
Abstract
Background:
There is increasing evidence that premature newborns and infants with low birth weight can benefit substantially from an exclusive human milk-based diet (EHMD), consisting of human milk supplemented with a pasteurized donor human milk-derived fortifier. However, compared with the standard infant diet, EHMD also represents a significant added cost to the hospital and/or health system, thereby raising important questions about the economic feasibility of incorporating EHMD into newborn care.
Design:
We conducted a cost analysis and estimated the potential cost savings to a Canadian tertiary hospital based on the attributable complications averted from EHMD among low-weight neonates. A meta-analysis was performed to derive input parameters. A probabilistic analysis was conducted to determine the probability that EHMD is cost saving and 95% confidence interval (CI) around our estimates.
Results:
Our findings show that providing EHMD to preterm infants under 750 g at birth and at the highest risk of developing major complications is likely to be cost saving in the amount of $107,567 (95% CI: −145,229 to 360,362) per year. Extending EHMD to higher weight classes may be economically feasible depending on the pricing of the human milk-derived fortifier and the baseline risk of complications in the hospital setting.
Conclusions:
This comprehensive study provides critical insight for hospital-based decision makers to evaluate the potential gains and uncertainties associated with improved nutritional care for neonatal patients.
Introduction
The care of very-low birth weight infants (VLBWI; below 1,500 g) has long been known to be associated with both high health care costs and both stress and reduced quality of life for parents. 1 Efforts to identify safe and impactful ways to improve outcomes in this population are needed. There exists evidence suggesting that the provision of breast milk is a gold standard approach to ensuring nutrition for healthy full-term infants.2–4 It is also associated with improvements in immune defense, 5 neurologic development, 6 gastrointestinal function, 7 and reduced risks of adverse outcomes, such as necrotizing enterocolitis (NEC),8,9 retinopathy of prematurity (ROP), 10 sepsis, 10 bronchopulmonary dysplasia (BPD), 10 feeding intolerance, 11 and mortality. 12 Donor milk (i.e., provided in place of or in addition to milk from the child's mother when needed) also retains many of these protective effects. 13
Recommendations from both the Canadian Pediatric Society 14 and American Academy of Pediatrics 15 support the feeding of prematurely born infants with human milk. Current practice in many hospitals is to add a bovine milk-based fortifier to human milk to provide the increased calories required for adequate VLBWI growth. 16 An exclusive human milk-based diet (EHMD), defined as a diet consisting of the infant's mother's own milk, supplemented with pasteurized donor human milk when necessary, as well as a pasteurized donor human milk-derived fortifier, can offer considerable health benefits for prematurely born infants compared with a diet containing any cow's milk-based formula or fortifier (BOV), including reduced rates of NEC, ROP, sepsis, and BPD.17–20 The bioactive constituents of human milk have also been noted in downregulating inflammatory response at the intestinal cell surface, offering protection to infants from a cascade of steps that can move toward the incidence of major complications.21,22 Currently, pasteurized donor human milk-derived fortifier is available only from Prolacta Bioscience, Inc. and was approved by Health Canada in 2010. However, pasteurized donor human milk-derived fortifier represents a significant added cost compared with other bovine-based fortifiers, meaning health care system and hospital decision makers who are faced with limited resources and competing resource demands must determine whether the improved outcomes for patients also represent potential for cost recovery that would make human milk-derived fortifier not only clinically desirable but economically feasible as well.12,23
This study aimed to assess the financial implications of providing an EHMD, including human milk-derived fortifier (i.e., Prolacta®), to newborns who were admitted to the Neonatal Intensive Care Unit (NICU) at The Ottawa Hospital (TOH).
Methods
We performed a cost analysis using a stochastic decision tree framework to compare the expected total hospital costs for newborns receiving EHMD (human milk plus human milk-derived fortifier) compared with the current standard of care (human milk plus bovine milk-derived fortifier) from a hospital's perspective. Our base case analysis was providing EHMD only to the most extreme low birth weight infants (<750 g). We performed additional scenario analysis on each weight stratification, costing structure, and incremental cost of EHMD from $0 to $18,000 per patient.
