
Abstract
Background:
Maternal concern about inadequate milk volume commonly emerges in the first 2 weeks postpartum, a critical lactation period that includes secretory activation. This review summarizes the biology of secretory activation and evaluates the accuracy and feasibility of published measures of secretory activation.
Materials and Methods:
A systematic search of measures of secretory activation for mothers of healthy term and preterm infants yielded 62 abstracts. Following additional screening, 15 publications qualified for quantitative synthesis review and were evaluated with respect to accuracy (validated with another measure of secretory activation in the same mother) and feasibility (accessibility, cost, and ease of use).
Results:
Maternal perception of milk coming in (MP) is the most feasible measure, but its accuracy has not been established. Patterns of increase in maternal milk volume have been validated with maternal milk-borne biomarkers in breastfeeding, and breast pump-dependent mothers and normal values have been published. Accuracy of serial maternal urinary lactose concentrations has not been established for secretory activation and lacks feasibility. Maternal milk biomarkers are the accurate standard to which other measures are compared but currently lack feasibility for routine use.
Conclusions:
Use of secretory activation measures can personalize lactation care by matching maternal risk with appropriate diagnostics. Priorities for research and practice include validation of MP as a population-based screening tool, implementation of techniques that measure patterns of increase in milk volume for moderate risk populations, and the development of milk biomarker science for point-of-care use in the most complicated lactation scenarios.
Introduction
Maternal concern about inadequate milk volume is the most frequently reported reason for the cessation of exclusive or partial breastfeeding in healthy mother-infant dyads.1–7 Breast pump-dependent mothers of preterm infants cared for in the neonatal intensive care unit (NICU) also stop providing milk and fail to meet their own self-stated goals for continued feeding of their milk after NICU discharge due to inadequate pumped milk volume.8,9 In both populations, concerns about inadequate milk volume commonly emerge in the first 2 weeks postpartum, a critical period in the establishment of lactation and the development of an adequate milk volume that includes secretory activation or lactogenesis II defined as the onset of copious milk secretion. 10 Milk volume concerns during this period predict suboptimal long-term lactation outcomes, including poor infant weight gain, lack of exclusive breastfeeding, supplementation with formula or donor human milk, early unplanned weaning, and mothers' inability to meet their personal feeding goals.8,11–14
Achievement of secretory activation is so critical for adequate milk volume that nearly two decades ago, Chapman et al. called for targeted lactation care during the early postpartum period as a public health priority. 3 Since Chapman's prescient article, multiple risk factors for delayed or impaired secretory activation have been reported, including acute or chronic maternal health conditions such as diabetes, pregnancy-induced hypertension, and prepregnancy overweight (body–mass index; BMI ≥25) or obesity (BMI ≥30). In addition, delivery factors such as preterm birth, breast pump-dependency, cesarean birth, and excessive blood loss have been linked to delayed or impaired secretory activation.10,15–17 Although these risk factors affect a sizeable proportion of the childbearing population, lactation care has not evolved to address these challenges. Typically, studies recommend providing additional lactation “support” during this period, but “support” has not been translated into evidence-based, personalized interventions that target underlying risk factors. Furthermore, simply providing “additional support” is not always effective in helping at-risk women achieve adequate milk volumes.8,18–21
Thus, there is a need to prioritize, reconceptualize, and personalize lactation care during this critical period. Central to the design, implementation, and evaluation of evidence-based lactation interventions is the integration of objective, accurate, and feasible measures of secretory activation. These measures should be used in both research and practice to guide the assessment, diagnosis, and management of delayed or impaired secretory activation, especially in high-risk populations. The purpose of this review is to summarize the biology of secretory activation and to evaluate the measures of secretory activation with respect to accuracy and feasibility (accessibility, cost, and ease of use) for use in research and clinical practice. These measures, as reported in the research literature, include MP, patterns of increase in milk volume, serial maternal urinary lactose concentration, and serial maternal milk-borne biomarkers.
