
Abstract
The leadership team at the Center for Maternal, Fetal and Neonatal Medicine, Saitama Medical Center, Saitama Medical University in Tokyo, Japan sought to improve our human milk (HM) and breastfeeding rates for vulnerable infants. This article describes the quality improvement (QI) initiative, which involved the implementation of the first three steps of the Spatz 10-step model for HM and breastfeeding in vulnerable infants. Our main objectives were to ensure that: (1) families were making informed feeding decisions about HM and breastfeeding as a medical intervention; (2) mothers were pumping early and often; (3) the staff implemented HM management; and (4) the proportion of infants who received HM at 1 month of life increased. Using a QI approach led by a nursing team, we were able to achieve all our goals. Our prenatal education was effective at having more families choose HM and breastfeeding versus formula. Our time to first milk expression improved as did the mothers' adherence with pumping early and often. We purchased physical resources to ensure that all milk was efficiently delivered to the infant in appropriate storage containers. At the initiation of this QI project, exclusive HM rates at discharge were only 15%. In only a 4 months time frame, the HM rate at discharge increased threefold to 47%. During the entire year, the portion of mothers selecting formula continued to decrease and HM rates continued to rise.
Introduction
The Baby-Friendly Hospital Initiative (BFHI) was established in 1991 as a worldwide program to incentivize maternity facilities to adhere to the Ten Steps to Successful Breastfeeding and comply with the International Code of Marketing of Breast Milk Substitutes. A report published by the World Health Organization (WHO) in 2017 has concerning findings about the state of the BFHI program worldwide. 1 Less than 10% of all births globally are occurring in BFHI facilities, and because hospitals have not been able to develop internal monitoring systems, the principles of BFHI are not maintained over time. 1
In response to the 2017 WHO report, the BFHI guidelines were updated in 2017 including principles that apply to preterm infants. 2 While the new guidelines are improved, little has been done to date to ensure implementation of the new guidelines worldwide. 3 The new guidelines do not address other vulnerable infants who may be separated from their mothers at birth. 2 Globally, only 41% of infants receive exclusive human milk (HM) for the first 6 months. 4
Breastfeeding in Japan
The awareness of breastfeeding in Japan has increased with more than 90% of mothers reporting the desire to breastfeed their infants during pregnancy. 5 In 2015, 96.5% of mothers engaged in at least partial (nonexclusive) breastfeeding during the first month and 89.8% in the third month. 5 The percentage of exclusive breastfeeding in Japan had increased to 51.3% in the first month of life and to 54.7% in the third month of life. 5
Japan was the first developed country to have the BFHI hospital accredited by the WHO and UNICEF in 1991, 6 and as of 2019, there were 47 BFHI facilities in Japan. 7 With BFHI accreditation, nursing teams tend to work together better and the overall facility's morale toward breastfeeding increases; however, this attitude is not maintained over time. 8 More effective staff education is needed with workshops recommended instead of traditional Japanese lectures. 8 In Japan, 83.3% of the medical facilities received formula company support. 9 Seven factors have been reported to negatively impact breastfeeding rates in Japan: (1) the modern trend of artificial nutrition and moms aspiring to feed their infants with formula; (2) the convenience of formula that allows mothers to share baby-feeding duties with other members of the family; (3) social changes such as women's emancipation and problems associated with going back to work; (4) nuclear family system becoming widely spread form of family, urbanization, and industrialization; (5) the rising number of hospital births and caregivers struggling to provide proper information and breastfeeding support; (6) a limited number of public initiatives protecting breastfeeding (National Nutrition Survey and Healthy and Happy Family 21 Initiative: both of which focus only on healthy infants); and (7) fear of environmental pollution that may impact HM quality. 10
There has not been any national initiative to improve HM and breastfeeding for vulnerable infants. Data from the United States show that there are persistent barriers to the provision of evidence-based breastfeeding care in the neonatal intensive care unit (NICU). 11 There is a clear need to increase capacity globally so that NICU infants have access to HM through the entire NICU stay and beyond. 12 In Japan, there exist very little data on HM and breastfeeding in vulnerable infants. Only one publication reported exclusive breastfeeding rates of 11.4% at 6 months postpartum for very low birth weight (VLBW) infants. 6
In 2018, the leadership team at the Center for Maternal Fetal and Neonatal Medicine (CMFNM), Saitama Medical Center (SMC), Saitama Medical University sought to improve our HM and breastfeeding rates for vulnerable infants. The CMFNM is an acute care department of SMC specializing in advanced perinatal care. The hospital's obstetric (OB) ward has 61 beds and there are 81 beds in the NICU. The center has 970 births annually, of which 56.7% are cesarean births. The NICU admits more than 800 infants. There are 60 midwives and 56 nurses working in OB wards and 145 nurses working in the NICU. Following a comprehensive literature review examining outcomes in the United States and Thailand, we selected the Spatz 10-step model for HM and breastfeeding for vulnerable infants13–17 to implement our quality improvement (QI) project. The QI project was reviewed and approved by the Ethics Committee of the Saitama Medical University/SMC.
