
Abstract
Background:
An exclusive human milk (EHM) diet in extremely low birth weight (ELBW) infants (birth weight ≤1,000 g) is linked to an increased likelihood of extrauterine growth restriction (EUGR, weight <10% at discharge). Past studies associated EUGR with worse neurodevelopmental (ND) outcomes; however, its impact when an EHM diet is used is unknown.
Objective:
Determine whether EUGR adversely affects 2-year ND outcomes of ELBW infants fed an EHM diet. Secondary aims were to compare short-term morbidities and growth through 2 years corrected age (CA).
Materials and Methods:
Prospective cohort study of ELBW infants fed an EHM diet until 34 weeks corrected gestational age and assessed at 2 years CA. ND outcomes between EUGR and non-EUGR infants were compared using the Bayley Scales of Infant Development 3rd Ed (BSID-III).
Results:
Eighty-one ELBW infants survived, 44 were seen for follow-up, and 16 (36%) were EUGR. Baseline characteristics and Neonatal Intensive Care Unit (NICU) morbidities were similar. There were no statistically significant differences (median [25–75%]) between EUGR and non-EUGR groups in cognition, (90 [80–99] versus 95 [90–104]), language (84 [68–105] versus 89 [75–100]), or motor composite scores (87 [74–96] versus 91 [88–96]). Weight z-scores during NICU stay dropped in both groups, more pronounced for the EUGR infants. There was no difference in linear or head growth.
Conclusion:
In our institution, ND outcomes at 2 years CA for ELBW infants fed an EHM diet were similar regardless of EUGR status. This suggests a neuroprotective effect of EHM diet in the ELBW population, despite weight gain velocity during NICU stay.
Introduction
The American Academy of Pediatrics recommends exclusive breastfeeding for the first 6 months of life for all infants, especially those born preterm. 1 In preterm infants, breast milk decreases the incidence of necrotizing enterocolitis (NEC), bronchopulmonary dysplasia (BPD), sepsis, and retinopathy of prematurity (ROP).1–3 For all neonates, and especially preterm infants, mother's own milk (MOM) is recommended as first line of nutrition. However, if MOM is not available, pasteurized donor human milk (PDHM) is the second best dietary option. Both have been associated with a decreased incidence of NEC compared to preterm formula only.1,4,5
An exclusive human milk (EHM) diet consists of only MOM and/or PDHM and human milk-derived human milk fortifier (HUM). Studies have shown that preterm infants who receive an EHM diet have slower growth than those fed preterm formula and are therefore at higher likelihood of experiencing extrauterine growth restriction (EUGR: weight ≤10th percentile for corrected gestational age (CGA) if appropriate for gestational age at birth) at the time of Neonatal Intensive Care Unit (NICU) discharge (DC).4,6,7 Ehrenkranz et al. found that slower growth velocity of extremely low birth weight (ELBW) infants in the NICU was associated with poorer neurocognitive outcomes at 18–22 months corrected age (CA). 8
However, preterm infants fed human milk have improved neurodevelopmental (ND) outcomes when compared to those fed preterm formula.9–12 Magnetic resonance imaging studies of preterm infants at term equivalent demonstrate improved connectivity and white matter microstructure in those who receive an EHM diet for ≥75% of their NICU stay. 13 Therefore, we hypothesize that the risks of slower growth velocity in preterm infants fed an EHM diet may be ameliorated by both reduction in neonatal morbidities and the potential direct neuroprotective or neuropromoting effects of human milk.
The aim of our study was to compare the ND outcomes at 2 years CA, measured by the Bayley Scales of Infant and Toddler Development 3rd Ed. (BSID-III) between EUGR and non-EUGR ELBW infants fed an EHM diet until 34 weeks CGA. Secondary aims were to compare differences in growth velocity until 2 years CA between the groups.
Materials and Methods
Patient population
This is a prospective cohort study of inborn and outborn ELBW infants who were admitted within 24 hours of life to the Maria Fareri Children's Hospital Level IV NICU from February 2015 to September 2016 and seen through 2 years CA at the affiliated Regional Neonatal Follow-up Program. We excluded infants with major congenital anomalies or genetic disorders that would impact growth or neurodevelopment, and any infant who received formula or bovine-based fortifier (BOV) before 34 weeks CGA. Demographic and clinical data were collected from the medical records and parental report. The study was approved by the New York Medical College and Westchester Medical Center Institutional Review Boards.
