4 months; range: 14.6 days–12.0 months) with a majority of infants (63/79; 80%) already receiving exclusively formula and less infants being breastfed (16/79; 20%; exclusively: 10/79; 12.7%; partially: 6/79; 7.6%). Upon invitation to include breast milk into their infants KD, all mothers decided to do so. Infants on formula received standard KD by default. More infants were male (47/79; 69%). The etiology of epilepsy was unknown in every third infant (31/79; 30%). The KD was the first antiepileptic therapy in a small minority of infants (10/79; 13%): most infants (69/79; 87%) received antiepileptic drugs (AED) before KD initiation. In this study, the amount of concomitant AEDs at initiation of KD was two (median; range: IQR: 1–2, range: 0–4). The amount of previously used AEDs until the KD was started was two (median; IQR 1–3, range: 0–12). The median duration of KD was 10.7 months (IQR 5.7–20.5 months; range: 0.4–74). Baseline characteristics of participants by group are shown in Table 1. The z-scores of body weight at baseline were significantly higher in infants who received breast milk. Other parameters did not differ significantly. The median duration of KD was 10.1 months (IQR: 7.0–25.8 months).
Ketosis and treatment effectiveness
The time to achieve clinically relevant ketosis did not differ significantly between groups (p = 0.78). Ketosis was reached in infants with breast milk after 47 hours (median; IQR: 24–95 hours), in infants without breast milk after 41 hours (median; IQR: 22–70 hours). The proportion of infants with a beta-hydroxybutyrate level >2 mmol/L (defined as clinically relevant) was significantly lower in infants with inclusion of breast milk on the third day of the KD only (Fig. 1). Two infants in the group without breast milk failed to achieve clinically relevant ketosis (beta-hydroxybutyrate levels: 0.2–0.9 and 0.2–1.8 mmol/L) and three infants achieved clinically relevant ketosis as late as after 8, 9, and 15 days, because of medications containing small amounts of carbohydrates, which was detected and resolved. The time-course of beta-hydroxybutyrate levels was not significantly different between both groups (Fig. 1). The KD was equally effective in both groups. About two thirds of infants showed seizure reduction by more than half, and in about a third of infants, seizures ceased completely (Table 2).
Nutritional intake and growth
Infants who were breastfed at baseline received a lower fat:nonfat ratio and significantly more carbohydrates (Table 3). After KD was implemented, infants who received breast milk in their KD consumed significantly more energy (difference between medians of 7 kcal, p = 0.044). Individual data of infants who received a KD with breast milk are displayed in Supplementary Table S1. The main type of epilepsy was West Syndrome (14/16) of varying etiology. On the first day of the KD, infants who also received breast milk received 144 mL of mothers' milk (median; IQR 90–307 mL/day, min. 34 mL–max. 600 mL), which was 30% (median; IQR 6–50%) of liquid meals (fat/nonfat ratio: 1.83:1; median; IQR 1.5–2.5). On day 3, the amount of breast milk included was 90 mL (median; IQR 53–203 mL/day, min 24 mL–max. 260 mL), which was 9% (IQR 6–15%, range 3–38%) of liquid meals. The fat/nonfat ratio of liquid meals was median 2.48:1 (IQR 2.01–2.6). The median duration of including breast milk was 127 days (IQR: 17–166 days; range: 7–482 days). An example of a ketogenic prescription is given in Supplementary Table S1.
Growth (z-score difference for weight and height from baseline to last follow-up) was not significantly different between the two groups: difference z-score of weight: 0.08 versus 0.25 (median, 95% CI: −0.28 to 0.76; p = 0.82), difference z-score of height: −0.22 versus 0.48 (median, 95% CI: −0.41 to 1.22; p = 0.43).
Feasibility
Eight out of 16 (50%) mothers who started to include breast milk into the KD continued to provide breast milk for more than 3 months. Five mothers (31%) provided breast milk less than a month (stopped after 7, 8, 10, and 10 and 19 days). Five mothers (31%) managed to nurse their infants on the KD, with three mothers who switched to breastfeeding after pumping milk at the start of KD and two mothers who nursed from the first day of the KD. Four mothers (25%) provided breast milk until weaning without switching to infant formula.
Adverse effects
There was no significant difference in total adverse effects (Table 4). Constipation and low fluid intake was as the most frequent adverse effect in both groups. Intermittent high triglycerides at 3 months were observed in up to 30% of infants.
Discussion
The KD is a well-established diet for severe early-onset epilepsy syndromes.3,9 The present article reports for the first time the feasibility, effectiveness, and safety of a KD that includes breast milk compared to the conventional exclusively formula-based approach in infants. Clinically relevant ketosis was typically achieved within the first 48 hours of therapy and maintained throughout the KD. A higher caloric intake after 3 months of therapy was observed in infants with KD where breast milk was included.
