
Abstract
Background:
Several Chinese mothers experience problems related to their breasts during breastfeeding and are referred to hospitals for treatment after a massage by a “cuirushi.” Some of these patients develop large breast abscesses. Notably, the treatment of residual milk cavities is difficult after pus aspiration. Lactational residual milk cavities in the breast hinder effortless breastfeeding, but no solution has been reported thus far. This study aims to explore the use of a simple and minimally invasive method for treating lactational residual milk cavities and enabling mothers to breastfeed effortlessly.
Materials and Methods:
We retrospectively analyzed clinical data of 28 patients with lactational residual milk cavities treated using negative-pressure suction cannula and drainage at our department from December 2016 to May 2019. The success rate, safety, and feasibility of this technique are summarized.
Results:
Among the 28 patients, the first catheterization was successful in 7 (25%) patients, the second in 13 (46.4%) patients, and the third or subsequent catheterizations in 8 (28.6%) patients. The intubation time was <10 days in 3 patients, between 10 and 20 days in 12 patients, and >20 days in 13 patients. During and after treatment, 21 patients (75%) continued breastfeeding with the affected breast.
Conclusions:
Ultrasound-guided negative-pressure suction cannula is a new method to treat lactational residual milk cavities that may remain after initial therapy for lactational breast abscess. The treatment of lactational residual milk cavities offers significant advantages in supporting mothers during breastfeeding.
Introduction
Most families in China acknowledge the benefits of breastfeeding and are eager to achieve the WHO breastfeeding guidelines's goals. However, the current breastfeeding rate in China is relatively low; in 2019, the rate of exclusive breastfeeding in China within 6 months was 29.2%. 1 A study 2 determined that breast massage by nonmedical personnel was a risk factor for lactational mammary abscess. The Academy of Breastfeeding (ABM) 3 recommends that the optimal treatment for lactational breast abscesses caused by mastitis is ultrasound (US)-guided puncture and drainage without interrupting breastfeeding, thereby enabling patients to recover with comparatively less trauma. However, during treatment, some patients may develop residual milk cavity into which the milk leaks continuously, influencing the babies' milk suckling and affecting breastfeeding.
Therefore, US-guided negative-pressure suction cannula is a new method to treat lactational residual milk cavities that may remain after initial therapy for lactational breast abscess. To the best of our knowledge, this is the first study to demonstrate the advantages of a negative-pressure suction cannula in the treatment of lactational residual milk cavity.
Materials and Methods
Definition of lactational residual milk cavity
Lactational residual milk cavity is the milk cavity formed by the accumulation of milk after initial therapy for lactational breast abscess. The distinction between a lactational residual milk cavity and a mammary abscess is that a lactational residual milk cavity contains milk, whereas a breast abscess is a localized accumulation of infected fluid in breast tissue. 4
General data
We retrospectively analyzed the clinical data of 28 patients with lactational residual milk cavity that affected breastfeeding who were treated at our outpatient department from December 2016 to May 2019. For statistical convenience, the severely affected side of one patient with bilateral breast lesions was considered for the study, the remaining patients had unilateral breast lesions. Patients with residual milk cavities not affecting breastfeeding were not included. Residual milk cavities affecting breastfeeding are referred to milk cavities under the nipple–areola that affected infant's suckling. This study was approved by the ethical committee of the Maternal and Child Health Hospital of Haidian District, Beijing. Informed consent was obtained from all cases. All 28 patients in this study had a history of breast massage by a “cuirushi.” In China, “cuirushi” is a person who assists mothers to produce more breast milk by massaging their breasts and is an accessible, although uncertificated layperson.
Steps and methods
Selection of puncture points: The needle was inserted into the upper part 1–2 cm from the residual milk cavity; the needle tip was pointed downward to reduce the possibility of shedding.
US-guided disposable cannula catheterization and drainage: A local subcutaneous injection was performed on the skin puncture point using 1 mL of 1% lidocaine. A disposable cannula (BD Insyte 22GA or 18GA) was inserted into the residual milk cavity under US guidance (e.g., the cavity with the most liquid was selected from the honeycombed multi-cavity), and the needle tip was located in the center of the residual milk cavity. After the milk flowed out successfully, the inner needle was withdrawn, and the cannula was connected to the connecting tube (venous connecting tube), which was, in turn, connected to a 10 mL negative-pressure syringe.
The disposable cannula and partial connecting tube were affixed to the breast skin using transparent film (Shingna medical skin healing film type A, transparent medical accessory; Shandong Shingna Medical Products Co., Ltd.). Patients were taught to observe and self-treat the drainage fluid. When the milk drained from the negative-pressure syringe was >8 mL, the milk was discarded and the negative-pressure syringe was reconnected for suction. The drainage volume was recorded, and the negative-pressure syringe was changed daily. Patients were recalled to evaluate the patency of the cannula every 3 days after surgery. If the drainage was not patent or loose, the cannula was replaced (Figs. 1 and 2).