The QI Project
The QI project commenced in March 2017. Key stakeholders and nursing staff led the project, and the decision was made to focus only on the first three steps of the model for this QI project (Table 1). To structure the work of the team, we decided to implement Plan-Do-Study-Act cycles (Table 2). To ensure that all families were making an informed feeding choice (Step 1), 13 we changed our education of families about HM and breastfeeding. Before the QI project, this information was not provided until the postpartum period. With the QI project, we began to provide this information with antenatal education at 18 weeks of pregnancy. Content of antenatal education for every family included benefits of HM and breastfeeding for the infant and for the mother herself, an explanation of how mother's lactation is initiated and milk supply is established. If an NICU admission was suspected, the family also received specific education about HM as a medical intervention.13,18
Ten Steps to Promote and Protect Human Milk and Breastfeeding in Vulnerable Infants
HM, human milk.
Plan-Do-Study-Act Cycles Implemented by the Saitama Medical Center Leadership Team
HM, human milk; PDSA, Plan-Do-Study-Act.
To ensure the availability of HM for initial feedings and for high-risk mothers to be able to breastfeed long-term, Step 2 (initiation and maintenance of milk supply) was implemented. 13 Our goal was for mothers to pump earlier (within 1 hour postdelivery) and more frequently (eight or more times per 24 hours) to: (1) more easily achieve the target milk volume of 500 mL/day at 1-month postpartum13,19 (before the start of our QI project, only 15% of our mothers were meeting this goal) and (2) increase the proportion of infants who received HM at 1 month of life.
At the initiation of the QI project, SMC owned 20 hospital-grade Symphony® pumps. However, they were not equipped with Initiation Technology™. In June 2017, all pumps were upgraded to the new technology that facilitates the removal of colostrum and enhances coming to volume.20,21 Milk production is enhanced with pumps that mimic infant suckling patterns in the first few days of life.20,21 Research also supports that mothers should pump early and often (ideally within the first hour and before 6 hours after birth).21–24 Frequent expression every 2 to 3 hours is critical.22–25 Simultaneous expression (double pumping) yields more milk in less time and results in higher prolactin concentrations. 26
In July 2017, to meet the goals of: first expression within 1 hour of birth, expressing frequently—8 or more times per 24 hours, and double pumping, all 261 staff nurses in the NICU and OB wards were provided in-depth education. The training was given in seven sessions over 3 days. All OB nurses were also educated on how to choose a proper size of the breast shield using PersonalFit® guide.
Two Symphony pumps with Initiation Technology were also placed in the operating room (OR) for mothers delivering by cesarean section. To facilitate early and frequent milk expression, key stakeholders made the decision to stock sterile breast pump kits on-site (this had not been a practice previously).
To address Step 3 of the model (HM management), we started the use of two different milk collection containers (disposable colostrum containers and sterile 80 mL containers) and disposable pump sets. Each mother was given a bottle size to match her milk production and keep her motivated. Mothers were provided instruction on labeling. Milk was stored by the OB nurse in the medical-grade refrigerator, for which a temperature uniformity of 5°C was constantly being monitored. Milk was then transported to either the NICU or the growing care unit. In addition to our refrigerators for milk, we invested in medical-grade freezers (−20°C).
Data Collection
In November 2017, QI data collection commenced. Maternal milk volume logs were first scanned and attached to the electronic record. In January 2018, an Excel datasheet was uploaded to three iPads® (Apple, Inc.) for all nurses on the OB unit to input the data. Between April and May 2018, we began to monitor the following QI indicators monthly: (1) time of first milk expression with goal being within 1 hour of birth; (2) mother expressing often with goal of 8 or more times in 24 hours; (3) percentage of mothers with milk coming to volume with goal being more than 70% of mothers; (4) identification of mothers with risk factors for delay in lactogenesis II/low milk supply; and (5) rates of any and exclusive HM/breastfeeding at 1 month postdelivery with goal of 50%.