Effectiveness of the KD at 3 months was high in both groups: infants with breast milk showed response in 67% and seizure freedom in 40%; infants without breast milk showed response in 70% and seizure freedom in 27%. The most frequent adverse effects were low fluid intake and constipation in both groups. However, during the first 3 months no infections occurred in infants receiving breast milk compared to infants without breast milk included. The microbiome in mother's breast milk and areolar skin shapes the infant's gut in early life, underscoring the importance of breastfeeding in the maturation the infants gut microbiome, which has implications on infections and immunity.29,30
In addition, the higher carbohydrate intake and lower fat/nonfat ratio was reflected by a lower percentage of hypoglycemia and high lipids in infants with breast milk included. Also, a higher percentage of KD refusal and constipation seen in this group might reflect a flavor preference for breast milk due to the mixed feeding of KD formula and breast milk and a greater nutritional change.
In two infants, KD was initiated with feedings at the breast after bottle-feeding the KD formula, and in five infants, breastfeeding was successfully continued after the KD was stopped.
Breastfeeding is the normative standard for infant nutrition, providing healthy growth and development, recommended exclusively during the first 6 months and advised to be continued up to 1 year of age or beyond while gradually introducing solid foods. 31 Breast feeding as well as including pumped breast milk does not only provide macro- and micronutrients but also promotes intestinal, immune, and cognitive development. 32 In infants with inborn errors of metabolism such as phenylketonuria33,34 breast milk on demand is frequently included after having given a small amount of specialized formula when close clinical and metabolic monitoring is guaranteed. 35
The prescription of the KD allows only very restricted amounts of carbohydrates, so that the inclusion of breast milk is difficult, let alone the continuation of breastfeeding. In the previously reported case series,21–23 feeding at the breast while on KD was described in 3 cases, 21 and expressed breast milk was used in the other 14.22,23 Also in our cohort, two infants were exclusively breastfed: the allowed amount of breast milk was fed at the breast after the calculated amount of ketogenic formula to guarantee the calculated fat/nonfat ratio. However, most mothers in our cohort preferred to express breast milk. Regardless of the beneficial properties of pumping human milk, infants fed with pumped milk have been recently described to show a different and less diverse microbiome than breastfed infants, 36 so that breastfeeding while on the KD should be encouraged.
As described in the study by Cole et al., 21 fat/nonfat ratios were lower also in our patients who received breast milk, which was also confirmed by a higher amount of calories per day at 3 months. A gradual introduction and a modified fat/nonfat ratio of 2:1 up to 2.5:1 allowed us to keep a high amount of breast milk integrated in the KD while maintaining ketosis.
Finally, including breast milk during KD in infants with epilepsy allows for achieving stable ketosis and maybe to maintain some the health benefits of breast milk as well as mother–infant bonding.
Our data show the feasibility of including expressed breast milk into the KD and to maintain breast-feeding—even until weaning in 25% of patients. Treatment response (i.e., reduction in seizure frequency, as well as seizure freedom) is in accordance with infants on standard KD.6,7,9,37,38 The higher percentage of seizure freedom in infants with breast milk included, although not significant, might reflect the documented epidemiological association of breastfeeding with a decreased risk of epilepsy. 39 On the contrary, infants with a KD that included breast milk were slightly younger and received less AEDs than infants without breast milk, which also favors a better response to therapy. 6 This potential additional benefit of breast milk on the effectiveness of the KD still remains to be studied, in particular with regard to developmental and cognitive long-term outcome.
Strength and limitations
This is the first study that directly compared a KD with breast milk included to the standard KD that is exclusively based on formula. In addition, we analyzed the largest group of infants (n = 16) and described in detail how to achieve ketosis and maintain feeding at the breast, however, in a cohort of 79 infants, this is a relatively small sample for subgroup analysis. The fact that ketosis can be achieved in most patients within the first 48 hours is promising: Data are, however, still very limited, especially on mothers actually nursing their children while on the KD. Since the team has gained experience in including breast milk to the standard KD during the study period, protocols changed insofar as in the last year's nursing while on the KD was accepted by mothers earlier, that is, already from the first day of the KD.
Summary and Conclusions
Our results show that ketosis and hence seizure control is feasible with inclusion of breast milk into the KD. We also show that continuing nursing while implementing the KD is complicated for both team and mothers and only achieved in a minority. Effectiveness and safety are not different. However, infections do not occur when breast milk is included.
Based on our results, we suggest to aim at continuation of breastfeeding at start of the KD by bottle-feeding the ketogenic formula and to feed the remaining amount of tolerable carbohydrates at the breast—as recommended also for inborn errors of metabolism such as phenylketonuria.33–35
Future research should focus on the question how to further optimize the composition of human breast milk, for example, by using hind milk to allow for even higher amounts of breast milk and booster the fat/nonfat ratio. Moreover, long-term beneficial effects of breast milk with respect to growth, cognitive development, and effects on the gut microbiome are to be explored in future studies.
Footnotes
Disclosure Statement
A.D. has received travel reimbursement and speaker honoraria from SHS, Nutricia, and Vitaflo; P.T.-S. has received travel reimbursement from SHS, Nutricia, and Vitaflo. M.F. received travel reimbursement from SHS, Nutricia. None was related to this article. The other authors have no conflicts of interest to disclose.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.