Biology of Secretory Activation
During mid-pregnancy the breast undergoes secretory differentiation, during which the mammary epithelial cells differentiate into lactocytes capable of synthesizing milk components such as lactose. 22 Secretory differentiation is catalyzed by systemic hormones that stimulate lactocyte growth and ductal system proliferation, including reproductive (estrogen, progesterone, prolactin, and oxytocin) and metabolic hormones (human growth hormone, glucocorticoids, and insulin). 23 The transition of the mammary gland from secretory differentiation to secretory activation occurs during a short but critical postpartum period that involves dramatic changes in systemic hormones, anatomical changes in the mammary epithelium, and compositional changes in milk. 24
Changes in systemic hormones occur with the delivery of the placenta, causing a rapid decline in circulating progesterone, which antenatally inhibits the milk-synthesis capability of prolactin. 25 Prolactin, newly released from its progesterone inhibition, catalyzes anatomic changes in the mammary epithelium, specifically the closure of paracellular pathways. 22 Paracellular pathway closure is essential to subsequent milk secretion, adequate milk volume, and the maintenance of lactation. 26 Impaired paracellular pathway closure disrupts milk synthesis at a critical lactation stage, making later resolution of low milk volumes difficult or impossible. 24 Milk composition changes from colostrum to transitional milk due to a combination of activated milk synthesis in the lactocyte and paracellular pathway closure. As a result, lactose, citrate, and fat are retained in the alveolar lumen and available for feeding. 27 For healthy mothers with uncomplicated pregnancy and birth scenarios, secretory activation occurs within 72 hours postpartum. 16
However, several maternal risk factors have been associated with delayed and/or impaired secretory activation, including primigravidae, overweight and obesity, preterm birth, and/or perinatal complications such as antenatal bed rest, cesarean delivery, chorioamnionitis, and pregnancy-induced hypertension along with the use of medications to manage these conditions.9,11,16,17,28–30 The biologic mechanisms that explain most of these risk factors have not been well-elucidated.
Methods
A systematic search was undertaken to identify and evaluate the different measures of secretory activation for mothers of both healthy term and preterm infants. No time limits were placed on the search strategy since much of this original research was conducted decades ago. 31 An exhaustive literature search was performed between June 2016 and July 2019 and included PubMed, the Cumulative Index for Nursing and Allied Health (CINAHL), Embase, and the SCOPUS databases. Search terms included secretory activation, lactogenesis, milk production, milk synthesis, milk yield, milk volume, tight junctions, measure, urine, and biomarker. Terms were searched both separately and in various combinations.
Study selection
The selection of articles was performed using titles, abstracts, and full texts. A minimum of two authors reviewed all full-text studies. Inclusion criteria were as follows: (1) human subjects, (2) English language, (3) purpose was measurement of secretory activation or milk coming in, and (4) a second measure of secretory activation was used to establish accuracy of the proposed measurement with the exception of milk-borne biomarkers because this measure is considered the accurate standard. The search process yielded 62 abstracts, which were reviewed for suitability. An additional eight full-text articles were retrieved by text mining. Of these 70 records, 15 met inclusion criteria (Fig. 1). Agreement among authors was obtained through discussion, yielding a total of 15 publications for quantitative synthesis review.
