
Abstract
Background:
To evaluate the efficacy of a multidisciplinary quality improvement intervention to promote mother's own milk feeding and reduce necrotizing enterocolitis (NEC) in very low-birth-weight infants.
Materials and Methods:
We conducted a pre (January 2014 to March 2015)–post (April 2015 to June 2016), nonrandomized, interventional cohort study of infants born at <1,500 g birth weight and admitted to the Fudan University Children's Hospital level III neonatal intensive care unit in Shanghai. The intervention included establishing a breast milk promotion team and breast milk pumping room, educating staff and parents, and distributing teaching materials. The primary outcome was breast milk feeding rate. Secondary outcomes included incidences of NEC, NEC needing surgery, mortality, and time to full enteral feeds.
Results:
A total of 488 infants (210 baseline, 278 intervention) <1,500 g were enrolled. The intervention group had significantly increased feeding rates for any mother's milk (34.76% vs. 80.58%; p < 0.01) and high-volume mother's milk (≥50% of feeds; 22.86% vs. 61.15%; p < 0.01), and decreased incidence of NEC needing surgery (7.62% vs. 3.24%; adjusted odds ratio [OR] 0.32, 95% confidence interval [CI] 0.14–0.76). There were no significant differences in rates of mortality (0.5% vs. 1.49%; adjusted OR 2.10, 95% CI 0.22–19.6), NEC (10.00% vs. 7.55%; adjusted OR 0.59, 95% CI 0.31–1.14), and time to full enteral feeds (20.18 ± 1.67 days vs. 24.15 ± 1.65 days; adjusted OR = 1.09, 95% CI 0.99–1.21).
Conclusions:
Our quality improvement initiative increased the consumption of mother's own milk and reduced the severity of NEC in very low-birth-weight infants.
Introduction
Human milk provides many health benefits in early infancy that extend into adulthood.1–3 The nutritional benefits of human milk are well established, especially for infants born preterm.4–6 In 2012, the American Academy of Pediatrics issued a statement on breastfeeding and declared that clinicians should recommend feeding mother's milk to preterm infants. 5 Further, numerous strategies have been established to facilitate breastfeeding practices in U.S. hospitals and communities. 7 In developed countries, mother's milk is promoted by all professional organizations and is the gold standard for nutrition in the neonatal intensive care unit (NICU). 8 In contrast, despite a growing body of evidence advocating the use of mother's milk, almost all babies admitted to NICUs in China are still fed infant formula. 9 The prevalence of mother's milk feeding in Chinese NICUs is rarely reported, but 1 multicenter observational study based on 10 tertiary NICUs in China found that only 13.6% of preterm infants received any mother's milk during their hospitalization. 10
Previous research from developed countries has shown that mother's milk feeding rates can be significantly improved by implementing structured, evidence-based practices to promote mother's milk use in the NICU.7,11,12 However, quality improvement initiatives to improve mother's milk feeding in NICUs in China are lacking.
We carried out a multidisciplinary quality improvement initiative aimed at increasing the prevalence of mother's own milk feeding in infants born at <1,500 g in the tertiary NICU at Children's Hospital of Fudan University (FUCH) in Shanghai, China. We evaluated the effect of our mother's milk promotion program by comparing the mother's milk consumption rates and neonatal outcomes of infants both before and during the initiative.
Materials and Methods
Context
Our before-and-after study was conducted in the level III NICU at FUCH in Shanghai, China between January 1, 2014 and June 30, 2016. The FUCH NICU treats only out-born infants, has 50 beds, and is staffed at all times by onsite, board-certified physicians and neonatologists. Our study compared the feeding statuses of infants with a birth weight <1,500 g born during the baseline period (January 1, 2014 to March 31, 2015) versus during the implementation of the mother's milk promotion period (April 1, 2015 to June 30, 2016).