Nutrition protocol
All infants received an EHM diet until 34 weeks CGA, including oral care with mothers' own colostrum/breast milk or PDHM from the first hours of life until the first oral feed, MOM, PDHM, and HUM (Prolacta+H2MF; Prolacta, Duarte, CA). All mothers received antenatal and postnatal lactation support. Infants received MOM first line and PDHM was given only if MOM was contraindicated, or available in insufficient quantities to meet the baby's needs.
Total parenteral nutrition (TPN) was given from birth with protein 3 g/kg/day, fat 1 g/kg/day, and dextrose 6–8 g/kg/day. Protein and fat were each increased by 1 g/kg/day until 4 g/kg/day and 3 g/kg/day, respectively. Dextrose was increased by 1 g/kg/day to a goal of 9–10 g/kg/day. With this rapid advancement, TPN provided 90 kcal/kg/day by day 3 of life. Trace elements, vitamins, calcium, and phosphorus were adjusted based on laboratory results. TPN was continued until enteral feeding volume reached 120 mL/kg/day.
Enteral feeds were initiated by day 0–2 at trophic volumes of 20 mL/kg/day and increased by 20 mL/kg/day as clinically tolerated to goal feeds of 160 mL/kg/day (>120 kcal/kg/day). Standard fortification with Prolacta+H 2 MF to 24 kcal/ounce was initiated at enteral feeding volume of 80 mL/kg/day and advanced to 26 or 28 kcal/oz at the clinician's discretion, based on growth.
At 34 weeks CGA, the diet was modified as follows: infants continued to receive MOM as available. HUM was changed to BOV fortifier (Enfamil Human Milk Fortifier, Acidified Liquid; Mead Johnson Nutrition, Chicago, IL). PDHM was replaced with 22 kcal/ounce preterm formula.
Short-term outcomes
NICU morbidities impacting growth and neurodevelopment were compared between EUGR and non-EUGR infants. The following definitions were used: BPD: need for any respiratory support at 36 weeks CGA; severe ROP: stage 3/higher or laser therapy; severe intraventricular hemorrhage (IVH): Papile's grade 3/4 or periventricular leukomalacia (PVL); NEC: pneumatosis confirmed on abdominal X-ray; sepsis: positive blood or cerebrospinal fluid culture; and patent ductus arteriosus (PDA): surgical ligation after failed medical treatment for hemodynamically significant PDA. 14
Growth
Anthropometrics (weight, head circumference [HC], and length) were recorded at three distinct time periods: birth, NICU DC, and 2 years CA. An electronic digital scale (Scale-tronix® Pediatric/Infant Scale 4800; Welch Allyn®, Skaneateles Falls, NY), paper tape measure, and a plastic length board (Premie Stadiometer; Ellard Instrumentation Ltd, Monroe, WA) were used accordingly. z-Scores based on gestational age (GA) at birth, CGA at DC, and CA at 2 years were generated from the 2013 Fenton Growth Chart, the WHO Growth Chart (if older than 50 weeks CGA), and the CDC Growth Chart (if >24 months CA).15–17 NICU growth velocity (g/kg/day) was calculated from birth to DC and from time of regaining birth weight to DC using the exponential method. 18
Small for gestational age (SGA) infants (birth weight <10%) were classified as EUGR only when both DC weight <10% and weight z-score change >−2.0 were present. SGA infants who achieved “catch-up growth,” with either DC weight >10% or DC <10%, but change in z-score <−2.0 were defined as non-EUGR.
