
Abstract
Background:
Oral direct factor Xa inhibitors, collectively referred to as direct oral anticoagulants, are not recommended for breastfeeding women due to insufficient data about the transfer of these drugs into breast milk. In this study, we serially measured rivaroxaban concentrations in the breast milk of one nursing mother who was at high risk of deep vein thrombosis and evaluated the health of her breastfed infant.
Materials and Methods:
Breast milk rivaroxaban concentrations were measured 3 months after delivery by a validated liquid chromatography-tandem mass spectrometry method. Breast milk samples were collected sequentially after 15 mg of oral rivaroxaban administration after ethical approval and informed consent. Case report: A 38-year-old female diagnosed with the antiphospholipid syndrome had received rivaroxaban after delivery. The infant was partially breastfed until the age of 18 months. The mean minimum and maximum rivaroxaban concentrations in breast milk were 9.73 ng/mL before each dose and 53.9 ng/mL at 6 hours after each dose, respectively. The mean daily infant dose was 0.0034 mg/kg and the mean relative infant dose (RID) via breast milk was 1.79%.
Discussion and Conclusion:
The RIDs of rivaroxaban did not exceed 10% of the maternal dose, suggesting that exposure of rivaroxaban via breastfed is seldom clinically relevant for the infant. A pediatric assessment of the infant found no detectable drug-related adverse effects. Further studies are needed to elucidate how breastfeeding infants are impacted by exposure to rivaroxaban.
Introduction
A subset of pregnant patients require anticoagulation during pregnancy and/or in the postpartum period, including women at high risk of deep vein thrombosis (DVT), those with valvular heart diseases, and some with fetal loss. Oral direct factor Xa inhibitors (e.g., rivaroxaban, apixaban, edoxaban), collectively referred to as direct oral anticoagulants (DOACs), should not be used during pregnancy due to increased reproductive risks in animal studies and insufficient human safety and efficacy data.1,2 DOACs are also not recommended for breastfeeding women due to insufficient data about the transfer of these drugs into breast milk. 2 Although the data about rivaroxaban secretion into breast milk have been already reported,3,4 more data are needed. Furthermore, a detailed concentration profile in the breast milk after rivaroxaban administration has been not observed. In this study, we measured rivaroxaban concentrations in the breast milk of one nursing mother who was at high risk of DVT and evaluated the health of her breastfed infant.
Materials and Methods
Rivaroxaban detection
Rivaroxaban and its structurally analogous internal standard (IS, rivaroxaban-d4) were obtained from Toronto Research Chemicals (Toronto, Canada). Acetonitrile in LC-MS grade, 10 mM aqueous ammonium formate containing 0.1% formic acid in LC-MS grade, and formic acid were obtained from Fisher Scientific GmbH (Schwerte, Germany). Water was purified by the Milli Q system (Millipore Waters, Tokyo, Japan). Blank breast milk was obtained from healthy volunteer subjects.
Sample collection and preparation
Breast milk samples were collected sequentially at −1, 3, 6, 9, 12, 15, and 18 hours after 15 mg of oral rivaroxaban administration, and stored below −80°C until analysis. To determine the intraday variation of rivaroxaban transfer into breast milk, samples were collected twice on 2 different days. Sample preparation was performed by protein precipitation with acetonitrile. Two hundred microliters of breast milk from calibration, quality control, or patient samples were placed to 1.5 mL plastic centrifuge tubes. Acetonitrile (200 μL) containing deuterated IS (rivaroxaban-d4, 100 ng/mL) was added to samples. The samples were then centrifuged at 26,700 ×g for 5 minutes at 4°C. The supernatants were filtered through a 0.22 μm filter (Millex®-GV; Merck Millipore, Tokyo, Japan) and transferred to an autosampler vial. Finally, 1 μL was injected into the LC-MS/MS system.