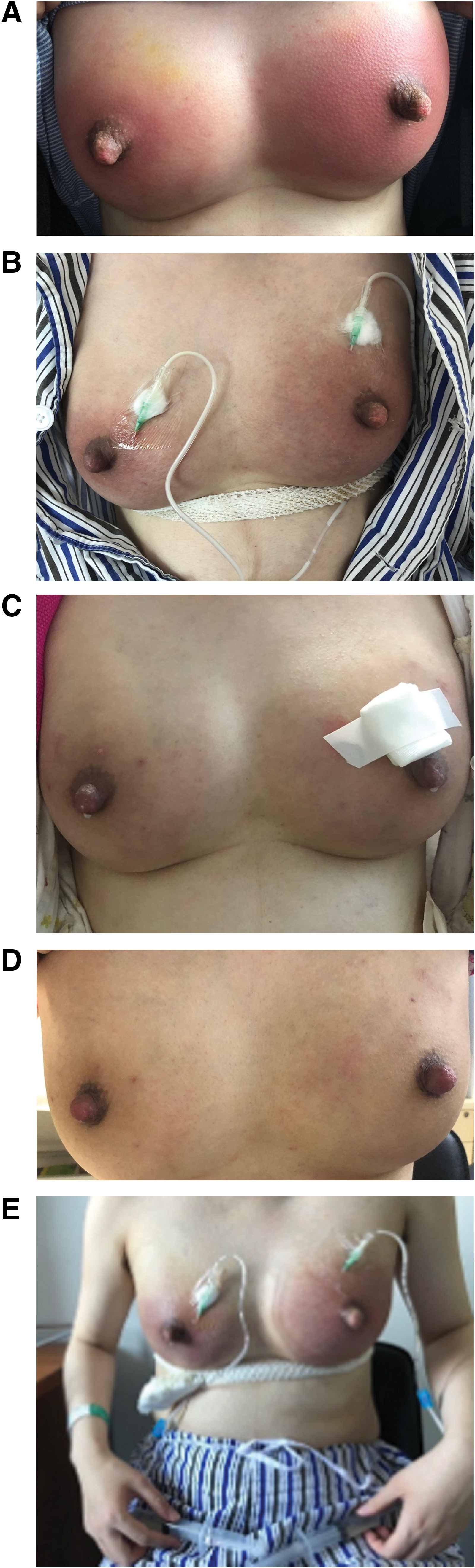
The treatment process and improvement process of the patient whose breasts had been massaged six times after 9 days postpartum.

The mother was 20 days postpartum and her breasts had been massaged three times,
Discharged patients were instructed to return immediately if they encountered the following problems: (1) the drainage fluid did not increase within 12 hours (5 cases); (2) the cannula fell off (8 cases); (3) the residual milk cavity enlarged (0 cases); and (4) the breast was red and swollen, painful, or feverish (0 cases). The cannula was removed when the 24 hours drainage volume of milk was <20 mL and the local mass had disappeared.
All patients were encouraged to breastfeed with bilateral breasts. When breastfeeding was difficult with the affected breast, the mothers were taught using manual expression. Antibiotics were not used during catheterization.
Criteria for recovery
One month after extubation, the breast mass was not enlarged on US, and no redness, swelling, or pain was noted in the original residual milk cavity.
Results
Among the 28 patients, the first catheterization was successful in 7 (25%) patients, the second in 13 (46.4%) patients, and the third or subsequent catheterizations in 8 (28.6%) patients. Intubation time was <10 days in 3 patients, between 10 and 20 days in 12 patients, and >20 days in 13 patients. Overall, 21 patients (75%) continued breastfeeding with the affected breast. No patient revealed any signs of infection, such as increased redness, swelling, and pain during catheterization. Moreover, scar formation was not observed at the affected site after recovery (Table 1).
Clinical Features and the Proportion of 28 Cases
MESA, methicillin-resistant Staphylococcus epidermidis; MRSA, methicillin-resistant Staphylococcus aureus.
Discussion
Cause of residual milk cavity
After lactational mastitis, if breastfeeding continues smoothly during treatment, generally, the symptoms will be gradually relieved, and the incidence of breast abscesses will reduce. However, all 28 patients in this study had a history of breast massage, and 23 had more than three breast massages. Witt et al. 5 indicated that in-office therapeutic breast massage during lactation helps reduce acute breast pain associated with milk stasis. They embrace the following principles: (1) focused gentle massage toward the axillae and (2) alternating gentle massage and hand expression.