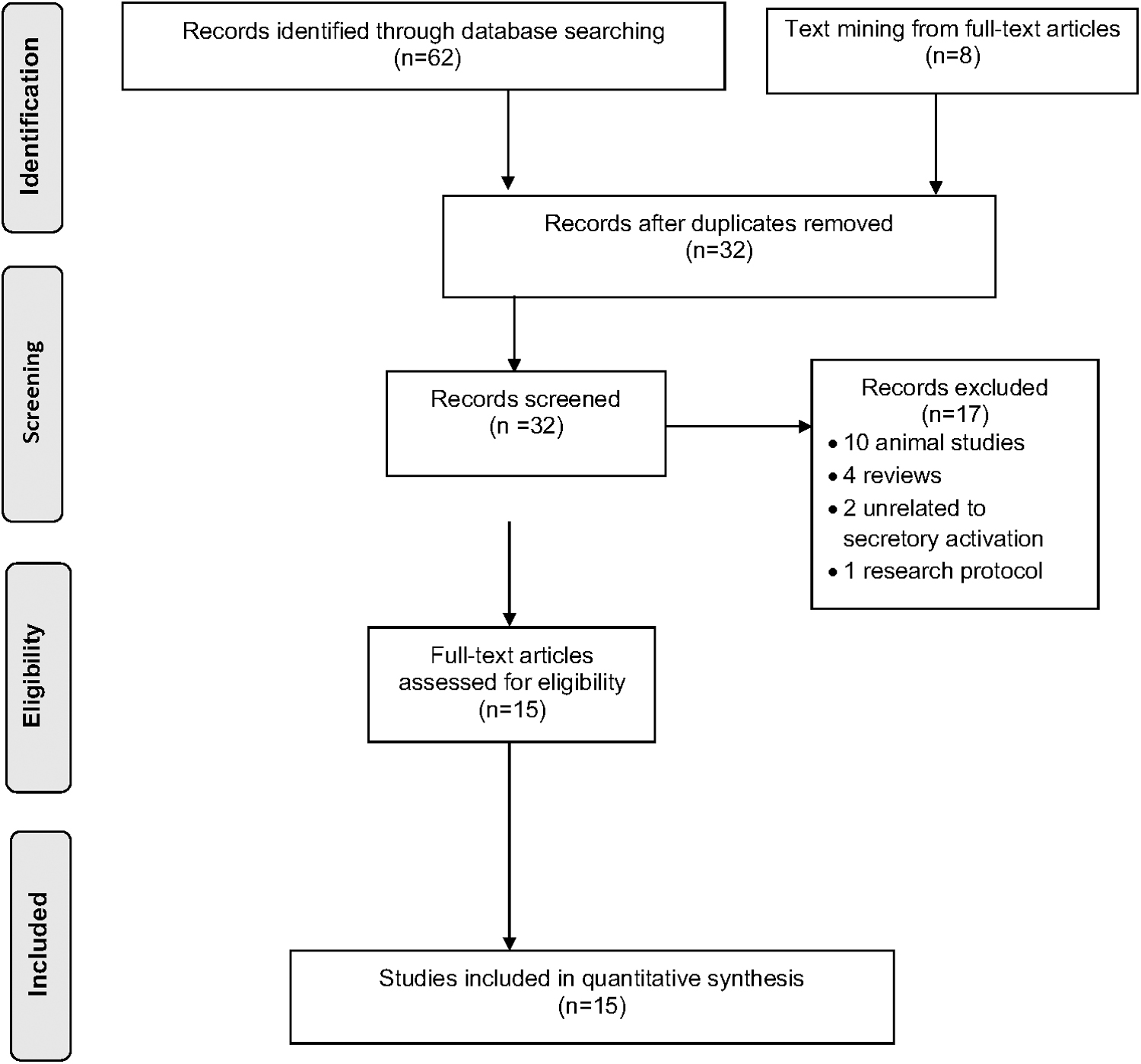
PRISMA flowchart for selection of studies.
Measures of Secretory Activation
The origins and underlying physiology for each of the four measures of secretory activation are described in this section. Table 1 summarizes each measure with respect to its accuracy, defined for this review as the concurrent validation with another measure of secretory activation. This review will also examine the feasibility of each measure, defined for this review as accessibility, cost, ease of use, and interference with normal breastfeeding behaviors or breast pump use.
Measures of Secretory Activation: Methodologies, Subjects, and Accuracy
Maternal perception of milk coming in
Maternal perception of milk coming in (MP) has been used as a measure of secretory activation for centuries, but has received limited rigorous investigation. 3 Although this measure was originally described as a sudden sensation of breast fullness and leaking of milk, a myriad of indicators have since been reported and used in research and practice. 32 These indicators have included both breast changes and infant behaviors such as audible swallowing during breastfeeding. Seven studies32–38 examined the timing of MP, with three32–34 of these seven measuring the time from birth until mothers reported MP. The remaining studies measured MP based on varied indicators such as maternal feeling of overfullness of breasts, 33 time postpartum that mother first felt breast fullness,36,37,39 sensation of hard breasts, fullness, swelling, or leakage of milk, 32 sudden feeling of breast fullness,34,35 and a breast fullness score. 38 Although the average time postpartum for MP is 60 hours, this time varies significantly among mothers (12–128 hours) and is influenced by factors such as mode of birth and maternal health characteristics. 28
No previous research has established the concurrent validity of MP using other validated measures of secretory activation for individual mothers. Nonetheless several researchers have used MP for predictive and comparison studies. Chapman and Perez-Escamilla 36 established the predictive validity of the timing of MP as a marker for subsequent delayed onset of lactogenesis. Similarly, Arthur et al. 33 demonstrated that diabetic mothers reported MP later than nondiabetic mothers. Kulski et al. 32 reported no difference between the timing of MP for cesarean versus vaginal birth. In separate studies, primigravidas reported MP later than multiparous mothers.34,35 These studies also reveal variability in the precision with which mothers report the timing of MP, with some reporting an exact time and others reporting an interval such as “the morning” or “overnight.” 39 Although this cluster of studies used MP as a predictor or dependent variable, both the indicators and methods of assessment varied considerably among investigators, highlighting a research gap. Thus, to date it is unknown whether MP accurately measures secretory activation and, if it does, which specific indicators of MP should be used for research and practice.