Study population
We included in our study all infants with a birth weight <1,500 g and transferred to the FUCH NICU within 24 hours after birth from January 1, 2014 through June 30, 2016. We excluded infants with mother's milk feeding contraindications, major congenital anomalies, or severe illness with contraindications for feeding; and those who were discharged against medical advice. The 210 infants admitted between January 1, 2014 and March 31, 2015 were in the control group, and 278 infants admitted between April 1, 2015 and June 30, 2016 were in the intervention (mother's milk promotion) group.
Mother's milk promotion intervention
We adopted the evidence-based practice for improving quality (EPIQ) program developed by the Canadian Neonatal Network (CNN). 13 A 2-day EPIQ training workshop was conducted by the CNN team at FUCH before commencing the mother's milk promotion project. A local EPIQ team was set up, which comprised key physicians and nursing leaders in the NICU. The EPIQ team reviewed the literature on mother's milk promotion and practice strategies previously used by CNN and then developed the intervention bundles based on our hospital's reality.
The mother's milk promotion program to increase the use of mother's own milk in the NICU was implemented at the FUCH between April 1, 2015 and June 30, 2016 and included the following interventions:
(1) Multidisciplinary mother's milk promotion team
We created and trained a multidisciplinary mother's milk promotion team to increase NICU mother's milk feeding in support of this quality improvement project. The team comprised two neonatologists, five nurses, and one nutritionist who were empowered to regularly monitor the NICU mother's milk feeding rate, communicate with parents about mother's milk feeding, and provide parents with education and lactation support.
(2) Staff education
To learn new methods to support mother's milk production and breastfeeding, we sent two neonatal nurses from the FUCH mother's milk promotion team to Mount Sinai Hospital in Toronto, Ontario, Canada, where they received 2 months of training as a lactation coordinator and a lactation consultant. Meanwhile, using the “train-the-trainer” method, two experienced lactation consultants from Mount Sinai Hospital visited the FUCH NICU for 2 weeks to provide the local mother's milk promotion team with training in methods to support mother's milk production and breastfeeding in the NICU. In turn, the FUCH mother's milk promotion team then trained all other NICU staff on the importance of mother's milk feeding in the NICU and ways to support mothers who are learning to pump milk and breastfeed their infants.
(3) Teaching materials for parents
Teaching materials were designed to educate parents of very low-birth-weight infants about the potential benefits of mother's milk feeding for preterm infants and provide tips to obtain early colostrum, strategies for mother's milk pumping and hand expression at home, and guidance on the proper storage and transport of mother's milk. These teaching materials were also available on the NICU's social media platform (WeChat) and as written brochures. The written materials were distributed to all parents of very low-birth-weight infants in the NICU along with a mother's milk transportation package, which contained an ice bag and a milk preservation bag to facilitate milk transportation from home to the NICU.
(4) Breast pumping room
To promote mother's milk pumping and breastfeeding in the NICU, we designated a private and quiet area in the NICU as the breast pumping room. We decorated and equipped this room with two hospital-grade mother's milk pumps (Medela Symphony) and comfortable chairs to support mothers pumping milk and feeding their babies. This breast pumping room was available 24 hours a day with a lactation nurse available to give assistance and advice.
(5) Continuous parent education and communication.
One week before infant discharge, parents were invited to the NICU to spend several hours each day with their infants. The mother's milk promotion team encouraged mothers to breastfeed and provided practical lactation counseling and support until their infant was discharged. Also, we created a communication group on the WeChat platform for the mother's milk promotion team and the families to communicate efficiently. Meanwhile, another intended function of this platform was to allow parents of very low-birth-weight infants to help and support each other as they gained confidence.
Data collection
Informed written consent was obtained from parents after the researchers explained to them the study's purpose and processes and informed them that participation was voluntary and study data would be kept confidential. Demographic details and data on feeding type, mother's milk intake, time to full enteral feeds, and necrotizing enterocolitis (NEC) during hospitalization were recorded prospectively for each study patient. A trained research physician reviewed the data collection sheets and medical records for potential errors and confirmed each diagnosis. The staff responsible for data collection and analysis was not aware of the mother's milk promotion program. Written consent was obtained from parents for both phases of the study. The Research Ethics Board at FUCH approved the study. The study was registered with the U.S. National Institutes of Health (ClinicalTrials.gov) with number NCT02897388.