Ouyang et al. 6 suggested that breastfeeding women in China generally seek help from a “cuirushi” when they experience difficulties in breastfeeding. The Ministry of Resources and Social Security has not recognized postpartum breast massage therapists as a job category, and breast massage therapists do not have to register with the Ministry of Resources and Social Security, which means that several women face breastfeeding issues but lack adequate professional support. A “cuirushi” is not a certified professional and uses methods that are nonscientific, thereby possibly leading to a higher incidence of breast abscesses and more severe breast damage. 2
In the event of galactostasis in mastitis, the milk cannot be effectively removed, leading to increased tension in the breast and milk ducts. 7 If the breasts are subjected to pressure of firm massage, the acinus and milk ducts can be damaged, thereby leaking milk into the breast stroma or causing a secondary infection. After puncture treatment of breast abscesses, the pus is discharged from the body, but milk is continuously leaked out from the damaged milk ducts, thereby forming residual milk cavity in the late stage of lactational breast abscesses. All the 28 patients in this study had a history of breast massage, and 23 had more than three breast massages. Among the 28 patients, the diameter of the abscess cavity was 5–10 cm in 9 patients and >10 cm in 11 patients. In our study, 71.4% of patients had large residual cavities.
The breasts are one of the exocrine glands in the human body. Similar to the sweat glands and lacrimal glands, breasts secrete spontaneously after being stimulated. Human lactation, like in other mammals, depends on mother–infant interaction. The babies' nipple suckling, 8 breast searching, and crying stimulate the release of oxytocin and prolactin in the mothers' body. Prolactin stimulates the lactating cells to produce milk, and oxytocin promotes the contraction of myoepithelial cells in the acinar lumina and milk ducts, resulting in milk ejection. According to a systematic review 9 on breast massage, no uniformity exists currently regarding the standard, method, time, and intensity of breast massage.
In most studies regarding breast massage, most women received a variety of interventions, including massages that could affect the result. In China, 10 breast massages are performed by both medical and nonmedical personnel, the indications and methods cannot be unified, and the massage quality cannot be evaluated objectively. Therefore, further studies should be conducted to confirm its safety and effectiveness.
The reason for not using antibiotics during this treatment and for applying negative-pressure drainage
Twenty-four patients had used one or more antibiotics, and four had not used antibiotics before catheterization. Moreover, antibiotics were not used during the catheterization and drainage of the residual milk cavity in the late stage of lactational breast abscesses. At this stage, breast infection was controlled, and the milk flow was maintained after catheterization. Milk contains several anti-infective substances, such as white blood cells, immune substances, cytokines, and lactoferrin. 11 The protective effect of breast milk against infection is well documented. Data prove that milk from various species, including humans, contains antibodies against a vast number of antigens. 12 Although no similar literature has been reported, we believe that is the primary reason for the low likelihood of secondary infections in the breast.
Furthermore, the residual cavity is in a negative-pressure state, which is conducive to the growth of internal granulation tissue. When granulation tissue growth blocks breast breakage or it gradually repairs, the drainage volume will suddenly decrease, and the residual cavity will return to normal after extubation.
Discussion on catheterization times and the indwelling time
In all patients, a low-cost disposable cannula was used for puncture and drainage. Overall, 25% of patients underwent one catheterization, 46.4% underwent two catheterizations, and 28.6% underwent three or more catheterizations until successful completion. The causes of multiple catheterizations include catheter detachment and catheter blockage. The disposable cannula and the part of the connecting tube connecting the cannula are affixed to the breast skin by an adhesive and, therefore, it is not firmly attached. Recently, pigtail tube drainage, small incision drainage, and EnCor vacuum-assisted breast biopsy system have been reported13–15 to treat lactational breast abscess. However, these techniques are relatively invasive or expensive and resulted in postoperative scars.
The advantages of the negative-pressure suction cannula for treatment of lactational residual milk cavities are as follows: (1) simple technology that is easy to learn, (2) no stitches required and no scars, and (3) low cost. The disadvantage is that the fixation is not stable, with the possibility of slipping, thereby requiring multiple punctures. Only 25% of the cases in this study had a successful first catheterization. If the cannula falls off or the catheter is blocked, it can be replaced the next day. Overall, 42.9% and 46.4% of patients had the catheter indwelling for 10–20 days and >20 days, respectively, suggesting that it takes longer for the residual milk cavity to recover. High adaptability was observed during intubation. Overall, 75% of patients could continue breastfeeding with the affected side.
Conclusions
US-guided negative-pressure suction cannula is a new method to treat lactational residual milk cavities that may remain after initial therapy for lactational breast abscess. This treatment of lactational residual milk cavities offers potentially significant advantages in supporting the mother's breastfeeding. Clearly, future randomized clinical trials are necessary to confirm the value of this therapeutic approach.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.