In June 2018, two QI nurses were appointed to ensure that all data were being logged properly and were ready for monthly assessment. An Audit Nurse held monthly leadership meetings to review data set goals for the next month. The Audit Nurse also ensured that monthly results and audit feedback were shared with the entire OB team.
In May 2018, the official protocol for pumping early and often was implemented (See Fig. 1 for SMCs Pump Early, Pump Often Pathway.) All OB nurses received training on the protocol, including recently set QI goals. In the end of August 2018, we began to assess for and collect data on factors that may impact milk supply. We also improved our milk volume data collection sheet to 24 hours charting (versus days postdelivery) to prevent any ambiguity as to when events occurred in a patient's medical history. All OB and NICU staff received additional training regarding these changes. In October 2018, the senior author of this article provided an on-site visit to our hospital to audit the data and QI project.
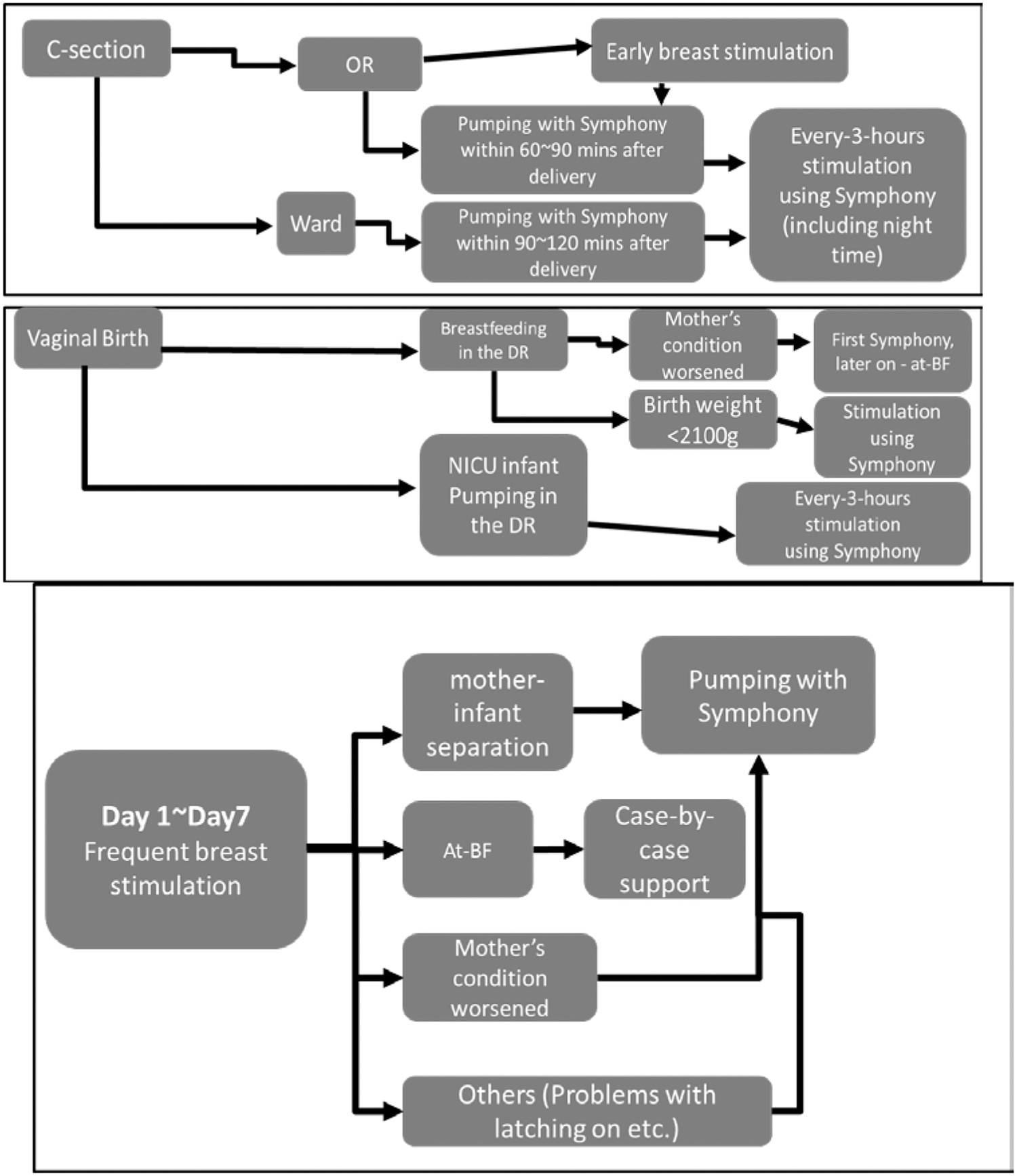
SMC protocol for pumping early and often. SMC, Saitama Medical Center.