Outcome measures
The primary outcomes were the mother's milk feeding rate and the colostrum feeding rate during hospitalization. Mother's milk feeding during hospitalization was divided into three categories: (1) any mother's milk, (2) high-volume mother's milk, and (3) exclusive mother's milk. Any mother's milk was defined as any mother's milk received by any means during the hospitalization, irrespective of the amount of mother's milk consumed. High-volume mother's milk was defined as mother's milk received for at least 50% of feeds during the hospital stay. Exclusive mother's milk was defined as only mother's milk received during hospitalization. The colostrum feeding rate was defined as the percentage of infants who received mother's own milk at least once within 7 days after birth.
The secondary outcomes were the rates of NEC, surgical NEC, mortality, nosocomial infection, periventricular leukomalacia (PVL)/intraventricular hemorrhage (IVH), retinopathy of prematurity (ROP), and bronchopulmonary dysplasia (BPD); time to full enteral feeds (measured in days after birth); and days in the NICU. We defined and classified NEC according to modified Bell's criteria (stage II or higher) 14 ; surgical NEC was defined as NEC that required surgical intervention because necrosis extended through the bowel wall and resulted in perforation. A multidisciplinary team, which included a surgical consult, assisted the neonatology team in deciding whether and when surgical intervention was required. Nosocomial infection was defined by using the Center for Disease control criteria. 15 ROP was classified according to the Committee for Classification of Retinopathy of Prematurity. 16 BPD was defined as need of supplemental oxygen or mechanical ventilation at 36 weeks postmenstrual age. 17 PVL/IVH was diagnosed based on ultrasound. Full enteral feeds were defined as reaching 120 mL/kg/day of feeds with any milk. Mother's milk was fortified when the feeding volume reached 100 mL/kg according to our unit-based practice. Donor breast milk was not available, and preterm formula was used when a mother's own milk was unavailable or in short supply during our study period. All definitions and feeding strategies were consistent throughout the entire study period.
Statistical analysis
For statistical analysis, the baseline period was January 1, 2014 to March 31, 2015 and the mother's milk promotion period was April 1, 2015 to June 30, 2016. Data were recorded on case report sheets and entered into databases, and all the data were crosschecked. The data were analyzed by using SPSS statistical software version 16.0 (IBM SPSS Statistics, Armonk, NY). Categorical variables were summarized by using counts and percentages, whereas continuous variables were summarized by using means and standard deviations. Categorical variables were compared by using chi-squared tests, and continuous variables were evaluated by using Student's t-tests. To prevent skewing of the results by data from very preterm infants in the intervention group, we stratified infants of >28 weeks' and 23–28 weeks' gestation separately and conducted multivariable regression analyses adjusted for gestation to compare the short-term outcomes between baseline and intervention groups. Odds ratio (OR), 95% confidence intervals, and p-values were determined for all outcomes. The level of significance was set at p < 0.05.
Results
Patient characteristics
We included 210 infants <1,500 g born during the baseline period between January 1, 2014 and March 30, 2015; and 278 infants born during the intervention period from April 1, 2015 to June 30, 2016. The intervention group included significantly more infants with a birth weight <1,000 g, a lower birth weight on average, and more infants born at 23–28 weeks' gestation than the intervention group (Table 1).
Infant Characteristics
SD, standard deviation.
Mother's milk feeding rates
The any mother's milk feeding rates for infants born at <1,500 g more than doubled, from 34.7% at baseline to 80.6% (p < 0.01) during the intervention period (Table 2). None of the infants achieved exclusive mother's milk feeding during their hospitalization at baseline, but the rate increased to nearly 20% (p < 0.01) after the intervention. In addition, both high-volume mother's milk and colostrum feeding rates increased significantly from baseline after the implementation of our mother's milk promotion program (Table 2).
Mother's Milk Feeding Rates
Any mother's milk was any mother's milk received by any means during the hospitalization, irrespective of the amount of mother's milk consumed.