LC-MS/MS method
Chromatography was performed on a 3000 Ultimate nano-LC system interfaced with a TSQ Vantage mass spectrometer (Thermo Scientific). The compounds were eluted from a Unison UK-C18 (3 μm reversed-phase porous ODS, 2 mm i.d. × 100 mm, Imtakt, Kyoto, Japan) in a gradient conditions, in which the mobile phase consisted of solvent A (10 mM aqueous ammonium formate containing 0.1% formic acid) and solvent B (acetonitrile containing 0.1% formic acid). The gradient was as follows: from time 0 to 2 minutes, a linear gradient from A:B 95:5 to A:B 5:95, time 2–4 minutes, A:B 5:95, and time 4–5 minutes, A:B 95:5. The flow rate was set at 0.4 mL/min. The column and autosampler tray temperatures were 40°C and 10°C, respectively. The MS/MS instrument was operated with a capillary voltage of 3.5 kV, source block temperature of 120°C, and desolvation gas (nitrogen) heated to 350°C and delivered at 600 L/h. The collision cell pressure was 3.0 × 10–3 Torr of indicated argon pressure. The compounds were monitored in positive ion mode using multiple reaction monitoring. The ions used for quantification in the scan mode were m/z 436 for rivaroxaban and m/z 440 for rivaroxaban-d4 (IS). Electrospray ionization was used in the positive ion mode, and the protonated ions [M + H]+ at m/z 145 for rivaroxaban and m/z 149 for rivaroxaban-d4 (IS) were monitored for quantification in the selected ion monitoring mode.
Method validation
To plot the calibration curves, rivaroxaban at seven different concentrations, from 0.5 to 1,000 ng/mL in breast milk were prepared in triplicate and analyzed. The calibration curve was obtained by plotting the peak area ratios of rivaroxaban to IS. The reproducibility of the method was evaluated by analyzing breast milk samples containing three different concentrations of the tested drugs (five replicates; intraday reproducibility) on the same day and also over three consecutive days (three replicates; interday reproducibility). The limit of detection and limit of quantification were defined as the quantities of breast milk samples corresponding to 3 and 10 times the baseline noise, respectively.
Statistical methods
The mean rivaroxaban concentrations in breast milk were used to calculate the mean area under the 24-hour concentration-time curve (AUC0–24) of rivaroxaban in breast milk. The AUC0–24 was calculated using the trapezoidal rule during the ascending portion of the curve and the log-trapezoidal rule during the descending portion of the curve. The elimination rate constant (ke) was estimated by log-linear regression of the descending portion of the observed concentrations. The half-life (t1/2) was calculated as 0.693/ke. To estimate the average drug level (Cave) in the breast milk, the calculated AUC0–24 was divided by the number of hours under the curve (24 hours).
Ethical approval
This study was approved by the Ethics Committee of the National Center for Child Health and Development, and the participant provided written informed consent.
Results
Rivaroxaban detection
The method exhibited excellent performance in terms of selectivity, robustness, the short run time (5 min/sample), and simplicity of sample preparation. The calibration range was ranged from 0.5 to 1,000 ng/mL with 200 μL of breast milk sample. Intra- and interday mean accuracies were within the ranges of 100.9%–103.7% and 99.8%–106.8%, respectively. Intra- and interday precisions were within the ranges of 1.1% to 2.1% and 1.8% to 8.7%, respectively.
Case
A 38-year-old female (78.0 kg body weight) diagnosed with antiphospholipid syndrome had received rivaroxaban before pregnancy at a daily oral dose of 15 mg (0.19 mg/kg) for 3 months to treat a DVT in her left lower thigh. She had experienced a stillbirth at 20 weeks' gestational age (GA) in her previous pregnancy. Rivaroxaban was discontinued because she wished to become pregnant again, and she was switched to low-dose aspirin (LDA) therapy. After becoming pregnant, unfractionated heparin was also administered concurrently throughout gestation. The patient's platelet counts immediately fell to 9,000/lL despite the temporary mitigating effect of intravenous immunoglobulin G therapy. Thrombocytopenia treatment with oral prednisolone at a daily dose of 40 mg and with intravenous methylprednisolone pulse therapy was ineffective. After administration of weekly intravenous rituximab (600 mg per week; four doses total) from 12 to 15 weeks of gestation, the platelet count was increased to the normal range. The daily dose of prednisolone was tapered to 15 mg by 28 weeks of gestation. During the patient's pregnancy, her platelet counts were maintained at about 150,000/μL. Results of D-dimer tests were consistently negative (<1.0 μg/mL). Overall, there was no worsening of DVT symptoms.