Results of the QI Project
All mothers and their infants who were hospitalized at our center between April 1, 2018, and March 31, 2019, and had milk volume records were included (n = 696) (See Table 3 for detailed demographics). Only 5% of our mothers had no risk factors for delay onset of lactogenesis II/low milk supply. Results are described below according to monitored QI indicators.
Demographic Characteristics of Dyads Hospitalized from April 1, 2018, to March 31, 2019 (n = 696)
One mother may have one or more factors.
SD, standard deviation.
QI indicator no. 1: time to first stimulation/milk expression (minutes)
Hill and Aldag reported that milk volumes and frequency of expression on day 4 are significant predictors of milk supply at 6 weeks for pump-dependent mothers.27–29 Therefore, to achieve better volumes, we analyzed data during the first 96 hours postpartum and at 1 month postpartum. Education of nursing staff and development of precise protocol for pumping early resulted in significantly earlier and more frequent stimulation of the breast. After implementation of the first three steps of the Spatz 10-step model, our time to first pumping session improved significantly with 78% of mothers pumping within the first 2 hours (Table 1). Forty-four percent of mothers pumped within less than 1 hour postpartum and 34% of them pumped within 2 hours.
Only 3% of mothers pumped later than 6 hours. Further measures such as monthly audit introduced in June 2018 leveraged early pumping even more, increasing the percentage of mothers expressing with 1 hour at the time to more than 10% (Fig. 2A). Average, minimum, and maximum time to first stimulation (TtFS) was constant regardless of mode of delivery or term/preterm birth (vaginal TtFS = 116 minutes, cesarean TtFS = 104 minutes, preterm birth TtFS = 149 minutes, term birth TtFS = 97 minutes). Prior to the quality improvement initiative, the average TtFS was 815 minutes (13.5 hours)
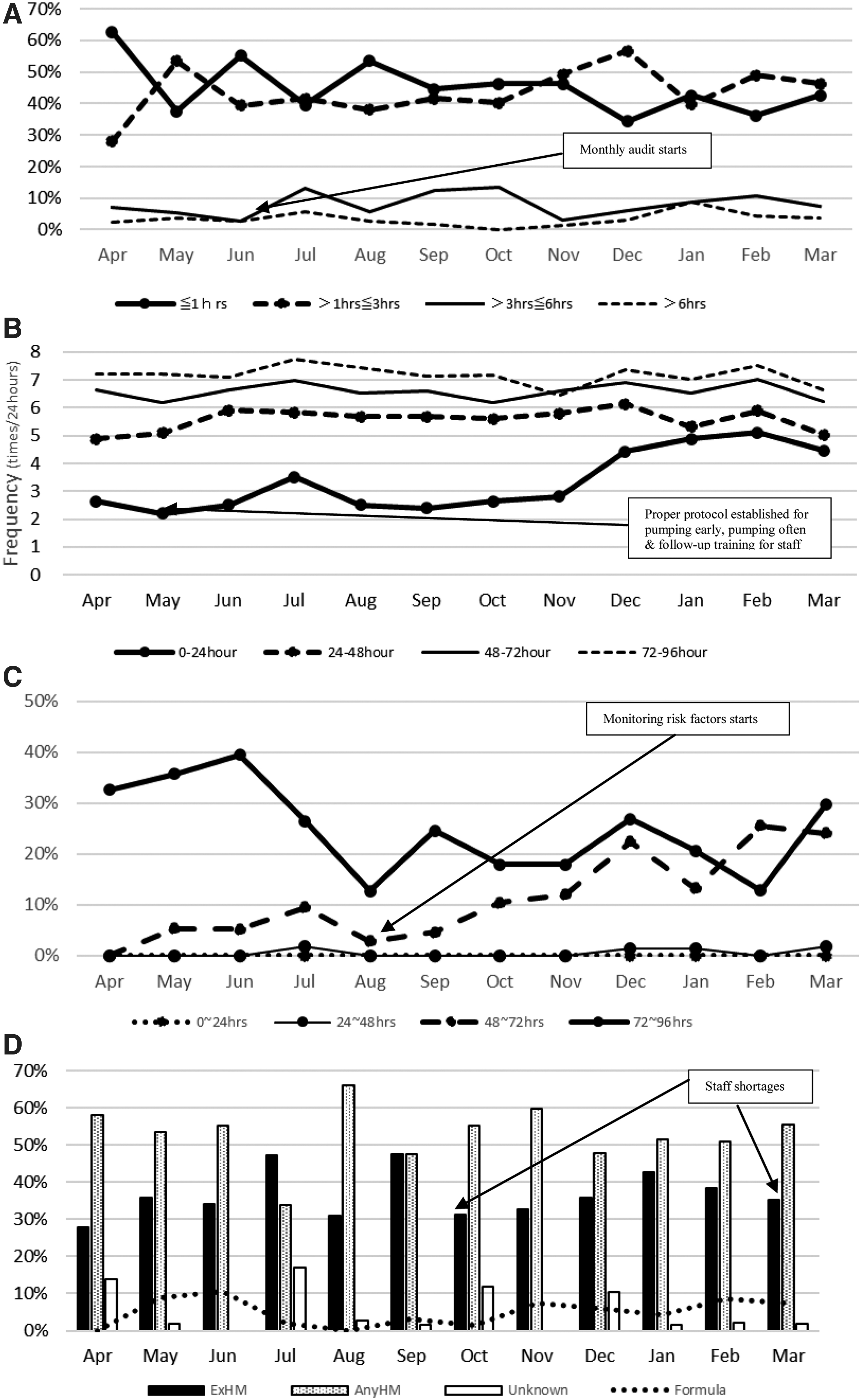
Before and after implementation of new measures—main outcomes by month (n = 696).
QI indicator no. 2: number of milk expressions per 24 hours
Measures introduced in May 2018, aimed at establishing precise protocol for pumping to achieve adequate volumes and enforcing double pumping to be done along with vital signs check, increased the number of milk expressions per day (Fig. 2B). Overall number of expressions (NoE) per 24 hours by 96 hours postpartum was consistent regardless of mode of delivery or term/preterm birth (vaginal NoE = 8, cesarean NoE = 7, preterm birth NoE = 7, term birth NoE = 7).