High-volume mother's milk was mother's milk for at least 50% of feeds during the hospitalization.
Exclusive mother's milk was only mother's milk received during hospitalization.
Colostrum was the percentage of infants who received mother's own milk at least once within 7 days after birth.
Neonatal outcomes
After implementation of the breast milk promotion program, NEC (≥stage 2) rates decreased from 10% during baseline to 7.55% during intervention (Table 3). This reduction in NEC (≥stage 2) did not reach statistical significance, but the incidence of surgical NEC decreased significantly from 7.62% at baseline to 3.24% postintervention (Table 3). The rates of nosocomial infection, ROP, and BPD; time to full enteral feeds; and days in the NICU were increased during the intervention with univariate analysis (Table 3). The trends for high-volume mother's milk consumption and NEC incidence are shown in Figure 1.
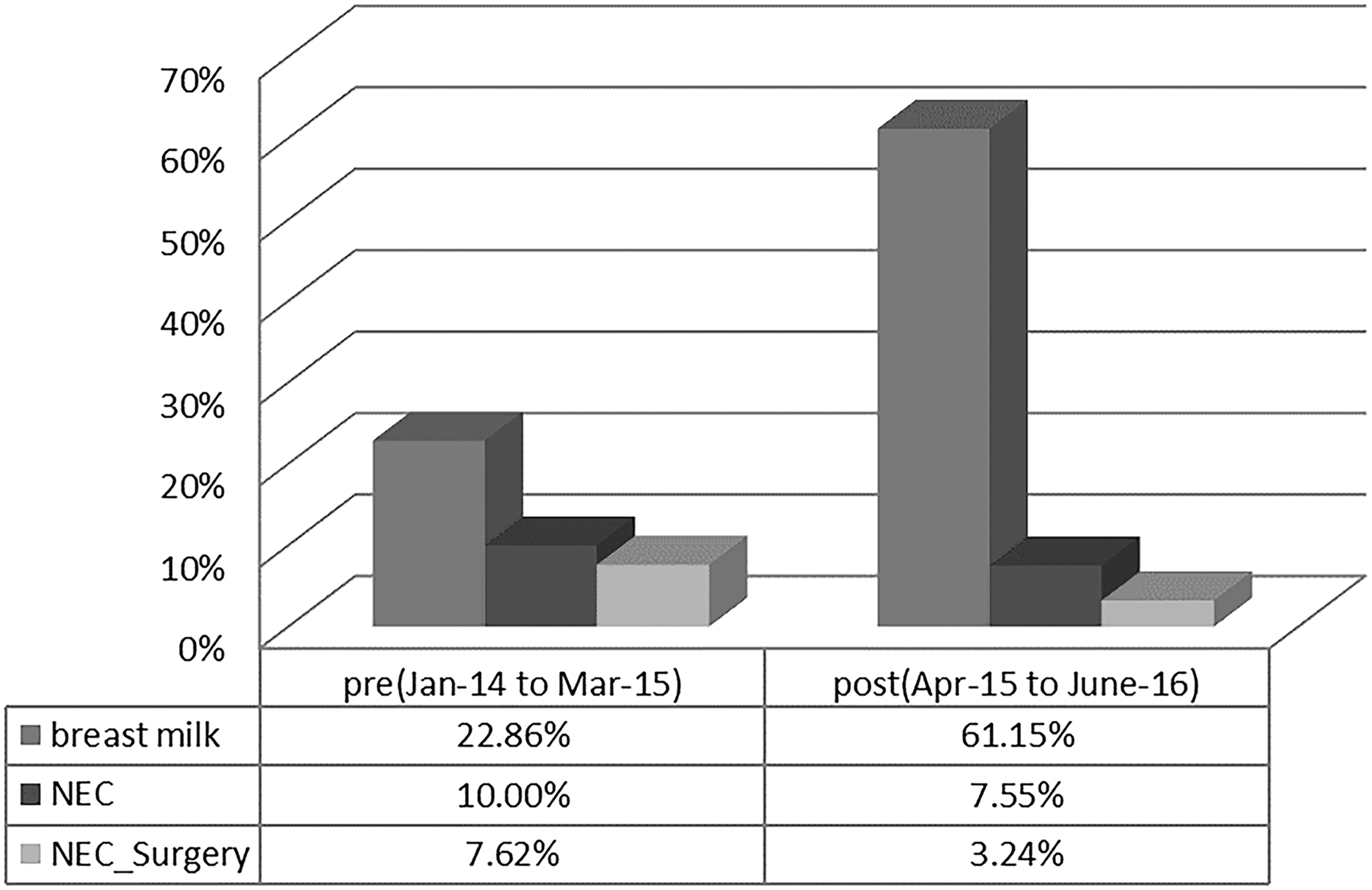
Trends for high proportions of mother's milk consumption and NEC incidence from preintervention to postintervention. NEC, necrotizing enterocolitis.