ND outcome
ND assessment with BSID-III was performed at 24 months (±6 months) CA at the Regional Neonatal Follow-up Program by a certified psychologist. 19 Composite cognitive, language, and motor scores for the infants' CA, as well as the developmental age (DA) for all subtests (fine/gross motor and expressive/receptive language) were determined. Moderate neurodevelopmental impairment (NDI) was defined as (1) BSID-III composite cognitive score <85, (2) bilateral blindness, (3) bilateral deafness, or (4) cerebral palsy. Severe NDI was defined as a BSID-III cognitive score of <70 or any of the above-mentioned impairments. To describe the degree of delay in each domain of the BSID-III, a developmental age difference (ΔDA) was calculated, where ΔDA = DA − CA. A negative difference indicates a lower than expected DA performance compared to CA.
Statistical analysis
Demographic characteristics, short-term NICU, and ND outcomes were compared between EUGR and non-EUGR groups utilizing chi-square or Fisher's exact test for categorical variables, and t-test or Mann–Whitney U test for continuous variables, as appropriate. Differences in growth changes over time within each group were assessed with paired t-test or Kruskal–Wallis test and changes in growth between the EUGR/non-EUGR groups were compared with unpaired t-test or Mann–Whitney U test. A p-value <0.05 was considered statistically significant. SPSS version 16.0 was used for data entry and analyses (SPSS, Inc., Chicago, IL).
Results
During the study period, 90 ELBW infants survived to DC. Nine were excluded: seven infants received formula before 34 weeks CGA and two were diagnosed with congenital anomalies. One died after DC, but before 2 years CA and was counted as lost to follow-up. ND assessment was performed on 44 of 80 eligible infants (55%): 16 (36%) were EUGR and 28 (64%) were non-EUGR (Fig. 1). To ensure study infants were representative of the entire ELBW cohort, despite loss to follow-up, we compared maternal sociodemographic and health characteristics, perinatal conditions, neonatal morbidities, and NICU growth patterns between infants who underwent ND assessment and those who did not (Table 1). We found no differences between infants who returned for follow-up and those who did not.
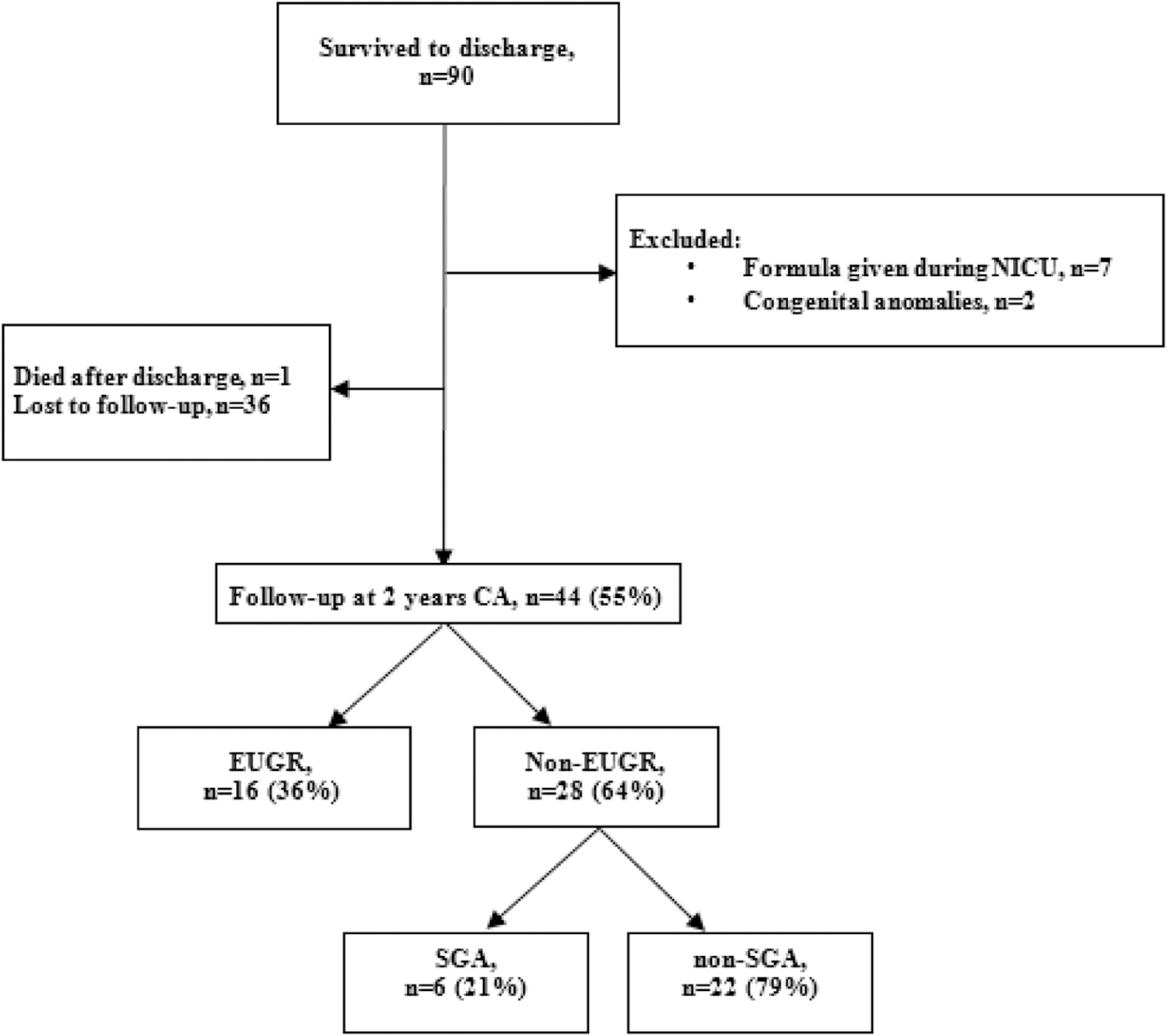
Flow diagram of internal and external patients.
Demographics of Infants with 2-Year Follow-Up Versus Those Lost to Follow-Up
BW, birth weight; CGA, corrected gestational age; DC, discharge; DOL, day of life; FU, follow-up; GA, gestational age; HC, head circumference; IQR, interquartile range; IVH, intraventricular hemorrhage; MOM, mother's own milk; NEC, necrotizing enterocolitis; PDA, patent ductus arteriosus; PVL, periventricular leukomalacia; ROP, retinopathy of prematurity; SD, standard deviation; SGA, small for gestational age; TPN, total parenteral nutrition.