QI indicator no. 3: time to coming to volume (hours postpartum)
The combination of early and frequent pumping resulted in milk coming in faster and improved milk volumes by discharge (96 hours postdelivery). Only 33% of mothers experienced milk coming in by discharge at the beginning of the initiative. This number increased to 56% by March 2019 (Fig. 2C). For mothers with term infants, milk supply was measured by pre- and post-weights with milk volume ranging from 0.2 to 665 mL by 96 hours (median 69; mean 109). Unfortunately, due to the limited number of scales in the unit, not every breastfeeding session was recorded for term infants; therefore, the data represent a lower estimate of actual milk production.
For mothers of preterm infants, all milk expression sessions were logged by the nurse/mother and entered into the Excel database. Milk volume at 96 hours ranged from 0.3 to 718 mL (median 92; mean 245).
QI indicator no. 4: identification of risk factors
Mothers with risk factors for delayed onset of lactogenesis stage II are being identified, and care has been optimized to meet the needs of different high-risk groups. Outcomes resulting from this measure are still under investigation, but preliminary data show that secretory activation has been occurring 1 day faster (between 48 and 72 hours) for all populations since the measure was implemented (Fig. 2C).
QI indicator no. 5: any and exclusive HM at 1 month postdelivery
Despite month-by-month changes over the course of 12 months, we saw a significant increase in infants receiving HM at 1 month of life. At the initiation of this QI project, exclusive HM rates at 1 month of life were only 15%. In 4 months, these rates increased over threefold to 47%. During the entire year, the portion of mothers selecting formula continued to decrease and HM rates continued to rise, with any HM rates reaching more than 50% in most of the months (Fig. 2).
Discussion
The Spatz 10-step model for HM and breastfeeding was effectively applied to the Japanese NICU context. This QI project resulted in significant improvement in the percentage of mothers expressing their milk within 1 hour of delivery, vulnerable infants receiving more of their mother's own milk by 28 days of life, and a decrease in the percentage of mothers who chose to feed their infants only with formula. This QI project represents the first published report to demonstrate the effectiveness of systematic implementation of the Spatz methodology in level III perinatal care center in Japan.