Patterns of increase in milk volume
Multiple researchers have described patterns of increase in maternal milk volume during the first 2 weeks postpartum.2,33,37,39–44 This measure has been validated concurrently with serial milk biomarkers in individual mothers33,40,41,44,45 and has been used to predict delayed or impaired secretory activation in healthy and at-risk breastfeeding dyads.5,16,17,28,42,43 However, patterns of increase in maternal milk volume are not a direct measure of secretory activation, but rather a combination of milk synthesis and the effectiveness and efficiency of milk removal by the infant, hand, or breast pump.
Research with healthy breastfeeding dyads has established normal values for milk volume during the first 2 weeks postpartum by calculating the amount of milk removed from the breast by the infant during feeding, referred to as “milk intake” or “milk transfer.” 44 This measurement is done using test weights, in which the infant is weighed pre- and postfeed under the same conditions with a highly accurate digital (not a rotary balance) scale, with 1 g increase in weight = 1 mL of milk removed.46,47 No significant differences in the accuracy of 24-hour test-weighing procedures have been reported between measures performed in the hospital by research staff and/or mothers and in the home by mothers.33,45,48–52 Furthermore, recognizing that in-home test weights during this vulnerable postpartum period may be incomplete, Neville et al. published an algorithm for estimating 24-hour milk volume when only intermittent test weights were performed. 53
Five studies used test weights to measure milk volume during the first 2 weeks in healthy term breastfeeding dyads and incorporated both prospective longitudinal33,34,44,45 and cross-sectional 54 designs. Both milliliters (mL) and grams (g) of milk volume have been reported in these studies, so for the purpose of this review, we report the unit used by the investigators in published studies. Mean milk volumes reported during the first 24 hours postpartum were 15 g, 54 37 g, 51 37.1 g, 45 and 44 g, 44 but these small volumes increased rapidly between days 2 and 7 postpartum. 44 In Neville's classic longitudinal study of 13 multiparous, exclusively breastfeeding mothers, milk volume patterns revealed a gradual increase between birth and 36 hours postpartum, followed by an abrupt increase between 49 and 96 hours, with a mean milk volume on day 7 of 610 g (range = 421–1008). 44 Chen et al. reported mean milk volume on day 5 postpartum for 24 primigravidas who gave birth vaginally (556 g) or by cesarean section (617 g) and for 16 multiparous mothers who gave birth vaginally (750 g). 34 Arthur et al. reported a mean milk volume of 82 g for day 2 and 556 g for day 6 postpartum in 13 exclusively breastfeeding mothers. 33
However, mean values do not reflect the marked variability for individual mothers and infants. For example, Kent et al. 55 reported 24-hour milk volumes ranging from 338 to 722 mL between days 6 and 13 for 29 healthy dyads who either did not perceive (N = 3) or did perceive (N = 26) breastfeeding problems. Similarly, Neville et al. 44 reported on a subset of mothers for whom milk volume peaked on day 4 postpartum but decreased thereafter. 44
Most, but not all, studies that measured hand expressed or pumped milk volume instead of infant milk intake were conducted with mothers of preterm infants hospitalized in the NICU.37,40,41 While eight studies reported milk volume during the first 2 weeks postpartum, only three specifically validated patterns of increase in maternal milk volume with milk biomarkers of secretory activation in term 44 and preterm40,41 populations. Remaining studies enrolled mothers of preterm infants into randomized37,56,57 and nonrandomized58,59 intervention studies for which patterns of increase in milk volume during the first 2 weeks postpartum were dependent variables and may have been reported in combination with another measure of secretory activation. 37
Similar to findings in term infants, these studies reveal minimal milk volumes during the first 24 hours postpartum. In Parker's randomized trial of early versus late pumping in mothers of very low birth weight (VLBW; < 1500 g birth weight) infants, mean milk volume during the first 24 hours postpartum was 19.2 mL and 0.7 mL for the early and late pumping groups, respectively. 37 Lussier's comparison of hand expression versus electric breast pump use revealed median (IQR) milk volumes of 0.1 mL (0, 2.6) and 3.7 mL (2, 22), respectively, for the first 24-hours postpartum. 57 A number of studies have reported a marked increase in milk volume starting on day 3 or 4 postpartum.2,17,39,41,45,55–57,60 Parker reported mean milk volumes on days 3 and 4, respectively, of 142 mL and 186 mL for the early pumping group and 45 mL and 70 mL for the late pumping group. 