In the study population, we compared differences between EUGR and non-EUGR groups in maternal sociodemographics, co-morbidities, and pregnancy complications, which may impact the infant's growth or neurodevelopment. There were no differences in socioeconomic characteristics between EUGR versus non-EUGR groups, including two parent home (88% for each group), maternal high school education or greater (88% versus 92%), private insurance coverage (44% versus 46%), or primary language other than English in the home (19% versus 25%). We found no differences in maternal ethnicity or maternal age (Table 2). There was no difference in the incidence of pre-eclampsia (13% versus 18%), premature prolonged rupture of membranes (≥18 hours) (31% versus 25%), or antenatal neuroprotective magnesium administration (81% versus 64%).
Maternal/Neonatal Demographics and Short-Term Morbidities
BPD, bronchopulmonary dysplasia; CGA, corrected gestational age; DC, discharge; EUGR, extrauterine growth restriction; GA, gestational age; HC, head circumference; IQR, interquartile range; IVH, intraventricular hemorrhage; NEC, necrotizing enterocolitis; PDA, patent ductus arteriosus; PVL, periventricular leukomalacia; ROP, retinopathy of prematurity; SD, standard deviation; SGA, small for gestational age.
As seen in Table 2, there was no difference between the groups in the GA or perinatal factors. Although not statistically significant, the EUGR infants were smaller at birth, but had similar HC. EUGR infants had a slower growth velocity overall from birth to DC (Supplementary Table S1). Both groups re-gained birth weight by 7 days of life. Although complications of prematurity are often associated with poorer growth velocity and a higher incidence of EUGR, we did not find a difference in the incidence of BPD, sepsis, NEC, IVH/PVL, or ROP (Table 2).
The average CA at the time of ND assessment was 25.7 months (Table 3). Six infants were evaluated outside the goal age range of 24 ± 6 months CA (two EUGR and four non-EUGR). The scores of the infants were similar to those screened within the appropriate range, and therefore the results of all were included in the analysis. For both groups, the median composite scores for cognition, language, and motor function were within normal range, although less than the standardized mean of 100. There was no statistically significant difference between the EUGR and non-EUGR infants for any composite score (Table 3).