Univariate Analysis for Neonatal Outcomes
BPD, bronchopulmonary dysplasia; CI, confidence interval; n, number in category; N/A, not applicable; NEC, necrotizing enterocolitis; NICU, neonatal intensive care unit; PVL/IVH, periventricular leukomalacia/intraventricular hemorrhage; ROP, retinopathy of prematurity; SD, standard deviation.
Mortality
There was no significant difference in mortality between our study groups (Table 3). However, one death during the baseline period was related to intestinal perforation secondary to severe NEC; this patient finally experienced multiple organ dysfunction syndrome even with emergency surgery. Of the four deaths that occurred during the intervention period, none was caused by NEC.
Decreased odds of surgical NEC
To adjust for confounding factors, we calculated adjusted ORs for the secondary outcomes (Table 4). Before adjusting for confounding factors, the odds of surgical NEC were significantly decreased and the odds of nosocomial infection, ROP, BPD, time to enteral feeds, and duration of hospital stay were significantly increased postintervention. However, after adjusting for gestational age, there were no significant differences in any of the outcomes, with the exception of surgical NEC, which remained significantly decreased postintervention (Table 4).
Adjusted Analyses for Neonatal Outcomes
ORs for the mean baseline outcome versus mean intervention outcome.
Adjusted ORs were based on multiple logistic regression adjusted for gestational age.
Logistic regression could not be applied, because there were no deaths at ≥29 weeks' gestational age.
Raw ratios for the mean postintervention outcome versus mean preintervention outcome.
Adjusted ratios were based on multiple linear regression adjusted for gestational age.
BPD, bronchopulmonary dysplasia; CI, confidence interval; N/A, not applicable; NEC, necrotizing enterocolitis; NICU, neonatal intensive care unit; OR, odds ratio; PVL/IVH, periventricular leukomalacia/intraventricular hemorrhage; ROP, retinopathy of prematurity.
Discussion
We completed a quality improvement initiative to promote the use of mother's milk in a Chinese NICU for infants born at <1,500 g. Comparing mother's milk consumption rates and neonatal outcomes from the baseline period with the intervention period, we found that our quality improvement initiative resulted in a significant increase in mother's milk consumption by very low-birth-weight infants during the intervention period in all the categories assessed. In particular, exclusive mother's milk consumption increased from 0% during the baseline period to 20% during the intervention period, and the percentage of infants born at <1,500 g who received any breast milk more than doubled to 80.6%. In addition, the rates of NEC decreased, although not significantly; and the odds of surgical NEC were significantly decreased, even after adjusting for gestational age.