Our analysis included all births at TOH from January 1, 2013, to December 31, 2017. We obtained data regarding patient birth weight, length of stay (in tertiary NICU and/or other neonatal care units), diagnostic codes associated with the conditions of interest, and case costing from hospital health administrative databases. The case costing system estimates total hospital costs by taking the sum of costs of each functional center, such as medications, laboratory tests, and current provision of total nutritional requirement, incurred by each patient. The system is based on a standardized costing methodology developed by the Ontario Case Costing Initiative, according to the Canadian Institute for Health Information Management Information Systems guidelines. 24 Only costs borne to the hospital were considered for this analysis, meaning that physician costs and discharge to other level III care institutions, such as transport team costs to the Children's Hospital of Eastern Ontario (CHEO) or rehabilitation, were not included. Our base case analysis used variable costs, as these are the costs directly incurred from health care utilization, which are the most likely sources of operational savings. Additional analysis was done using direct cost that attributes hospital costs only related to the immediate care of patients, and total hospital cost savings, in which we assume the hospital can leverage savings from all sources, including some portion of unused fixed assets such as beds and nursing time.
Average patient costs using the current standard of care were calculated according to birth weight category and complication type. The average cost per patient by weight category was the weighted average of the proportion of patients within each complication: NEC, ROP, BPD, sepsis, or other (includes no complications). These complications were identified using the diagnostic codes in the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (NEC = P77, ROP = H351, BPD = P271, sepsis [Newborn] = P360–9). We categorized patients as having complication if they had any of these codes during their hospital stay. Many patients may be transferred between NICU and non-NICU settings, depending on their clinical condition. We report the costs for patients split between NICU and non-NICU; however, our cost analysis combines these two costs according to the average cost by weight category and complication status. All cost saving analyses were adjusted to reflect the marginal difference in the cost of the complication and the cost borne by patients within the same weight category who did not develop any complication. Changes in expected patient costs from switching to EHMD were based on relative risk reductions of the proportion of patients who develop the complications of interest, thereby changing the weighted cost for the average newborn patient at TOH.
TOH has adopted a nutrition policy that favors the use of human milk (a mother's own milk and/or donor human milk) in the early feeding of VLBWI. However, if a newly born infant requires supplemental nutrients to be added to the diet, a bovine milk-derived fortifier is currently in use. Therefore, in this study, the only additional cost under consideration to achieve EHMD is the provision of a human milk-derived fortifier, that is, Prolacta. Studies reported a variety of prices for human milk-derived fortifier.12,25 Based on these studies and discussion with a representative from Prolacta Bioscience, Inc., a neonatologist who is part of our team (E.F.), and expert nutritionists of other centers in Canada who use the product, we assert an average total cost of $13,000 per patient to provide human milk-derived fortifier and performed scenario analysis of this cost from $0 to $18,000 per patient. All costs were inflated to 2019 dollars (CAD).
Several parameters of this model were informed by a targeted literature review that was conducted using PubMed. The literature search was performed to identify the effects of an EHMD with a human milk-based fortifier compared with a diet of human milk fortified with BOV on major complications among VLBWI. Appendix A1 includes search strategy details (See Appendix Table A1). All data on incidence of major complications for VLBWI who were fed EHMD and BOV diet were extracted from these studies and meta-analyzed using a random-effects model.
Results of the cost analysis are shown as the mean results of a probabilistic analysis that varied all costs, incidence rates, and treatment effect parameters according to their 95% confidence interval (CI) and distributions using a Monte Carlo approach with 10,000 iterations. We derived the probability of EHMD being cost saving based on the added cost of implementing exclusive human milk (EHM) over BOV by bootstrapping the probabilistic analysis according to the proportion of iterations where the expected cost saving was positive.
Results
From January 1, 2013, to December 31, 2017, a total of 31,335 newborns were admitted at TOH. Of these, 3,543 newborns were classified as low to extremely low birth weight, and 818 were diagnosed with one or more complications of relevance to the current study, representing an average annual prevalence of 2.6%. Complication rate by birth weight category is negatively associated with birth weight (Table 1). Table 2 presents the average hospital cost per case and length of stay according to complication, birth weight, and care unit (NICU versus non-NICU).
Incidence of Major Complications at The Ottawa Hospital by Birth Weight Category, 2013–2017
BPD, bronchopulmonary dysplasia; NEC, necrotizing enterocolitis; ROP, retinopathy of prematurity.
Hospital Cost per Case, by Complication Type and Birth Weight Category, 2013–2017
—, no observations in that category; LOS, length of stay; NICU, neonatal intensive care unit.
All studies found in our review included in our final analysis used Prolacta as the human milk-derived fortifier as this is the only such product on the market. Using an average added cost of $13,000 to provide human milk-derived fortifier to newborns for the duration of their admission, we estimate the added variable cost to the hospital to provide EHMD to all preterm infants with a birth weight of less than 750 g is $391,721 per year. Providing EHMD for these infants is expected to avert six cases of major complications (NEC, sepsis, ROP, or BPD) and over 313 total days of NICU admission days, resulting in $499,287 in variable cost savings, netting a $107,567 benefit for the hospital. Table 3 shows these base-case results, including 95% CIs, and results using alternative price structures. Table 4 presents the net benefit from EHMD, assuming different average prices of human milk fortifier per patient, according to birth weight categories that receive EHMD. The potential cost savings from an EHMD are highly dependent on the weight category of infants for whom human milk fortifier replaces the standard-of-care bovine fortifier.