Neurodevelopmental Outcomes at 2 Years Corrected Age
CA, corrected age; CP, cerebral palsy; ΔDA, developmental age in months-assessment age in months; EUGR, extrauterine growth restriction; moderate NDI, composite cognitive score <85, CP, deafness, and/or blindness; N/A, not available; NDI, neurodevelopmental impairment; SD, standard deviation; severe NDI, composite cognitive score <70, CP, blindness, and/or deafness.
The DA was lower than the CA for all subtests of the BSID-III, as demonstrated by a negative ΔDA for each subtest (Table 3). However, the EUGR and non-EUGR infants had similar ΔDA, signifying similar degrees of deviation from that expected for CA. The incidence of moderate and severe NDI between the two groups did not differ.
The EUGR infants had significantly greater weight z-score changes and lower DC weight z-scores (Fig. 2). However, both groups demonstrated catch-up growth between DC and 2 years CA. This was more pronounced in the EUGR group, resulting in no difference in weight z-score at 2 years CA. HC and length showed no difference at any time point between those who were EUGR or non-EUGR.
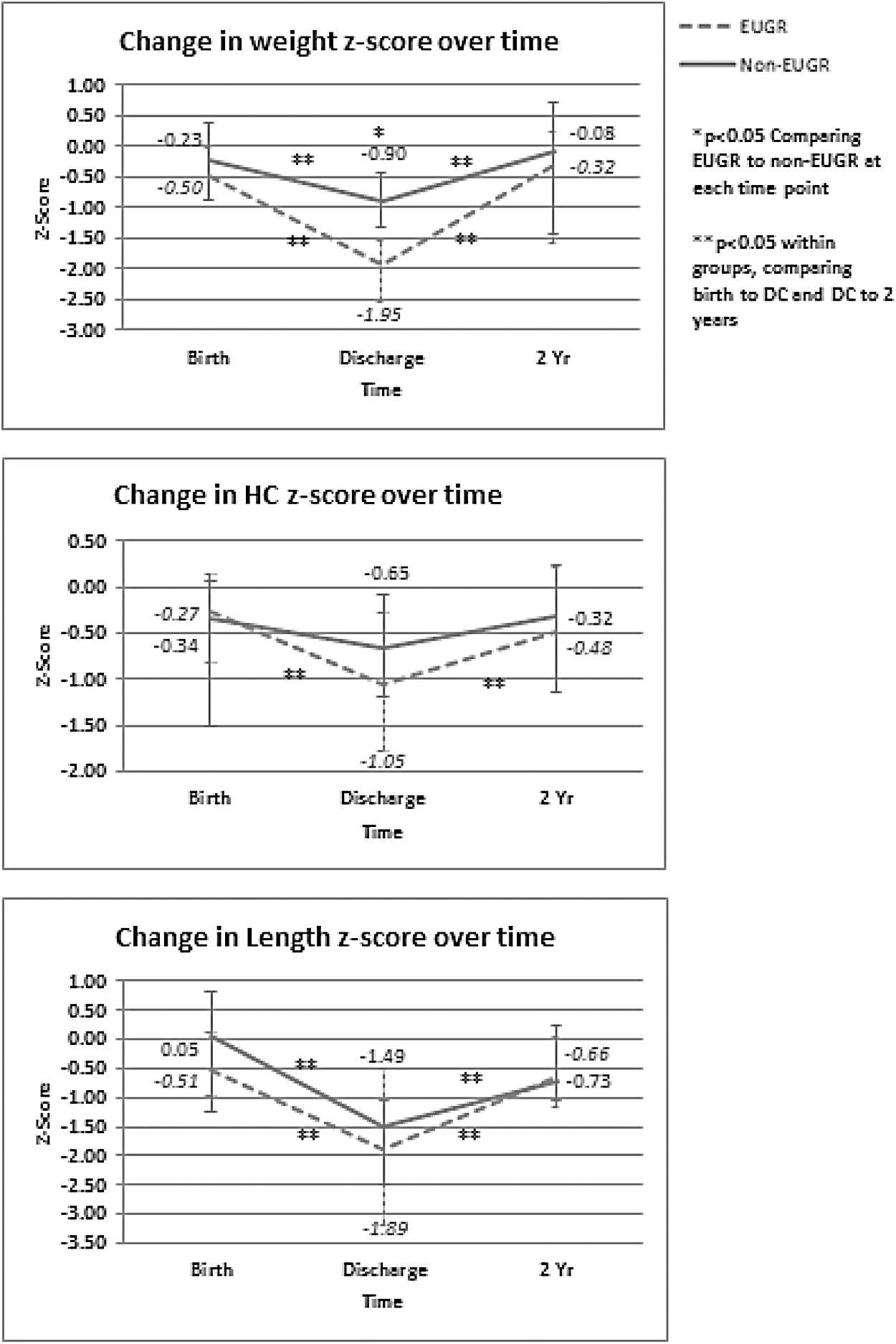
Changes in anthropometrics over time.