Our results are consistent with previous studies in developed countries that showed that multidisciplinary quality improvement interventions in the NICU can significantly promote breast milk consumption18,19 and reduce the incidence of NEC.7,11 In a multicenter quality improvement project, Lee et al. 7 demonstrated that implementation of a breast milk change package by a collaborative of 11 NICUs resulted in a significant increase in breast milk feeding (from 54.6% at baseline to 64.0% postintervention) and a decrease in NEC (from 7.0% at baseline to 2.4% postintervention) that was sustained over an 18-month period. A recent systematic review and meta-analysis also confirmed that mother's milk provided a clear protective effect against NEC via breast milk oligosaccharides and other bioactive components.20,21
Although BPD, ROP, and nosocomial infection; duration of NICU stay; and time to full enteral feeds all increased, this was likely because there were more extremely preterm and very preterm infants in the intervention versus baseline group. Indeed, after adjusting for gestational age, there were no significant differences in all of these outcomes. However, for the subgroup of infants born at 23–28 weeks' gestation, there was a significant increase in the time to full enteral feeds in the intervention group compared with the control group even after adjustment. It is possible that this is because there were more infants in the intervention group who were small for gestational age, had higher Clinical Risk Index for Babies (CRIB) II scores or had hemodynamically significant PDA.22,23 Unfortunately, we did not have this information available in this study. Other studies in Germany 24 and the United States 25 suggested that breast milk feeding was associated with reduced risks of BPD, ROP, late-onset sepsis, and earlier full enteral feeds achievement. However, it is possible that those studies involved exclusive breast milk (mother's own milk and donor milk) feeding whereas we did not because there was no human milk bank in our hospital at that time.
Our study shows that a multidisciplinary quality improvement initiative focused on breast milk promotion can significantly increase breast milk feeding in a Chinese NICU. In China, additional barriers are that parents are not permitted in the NICU because of concerns about cleanliness; and the cultural tradition of “maternal confinement,” which expects women to remain at home for at least 4 weeks after childbirth. 26 Consequently, parents can only see their infants in photos or videos, and only understand the condition of their infants through communication with NICU staff. In addition, donor mother's milk is not available in most NICUs, and Chinese parents have minimal knowledge of the benefits of mother's milk and breastfeeding. Indeed, promotions by formula companies have led many parents to believe that infant formula is superior to mother's milk. 27
The 4% reduction of surgical NEC in our study may also decrease intestinal failure, strictures, and malabsorption.28,29 We will follow up the subset of infants who underwent surgery for NEC in our future research.
There are several limitations to our study. First, this was a nonrandomized, pre–postinterventional cohort study conducted at a single center with the potential for bias from unmeasured confounding variables and that may have limited generalizability. However, randomized trials are not always feasible in interventions of this nature. Second, since the intervention in this study involved a bundle of practice changes, the contributions of each individual practice change cannot be clearly separated and it is difficult to assess which one was most effective.
Despite these limitations, the improvements we observed for this sample of very low-birth-weight infants in China are very encouraging. To our knowledge, this is the first quality improvement project to increase the prevalence of breastfeeding and promote mother's milk feeding in a Chinese NICU. The positive outcomes observed in this study provide important information for future comparative studies. Our findings may help to change the paradigm for nutrition practices and culture in Chinese NICUs from exclusive infant formula feeding to predominant breast milk feeding, which may have a tremendous impact on infant health and development in the future.
Conclusions
Our data suggest that implementing a bundle of practice changes is feasible and effective in improving breast milk consumption. In addition, the increase in mother's milk consumption is associated with a reduction in the severity of NEC in very low-birth-weight infants in a Chinese NICU. We will continue looking for opportunities to assess and enhance our current initiatives to further improve infant outcomes.
Footnotes
Acknowledgments
The authors would like to thank the neonatologists and nurses in the NICU for their support with the practice changes implemented for this study. These improvements would not have been possible without their efforts and cooperation. From the Maternal-Infant Care Research Centre (MiCare) at Mount Sinai Hospital, part of Sinai Health System, in Toronto, Ontario, the authors acknowledge Heather McDonald Kinkaid, PhD, for editorial support; and Philip Ye, MSc, for statistical support. This study was registered with the U.S. National Institutes of Health (![]() ): NCT02897388.
): NCT02897388.
Disclosure Statement
The authors have no conflicts or competing financial interests to declare.
Funding Information
This study was supported by the China-Canada Clinical Research Program, the Canadian Institutes of Health Research (CTP 87518), and Medela, Inc. (China) Research Funding. None of the funders was involved in designing the study; collecting, analyzing, or interpreting the data; writing the article; or deciding to submit this article for publication.