At 37 weeks' GA, a healthy female infant was born by cesarean section after spontaneous rupture of membranes, with a birth weight of 2,676 g. The infant's Apgar scores at 1 and 5 minutes were 8 and 9, respectively, and no abnormalities were observed. LDA and rivaroxaban were resumed at 3 and 5 days after delivery, respectively. The infant was partially (nonexclusively, at least 50%) breastfed until the time of this writing (at the age of 18 months); she continues to develop appropriately and no apparent adverse effects such as hemorrhage were observed at a medical check-up at 1 and 3 months, respectively.
Rivaroxaban concentration in breast milk
About 1 mL of breast milk was manually expressed by herself from one breast at each sample time. Breast milk rivaroxaban concentrations were measured 3 months after delivery by a validated liquid chromatography-tandem mass spectrometry method. As shown in Figure 1, breast milk rivaroxaban concentrations reached a peak at 6 hours after administration and decreased gradually thereafter. The mean minimum and maximum rivaroxaban concentrations in breast milk were 9.73 ng/mL before each dose and 53.9 ng/mL at 6 hours after each dose, respectively (Table 1). The estimated pharmacokinetic parameters of rivaroxaban in breast milk were described in Table 2. The half-life of rivaroxaban in breast milk was 4.7 hours. The calculated mean AUC0–24 and the average of rivaroxaban level in breast milk were 543.8 ng·hr/mL and 22.7 ng/mL, respectively. The mean daily infant dose was 0.0034 mg/kg and the mean relative infant dose (RID) via breast milk was 1.79%.
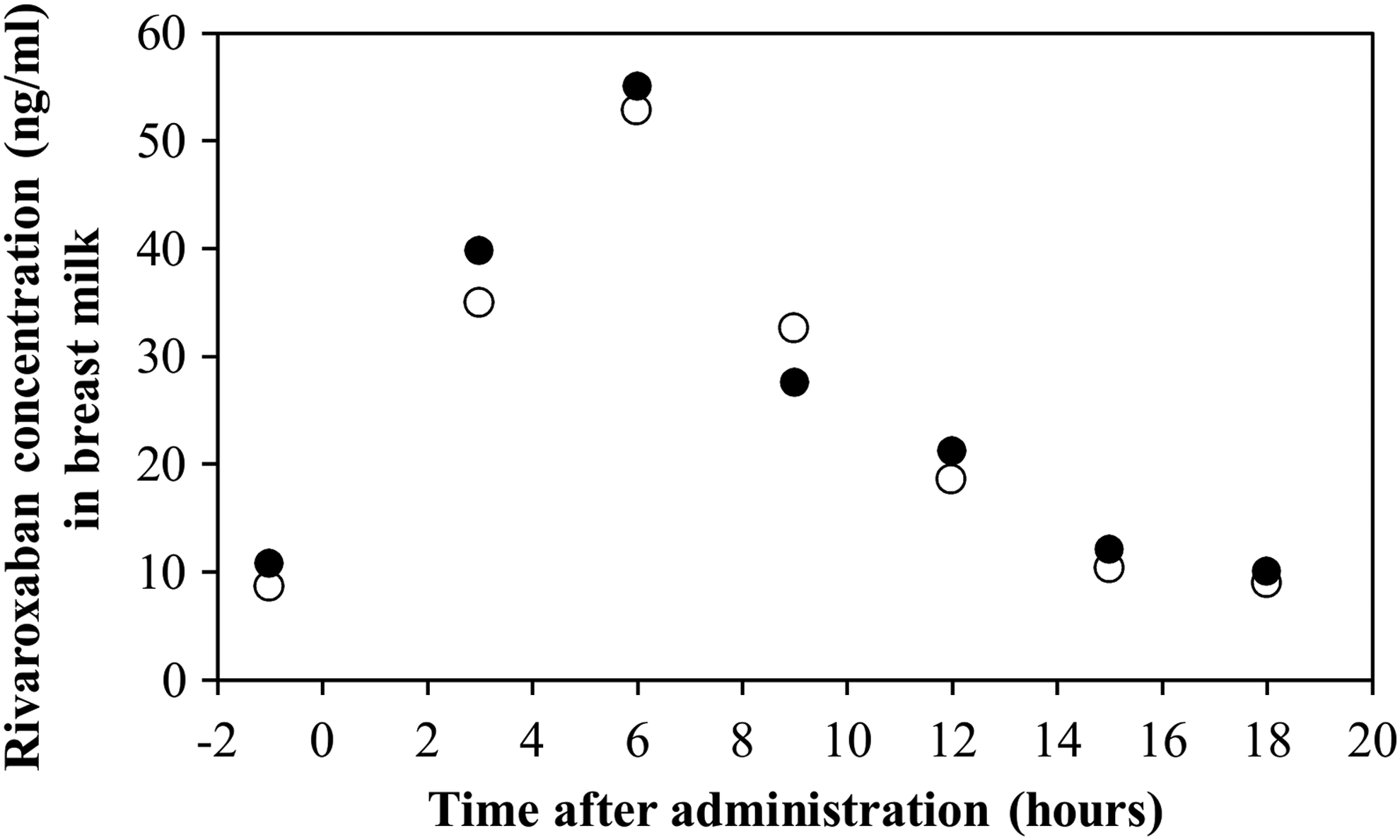
Concentration-time profile of rivaroxaban in breast milk. x-axis, time after administration. Closed and open circles indicate the concentrations of rivaroxaban in breast milk after doses on 2 different days.