Nineteen infants received only MOM, 23 received a mixed diet of MOM and PDHM, and 2 infants received exclusively PDHM, until 34 weeks CGA. There was no difference in weight gain between those fed MOM (13.3 ± 1.9 g/kg/day) compared to a mixed/PDHM diet (12.8 ± 1.9 g/kg/day). There was no difference in ND outcomes for any subtest of the BSID-III based upon the type of milk used.
There were six SGA infants in our cohort. All were included in the non-EUGR group. DC weight for all remained <10%, but they had similar growth velocity to non-SGA infants (14.4 ± 2.2 versus 12.8 ± 1.8 g/kg/day, respectively), and therefore a weight z-score change of <−2.0, resulting in none that met the definition of EUGR, despite being born small. There was no difference in the ND outcome between the SGA infants and non-SGA infants (cognitive score (mean ± SD) 85 ± 17 versus 93 ± 13, language score 86 ± 18 versus 88 ± 17, and motor score 83 ± 19 versus 89 ± 15).
Post hoc sensitivity analysis was done in which the SGA infants were excluded from the study group, and there remained no difference in the composite outcomes between the two groups for composite cognitive score (mean ± SD) (88 ± 15 versus 96 ± 11), language (86 ± 20 versus 89 ± 15), or motor function (84 ± 21 versus 93 ± 7).
Discussion
This is the first study to explore the specific relationship between EUGR in the NICU among ELBW infants fed an EHM diet and ND outcomes. In our cohort of infants who received an EHM diet until 34 weeks CGA, we did not find that EUGR had a significantly negative impact on ND outcomes at 2 years CA.
Weight gain is often used as a marker of appropriate growth, and linked to ND outcomes. However, most studies exemplifying this relationship were done in historical cohorts of patients fed a diet including preterm formula, and not according to current nutritional recommendations.20,21
More recent studies that utilize a breast milk diet show varying results. Maruyama et al. found growth velocity was related to NDI among very low birth-weight (VLBW: <1,500 g) infants only in infants with the slowest growth velocity (<8 g/kg/day), and not among infants fed an EHM diet. 22 Similar to our results, Rozé et al. examined the ND outcome of VLBW infants discharged home on exclusive MOM and found the likelihood of NDI at 2 or 7 years of age was reduced, despite slower overall weight gain during hospitalization, although the role of EUGR was not specifically evaluated. 23 Leppänen et al. evaluated the association of postnatal growth in VLBW infants fed breast milk and cognitive outcomes. They found that, although postnatal growth was associated with cognitive outcomes for appropriate for gestational age (AGA) infants, only HC growth velocity impacted the results for both AGA and SGA infants. 24
These studies support our findings that the role of growth velocity as expressed by weight gain alone may not relate to neurodevelopment in those fed an EHM diet. We likely did not see a difference between EUGR and non-EUGR cohorts, in part, because we did not have a difference in HC or length between them. Recent studies have demonstrated that other anthropometrics, such as length, HC, or fat-free mass may be more predictive of future neurodevelopment than weight gain. 25
Although our sample size is small, and from a single center, our results correlate with others who have assessed the ND outcomes of ELBW and VLBW infants fed an EHM diet. In a cohort of VLBW infants fed EHM supplemented with PDHM, O'Connor et al. reported average scores on the Bayley-III at 18 months CGA for cognition, language, and motor of 92.9, 87.3, and 91.8 respectively. 26 Similarly, Vohr et al. found that, in a cohort of ELBW infants fed >80% human milk, at 30 months CGA, mean Bayley-II scores for Mental Developmental Index and Psychomotor Developmental Index were 89.7 and 90.2, respectively. 11
In our study, although both groups regained BW by DOL 7, likely due to our aggressive TPN strategy, neither group gained weight at the goal rate of the “reference fetus” (15 g/kg/day). 20 It is believed that ideal weight gain for a prematurely born infant should match fetal growth, but this is often unattainable, and may not be beneficial.