37 Lussier reported day 4 median milk volumes of 119 mL and 265 mL for hand expression and electric breast pump groups, respectively. 57 At the end of the first postpartum week, Parker reported mean cumulative milk volume of 1,374 mL and 608 mL in the early and late pumping groups, 37 and Lussier reported median cumulative volume of 456 mL and 1,371 mL in the hand expression and electric breast pump groups, respectively. 57 Marked individual maternal variability was reported in all studies.37,41,57,59 Furthermore, maternal milk volume differed significantly as a function of type and timing of breast pump use, as well as hand expression versus pump for milk removal. These findings highlight the influence of the effectiveness and efficiency of milk removal when maternal milk volume is used as a measure of secretory activation.
Serial urinary lactose concentration measures
The use of serial maternal urinary lactose concentration (urinary lactose) as a measure of biosynthetic activity in the mammary gland was first described in the 19th century 61 and refined by Watkins in 1928, who described an extreme sudden increase in urinary lactose immediately before birth. 62 This measure is based upon both the upregulation of lactose production and secretion in the mammary gland, as well as the patency of paracellular pathways. Thus, serial changes in urinary lactose concentrations provide an indirect measure of paracellular pathway patency. 63 When the paracellular pathways are open, as is the case during secretory differentiation, lactose passes readily into the maternal blood and is excreted in the urine. When paracellular pathways close as occurs with secretory activation, urinary lactose concentrations decrease. 22
Although no study has focused specifically on the validation or use of serial urinary lactose measures during secretory activation, this measure has been correlated with patterns of increase in milk volume in mothers of term64,65 and preterm infants. 63 It has also been used to predict milk volume as measured by test weights 64 and to diagnose subclinical mastitis, 66 which is accompanied by reopening of paracellular pathways during established lactation.66–68 Serial urinary lactose concentration measures were originally conceptualized as an alternative to more invasive or disruptive measures of secretory activation such as test weights and maternal milk biomarkers.63,64,67,68 However, the measurement of urinary lactose over a 24-hour period versus a one-time spot check is preferred because analytes can vary depending on the time of day collected and will yield variable results. Thus, this measure is seldom used in current research and practice due to the inconvenience of collecting and analyzing 24-hour urine samples.
Serial measures of maternal milk biomarkers
Predictable changes in serial maternal milk biomarker concentrations (milk biomarker) occur between birth and secretory activation, 69 forming the basis for a measurement technique that was developed over three decades ago. 44 These biomarkers, which include lactose, citrate, sodium (Na), and total protein, are secreted through distinct transcellular and paracellular pathways during secretory activation (Fig. 2) and currently serve as the accurate standard to which other measures are compared. Fat and potassium (K) have also been used as biomarkers, with fat representing a specific transcellular pathway and potassium used primarily in the Na/K ratio to standardize Na fluctuations.32,45 Potassium concentrations increase rapidly after birth, stabilizing ≤96 hours postpartum.71,72

Origins of secretory activation.
Four transcellular pathways are involved in milk synthesis and secretion and enable the transfer of milk components across the cellular membrane. 70 In contrast, a single paracellular pathway bypasses the epithelial cell itself, allowing direct communication between maternal blood and milk. 71 This pathway is open at the time of birth and gradually closes during secretory activation, a prerequisite for continued milk secretion so that lactose, the primary osmotic driver of milk volume, remains in the mammary gland. 29 The paracellular pathway reopens only during inflammation (mastitis) and involution (weaning). 72 Thus, the predictable changes in milk biomarker concentrations during the early postpartum period reflect both upregulated milk synthesis and gradual paracellular pathway closure (Table 2). These biomarker changes have been described in uncomplicated lactation scenarios, and aberrations in biomarker changes coincide with and/or predict impaired secretory activation.5,17,40
Serial Changes in Milk Components as Biomarkers of Secretory Activation in Mothers of Term and Preterm Infants
Sample collected once or twice daily over the interval, not each day over the interval.