Cost Saving Analysis for Providing Exclusive Human Milk-Based Diet to All Infants <750 g Birth Weight at The Ottawa Hospital 2013–17 (95% Confidence Interval)
Complications consisted of NEC, sepsis, or BPD.
BOV, cow's milk-based fortifier; CI, confidence interval; EHMD, exclusive human milk-based diet; LOS, length of stay.
Net Variable Cost Savings to the Hospital, by Human Milk-Derived Fortifier Price and Birth Weight Category

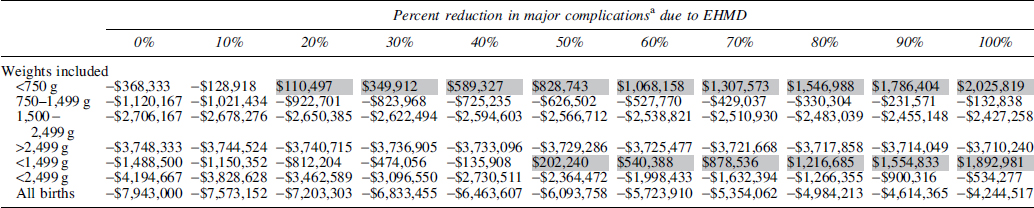
Table 5 illustrates the expected net savings for the hospital according to the effectiveness of the human milk-derived fortifier (the percentage of major complication cases averted) assuming an average added cost of $13,000 per patient to receive EHMD. If the hospital provided EHMD to preterm infants with a birth weight less than 750 g, EHMD is cost saving assuming it prevents at least 16% of major complications. EHMD could be cost saving when provided to infants weighing less than 1,499 g at birth if at least 47% of major complications are averted. Of course, if the average per patient price of providing human milk fortifier was less than $13,000, these minimum effectiveness thresholds would also decrease.
Net Variable Cost Savings to the Hospital, by Prolacta Effectiveness and Birth Weight Category
Discussion
This study highlights that the provision of EHMD to preterm infants at highest risk of developing major complications—those under 750 g at birth—is likely to be cost saving from a hospital perspective by preventing major complications. Assuming the most conservative estimate that only variable costs associated with patient care can be recovered by the hospital, we estimate that level III NICUs similar in scale and services to those of TOH would save roughly $107,000 per year. Extending EHMD to additional weight categories is likely to avert more complications; however, there is not strong evidence that human milk fortifier will “pay for itself” through cost recovery, let alone present net savings to the hospital. The primary reason for this is that as one targets less extremely preterm infants for EHMD, the absolute number of patients receiving human milk fortifier is increasing, however, the relative share of complications averted is decreasing, causing the marginal net cost of providing human milk fortifier per infant to rise rapidly. A subgroup analysis found that the cost saving results were consistent across all individual complications (results not shown), although with lower total expected savings. Despite some major complications being quite rare, we find it is still cost saving to apply EHMD for infants under 750 g at birth.
Although our study was based on a single Canadian center, recent costing studies conducted in the United States12,25,26 were consistent with our findings. Their results support the evidence that the use of EHM fortifier is linked with the reduction of severe short- and long-term health complications, therefore increasing the cost saving per baby. The most recent modeling study by Hampson et al., 26 for example, also found that providing EHMD to VLBWI was highly cost effective in the United States. Despite the differences in study designs and cost settings, our study provides encouragingly similar findings on the incidence thresholds necessary before EHMD becomes cost saving, and our sensitivity analyses found similar factors driving model uncertainty. From this we can be reasonably confident in the potential generalizability of advice to provide EHMD to the highest risk infants.
There are several assumptions in our analysis. First, the base case analysis assumes that the average cost of providing human milk fortifier for the duration of the patient's admission is $13,000. The price structure for human milk is affected by birth weight, hospitalization characteristics, length of stay for the infant, and so on, each of which is highly heterogeneous. In practice, providing EHMD is a variable cost that will be dependent on total duration in hospital, however, we apply a fixed cost primarily due to the fact that the manufacturer pricing similarly applies an average cost per patient model that accounts for variance in time on treatment, which we believe is reasonable for this type of decision model. Furthermore, the unit price of human milk fortifier varies across the literature as well as health care institutions that the authors contacted, introducing additional uncertainty to the cost parameter. To address this, our study provides Table 4 that estimates cost savings according to average cost of human milk-derived fortifier, that is, Prolacta per patient. This allows visualization of the scale of savings associated with different price points and can hopefully aid decision makers in determining whether EHMD is suitable based on their capacity to internalize the cost of human milk fortifier.