Weight gain slower than the “reference fetus” is often attributed to suboptimal macronutrient/caloric intake to meet the increased metabolic demands associated with prematurity. PDHM (mostly donated by mothers of full-term infants) is often associated with slower growth due to lower macronutrient and caloric content compared to milk from mothers of preterm infants. 6 As a result, there is some concern that this will lead to NDI.26,27 However, we found no difference in the growth velocity or the incidence of cognitive, motor, or language delay or NDI between those infants fed exclusive MOM versus those who contained a mixed diet of MOM and PDHM.
An EHM diet likely has independent neuroprotective effects for the ELBW infant, which may outweigh the potential negative effects of lagging weight gain. Breast milk provides many bioactive factors, including antibodies, hormones, and enzymes, which may be neuroprotective or neuropromotional. Human milk's oligosaccharides, found in both MOM and PDHM, provide numerous prebiotics, which may preserve or promote brain development. 28 Long-chain polyunsaturated fatty acids have been shown to play an important role in brain development and growth.29,30 Although pasteurization alters the nutritional composition of breast milk, many bioactive factors remain intact, which may help reduce inflammation and brain injury. 31
Although increased NICU morbidities often result in slower growth, we did not find a difference in the incidence of short-term NICU morbidities between the two groups. This may have been, in part, due to the overall low incidence of morbidities in our cohort compared to national referenced data, likely secondary to the benefits of an EHM diet, to which all were exposed until 34 weeks CGA. 32
A major limitation is a sample size and follow-up rate of 55%. However, other studies that have provided insightful information of nutrition and growth have been published, despite small numbers. 33 High attrition rates have been demonstrated among many longitudinal follow-up studies. 34 We are confident that our study population is a representative sample of the entire ELBW cohort as there were no differences between baseline characteristics or neonatal morbidities between those who did or did not follow up.
Still, because of our limited sample size, we interpret our results with caution. Post-hoc power analysis determined that our study is adequately powered to identify a difference of 13 points on the Bayley-III (∼1 standard deviation). Further studies with larger sample sizes are needed to determine if more subtle differences exist between these populations. Some studies have suggested that a difference as small as five points may create clinically significant difference in a child's abilities; the longevity of these differences remains unknown.35,36
That being said, the 2-year BSID-III is commonly utilized among preterm infants as a marker of long-term developmental outcomes. It is important to note that the impact of neonatal interventions has only been shown to diminish with increasing age. Schmidt et al., for example, found a neuroprotective benefit of caffeine at 18–21 months, which was lost by age 5 years. 37 Many mounting external influences may impact long-term outcomes. Follow-up of our cohort to an older age may demonstrate if longer-term ND differences exist.
Conclusions
We demonstrated that, at our institution, EUGR in ELBW infants fed an EHM diet, when head and length growth were preserved, did not negatively impact neurodevelopment at 24 months CA. These findings challenge previous studies associating slow weight gain with increased risk for ND delay and suggest a protective effect of an EHM diet. Our study raises the question as to which parameters of NICU growth velocity (weight, HC, or length) should be used as a quality metric in relationship to future neurodevelopment, especially when an EHM diet is implemented to decrease morbidities. Our findings are reassuring, but larger cohorts of ELBW infants and a longer follow-up period may be needed to ensure that the neuroprotective effects of human milk are sustained.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.