One 24-hour sample collected at different lactation stages ranging from week 1 postpartum to week 27.
Milk biomarker changes have been used to measure the timing and characteristics of secretory activation in 10 studies.32,33,40,41,45,52,59,73–75 Six of these studies included both milk biomarkers and at least one other measure of secretory activation, including MP and patterns of increase in milk volume.32,39,40,45,52,71 In some studies, a single milk specimen was collected between postpartum days 3–8 to measure Na or the Na/K ratio to predict breastfeeding duration.59,74,75 These studies revealed that a rapid decrease in Na was highly predictive of successful lactation, whereas a protracted elevation in Na or Na/K ratio predicted impaired secretory activation.59,74 For example, Murase et al. concluded that the Na/K ratio on postpartum day seven might predict breastfeeding outcomes for mothers of term infants who perceive insufficient milk supply. 75
Although milk biomarkers enjoy high concurrent and predictive validity (Table 2), having been validated simultaneously in the same mother using patterns of increase in milk volume, it is still unknown whether all or just some biomarkers should be used in research and practice. 41 It is also unknown which parameters should be used to interpret biomarker findings. For example, in three studies, only Na or Na/K ratios were measured and reported.35,59,75 In contrast, research with breast pump-dependent mothers of preterm infants has incorporated all four primary biomarkers and examined the number of hours or days postpartum that different combinations of biomarkers achieved values considered normal for mothers of term infants.40,41 Hoban et al., who measured 12-hourly milk samples over the first 14 days postpartum, reported a dose–response relationship between the number of biomarkers within normal range and pumped milk volume on days 3 and 5 postpartum. 41
Thus, the use of milk biomarkers as a measure of secretory activation holds promise for research and practice, but additional studies are needed to establish normal values and to determine which biomarkers are most predictive of lactation problems in low- and high-risk populations. Milk biomarkers may have limited feasibility for use in low-risk populations due to laboratory analyses, costs, and need for frequent milk sampling during the early postpartum period.
Discussion
To our knowledge, this is the first article to review measures of secretory activation for use in research and practice with a primary emphasis on accuracy and feasibility. Although MP is the most feasible measure with respect to availability and cost, its accuracy has not been established using another measure of secretory activation concurrently for individual mothers. In contrast, patterns of increase in maternal milk volume have been validated with milk biomarkers in both breastfeeding and breast pump-dependent mothers and normal ranges have been established. However, it is not a direct measure of secretory activation because it is influenced by the effectiveness and efficiency of milk removal. The accuracy of serial urinary lactose concentrations has not been established for secretory activation, and this measure lacks feasibility due to the 24-hour urine sampling required to establish patterns of change. Milk biomarkers have been studied singly and in combination and are more accurate but less feasible than are either MP or patterns of increase in maternal milk volume. Although normal postpartum patterns for milk biomarkers have been established, additional research is needed to adapt these measures to routine clinical use.
The findings from this integrative review reveal an inverse relationship between the accuracy of a measure and its feasibility, with the more accurate measures currently being the least feasible. Thus, a priority for research, as well as personalized lactation practice, is to determine which secretory activation measure is appropriately used for which population of mothers, based on maternal risk for impaired secretory activation (Fig. 3). However, this conceptualization should include an updated definition of maternal lactation risk, which has traditionally been based upon whether the infant is in the NICU and/or the mother is breast pump dependent. This approach misses many mothers who are at a significant risk for delayed or impaired secretory activation and subsequent suboptimal lactation outcomes, such as otherwise healthy mothers who are overweight or obese.11,12,16,18,20,21

Matching measure of secretory activation to maternal infant risk model.
Of particular urgency is the need to establish the accuracy of MP. This measure has the highest feasibility for use as a population-based screening tool for early detection of delayed or impaired secretory activation in healthy populations. Top research priority must be given to determining which indicators (e.g., full breasts, leaky breasts, and infant swallowing) to include and whether these indicators require adaptation for different populations. For example, no data affirm that overweight or obese mothers with larger breasts and greater tissue adiposity can accurately assess the same indicators of MP as normal weight mothers or whether breast pump-dependent mothers should use the same indicators as healthy breastfeeding dyads. Studies should target the concurrent validation of MP using milk biomarkers as the accurate standard in individual mothers.