Rivaroxaban Concentration in Breast Milk
Estimated Pharmacokinetic Parameters of Rivaroxaban in Breast Milk
The estimated daily infant dose via breast milk (mg/kg) was calculated based on drug concentrations in breast milk (mg/mL) and volume of breast milk ingested (mL/kg/day).
Since the actual volume of milk ingested by the infant was not known, 150 mL/kg/day was used in the calculation.
The relative infant dose (RID) was calculated using the estimated daily infant dose via breast milk (mg/kg/day) and the maternal dose (mg/kg/day).
Cmax, peak concentration in breast milk; tmax, time to Cmax; AUC0–24, area under the 24-hours concentration-time curve; ke, terminal-phase elimination rate constant; t½, terminal phase elimination half-life.
Discussion
Information on drug disposition in lactating women is important for enabling adequate and safe treatment decisions for both mothers and their infants. We report a case of anticoagulant therapy with rivaroxaban in a postpartum patient and demonstrate that rivaroxaban passes into human breast milk. Rivaroxaban concentrations in the breast milk samples were reached at a peak after 6 hours of drug administration. The mean RID of rivaroxaban that was calculated from the average concentration was 1.79%, which was similar to the previously reported.3,4 These RIDs did not exceed 10% of the maternal dose, suggesting that exposure of rivaroxaban via breast milk is usually not considered to be clinically relevant for the infant. 5 A pediatric assessment of the infant found the achievement of expected developmental progress for age and no detectable drug-related adverse effects.
Results must be interpreted with caution as the RID does not take the bioavailability of rivaroxaban in the infant into consideration. 6 A bioavailability of rivaroxaban was achieved to more than 80% when taken with food, and rivaroxaban is metabolized by cytochrome P450 enzymes, 7 suggesting that decreased drug clearance in an infant caused an unexpected drug exposure to breast-fed infants. Moreover, potential age-related differences in the pharmacodynamic effects of rivaroxaban in neonates need to be considered. 8 To characterize the infant's exposure precisely, an assay of a drug in blood samples of the breastfed infant would be required. Therefore, it cannot be definitely concluded that rivaroxaban is safe in breastfed infants.
Conclusion
In our case, the rivaroxaban concentration into breast milk was quite low, and the mean RID was 1.79% of the maternal dose. Further studies are needed to elucidate how breastfeeding infants are impacted by exposure to rivaroxaban and other DOACs.
Authorship
J.S., H.K., K.K., and Y.N. performed the research. J.S., H.K., K.K., and A.M. designed the research study. J.S. and H.K. analyzed the data. J.S., K.K., A.Y., and A.M. wrote the article.
Footnotes
Acknowledgment
We thank Ms. Mariko Takagai for her expert research assistance.
Disclosure Statement
A.M. received research grants/honoraria from Astellas Pharma Co. Ltd., Chugai Pharmaceutical Co. Ltd., and Mitsubishi Tanabe Pharma Co., Ltd. All other authors declare no conflicts of interest.
Funding Information
This work was supported by the Research Program on “A Study on the Risks and Benefits of Drug Use During Pregnancy and Lactation” from the Japanese Agency for Medical Research and Development, AMED (19mk0101086h0001), awarded to A.M.