A second assumption is that TOH represents other Canadian hospital settings. Other institutions may not exclusively use human milk, and therefore, the introduction of human milk-derived fortifier could have a different scale of impact on their patient population. As discussed above, the complication rate and number of EHMD-eligible patients have direct impacts on the economic feasibility of introducing human milk fortifier, meaning institutions that see higher volumes of inborn extremely preterm cases may see higher cost saving potential from providing EHMD.
Finally, TOH often transfers surgical patients and those requiring subspecialty pediatric consultation to CHEO; however, the costs incurred by other institutions were excluded, and therefore, the potential savings from prevention is likely underestimated. This is not a limitation in our methodology since we specifically set out to determine the savings from the EHMD-providing hospital perspective. However, this does raise the possibility that a multi-institutional perspective that considers the complete care pathways for preterm infants could increase the economic feasibility of providing EHMD.
Results of the probabilistic sensitivity analysis found that variability in case costing (Table 2) introduced the largest amount of uncertainty into the model. This is predominantly due to the heterogeneity of outcomes for neonatal patients; we partially addressed this by presenting our results stratified by birth weight to more appropriately reflect the associated outcomes for infants with shared risk factors. The second-largest source of uncertainty is the relative risk estimates that were pooled using a random-effect meta-analysis (Appendix A1; Appendix Tables A2–A4). To address this source of uncertainty, we considered how the net benefit calculation would change according to the relative effectiveness of the human milk-derived fortifier to avert major complications (Table 5).
This study focused on a single risk category, birth weight, as its cohort stratification strategy because it simplified the presentation of evidence for publication, and birth weight represents a risk factor that is easily assessed for targeting of interventions for any hospital. Implementation of EHMD in the hospital can be more nuanced than weight stratification in ways that can improve the economic feasibility of providing human milk fortifier to a larger percentage of preterm infants. It is possible to establish a simple evidence-informed decision tool of patient characteristics that indicate high risk of developing a major complication to determine whether an infant should be provided EHMD, among which birth weight is only one factor. While beyond the scope of this study, such a decision tool has the potential to increase the accessibility of EHMD for high-risk patients while providing a higher marginal return to the hospital.
It should be noted that our study only considers a limited set of potential health benefits of human milk-based fortifier. We perform an exploratory analysis (Table 3) by considering direct costs and all hospital costs associated with patient care (these costs are broken down explicitly in Table 2). This analysis provides a more complete picture of the potential savings in the unique circumstances when an institution can recover costs that are usually fixed. For instance, it is usually the case that an unused NICU bed does not confer major savings to the hospital since the cost of the bed and a staff for the ward is incurred regardless of whether a patient is there. Consequentially, total costs of patient care are not regularly helpful for calculating actual hospital savings, however, it can be helpful for illustrating the scale and share of the institutional costs incurred.
Although the full extent to which human milk-based fortifier affects health-related quality of life remains unknown, there is increasing evidence that supports the use of an EHMD in very-low birth weight preterm infants for improved long-term outcomes.12,27,28 Beyond this, there are societal benefits for parents and children that are not captured. When this evidence becomes available, a cost-utility analysis that considers the broader health system and societal perspective would be a valuable addition.
EHMD is increasingly sought after in hospitals, as it has shown to contribute significantly to the health of premature and low birth weight infants. There is, however, significant cost and decision uncertainty associated with adopting a full human-based milk diet that hospital decision makers should be aware of when forced to consider the economic trade-offs. Reduction in the cost of human milk-derived fortifier (Prolacta), cost sharing across institutions that receive discharged infants, and improvements in the effectiveness of EHMD are all promising avenues that can increase the economic feasibility of adopting EHMD to the largest possible proportion of infants in need.
What is already known on this topic
There is growing evidence that an EHMD has significant clinical benefit to premature and low birth weight newborns. Providing EHMD is expensive, but may be economically beneficial when considering the severe complications it can avert. Evidence uncertainty and insufficient decision tools leave heath care institutions unable to make informed decisions on whether to provide EHMD, and to which patients.
What this study adds
We compiled existing evidence on the benefits of human milk-derived fortifier to characterize the clinical and economic benefits from EHMD, as well the degree of uncertainty. We performed an economic analysis that provides a risk-stratified estimate of the economic feasibility of EHMD from a hospital perspective. Finally, we presented evidence that can aid institutions in generalizing our economic analysis to their institutional and clinical contexts.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This project received funding from IQ@TOH.