Of the secretory activation measures, patterns of increase in milk volume measure has been studied the most, has acceptable accuracy and feasibility, has established normal ranges through to the first 2 weeks postpartum, and is limited only by being an indirect measure as described. Thus, there is sufficient evidence for the clinical use of in-home test weights in at-risk populations such as mothers with a previous experience of early unplanned weaning or those with risk factors such as obesity, diabetes, polycystic ovarian syndrome, and cesarean delivery. Similarly, intervention research that targets the prevention, diagnosis, and management of impaired secretory activation should incorporate this objective, accurate, and feasible measure rather than the unvalidated measure of MP. However, when the milk removal entity is ineffective or inefficient such as with hand expression or in the case of late preterm/early term infants with suboptimal intraoral suction pressures, test weights may not distinguish between problems with secretory activation versus those related to milk removal.
Finally, the development of clinical science to support the use of milk biomarkers with mothers at the greatest risk for delayed or impaired secretory activation is an important research priority. At highest risk are breast pump-dependent mothers of preterm infants with multiple antepartum and intrapartum risk factors, such as excessive blood loss or pregnancy-induced hypertension and its resultant pharmacotherapy. Two separate studies with milk biomarkers in this population have revealed high rates of impaired secretory activation, as well as the feasibility of collecting sequential milk samples from mothers with hospitalized infants.37,40 Furthermore, innovative research by Hoban et al. 41 has demonstrated the potential clinical utility of milk biomarkers in breast pump-dependent mothers.
Research in this area should define normal ranges for specific biomarkers, determine which biomarker or combination of biomarkers should be measured, and inform the frequency and duration of testing. For example, Hoban et al. demonstrated that achievement of secretory activation, as measured by milk biomarkers, was not permanent in all mothers and was easily reversed during the first 2 weeks postpartum with suboptimal pumping behaviors. 41 As a minimum standard, intervention studies in this population should measure secretory activation with milk biomarkers rather than only with pumped milk volumes. Similarly, there is a need to increase the feasibility of measuring milk biomarkers with respect to cost and ease of use. Hoban et al. used LAQUA Twin Sodium and Potassium Meters (Horiba, Ltd, Kyoto, Japan) in a laboratory setting, but these instruments enjoy high feasibility for potential adaptation in the clinical setting for point-of-care measurement of Na or Na/K ratio. 41 This conclusion was supported in a recent report by Lai et al. 76 who established the accuracy of these instruments and concluded that these ion selective probes hold promise for the diagnosis of low milk supply and/or mastitis.
A strength of this article is the integration of original studies, in-depth search strategies, and the review of all studies by a minimum of two authors. Our review was limited by the relatively few studies that met inclusion criteria, but this reflects the current underdeveloped state of the research in this field. An additional limitation is that we chose not to include measurement of secretory activation using RNA-sequencing analysis of the human milk fat layer transcriptome that identifies gene expression profiles during the different stages of lactation as detailed by Lemay et al. 77 because these technologies are still under development and refinement.
Summary
The biologic changes in milk synthesis and secretion that characterize the first 2 weeks postpartum have been well delineated, but this science has not been integrated into clinical practice and research with the intent of identifying and managing delayed or impaired secretory activation. As increasing numbers of mothers have health conditions that elevate the risk of lactation problems originating in the first 2 weeks postpartum, these clinical and research gaps must be addressed. Research should target establishing the accuracy of MP for heterogeneous populations using already-validated measures of patterns of increase in maternal milk volume in intervention studies. In addition, developing the translational science for the use of milk biomarkers in populations at the highest risk for delayed or impaired secretory activation must be a priority.
Footnotes
Authors' Contributions
All authors made substantial contributions to and approved the systematic review.
Disclosure Statement
No competing financial interests exist.
Funding Information
2017 Trainee Expansion Program, supported jointly by the International Society for Research in Human Milk and Lactation (ISRHML) and Family Larsson Rosenquist Foundation; 2018 Golden Lamp Society Dissertation Award, Rush University College of Nursing.