Despite the identification of mothers with delayed secretory activation, decreases in TtFS, and more frequent and effective expression, there was only a small increase in the number of mothers who achieved coming to volume (defined as three consecutive days of >500 mL total volume) by day 14. There are a number of factors underlying this result including the quality of first stimulus, the impact of first hour postpartum in high-risk populations, the negative impact of Japanese birth traditions, staff shortages at various points throughout the year, environmental challenges of test weights, deeply rooted hand-expression culture, and follow-up and unnecessary supplementation after discharge.
The quality of first stimulus
Although many of our mothers received their first stimulation in the OR, the recommended pumping time of 15 minutes with the initiation pattern was not enforced properly due to OR preparation time (turnover) between one mother leaving and another entering. As a countermeasure, we recently installed battery packs for the two pumps in the OR to stimulate the breast while on the move to the OB ward.
The impact of first hour postpartum in high-risk populations
Parker et al. demonstrated that initiation of breast stimulation 1–3 hours after delivery increases the duration of lactation and decreases time to lactogenesis stage II in mothers of VLBW infants. To combat the impact of multiple risk factors that one mother may have and to achieve higher milk volumes on day 4, focusing on pumping within the first hour postpartum instills a sense of urgency among staff and families about establishing milk supply. Further investigation is warranted.
The negative impact of Japanese birth traditions
In Japan, often when a mother delivers her child, the time of her recovery is marked by an event called tokoage sanshuukan (lifting of the bedding after 3 weeks postpartum). Historically, until the tokoage ended, the mother was given 3–4 weeks of time where she was expected to “sleep, eat, and feed her infant” to gain strength and vitality, before the demanding period of parenting started.
However, perception of this tradition has changed in recent years. Most mothers nowadays interpret this period as time “to sleep, eat, and relax.” This interpretation of tokoage often led mothers to misunderstand nurses' efforts to support frequent stimulation of the breast immediately postpartum, and nurse to give in further care. As a result, frequent stimulation within the first 48 hours was lower than expected. To combat this, we have begun to align the time of pumping/breastfeeding to the time of vital signs check. However, we also acknowledge that increasing frequency of prenatal education and improving communication skills especially of younger staff are essential to better encourage the mother in her early postpartum efforts to breastfeed.
Staff shortages
When examining the full year of data, there are certain months where the exclusive HM rates were lower. This was particularly vivid during the months of October 2018 and March 2019, where we experienced a shortage of staff due to an increased number of deliveries. We recognize that the nurse has many patient care responsibilities. However, support of HM use and long-term breastfeeding in our center is a top priority. As we move forward with implementation of subsequent steps of the Spatz 10-step model, we acknowledge that better administrative and human resources measures will be needed to resolve those challenges.
Environmental challenges of test weights
Examining the results of milk volumes in term and preterm mothers, lower volumes in term mothers can be noted. This disparity in results, despite fewer risk factors in that population, may be related to the limited availability of Tanita™ scales on site. As a result, not every single breastfeeding session was captured for mothers of term infants. Therefore, these data might represent a lower estimate of actual milk production. As we are planning modernization of the ward, our goal is that the size and layout of a room will have more space for the necessary equipment and provide more privacy for families. This will improve our ability to provide evidence-based lactation care and breastfeeding support to mothers.
Deeply rooted hand-expression culture
Hand expression and hand massage are deeply rooted in Japanese midwifery culture. Multiple methods have been cultivated over the years, and professional training sessions are part of our culture. Japanese mothers may consider hands-only methods when trying to solve their breastfeeding problems. Fukuda et al. stated that the purpose of a midwife giving hand-care is not only to support a mother's lactation but also to “give (her) mental support and professional advice while performing the care.” 30 By doing so, the midwife supposedly helps the mother feel more confident in her childcare. 30 Therefore, many midwives and nurses may be resistant to implementing milk expression with a hospital-grade pump as a form of lactation care. This challenge was observed at SMC in the beginning of the initiative.
Follow-up and unnecessary supplementation after discharge
The Japan Ministry of Health, Labor and Welfare survey noted that 77.8% of mothers reported trouble with breastfeeding. 5 Top-box scores of the survey included answers such as: “I do not know if I am making enough milk” (40.7%), “I do not make enough milk” (20.4%), and “Breastfeeding is tough and killing me” (20%). 5 In Japan, first-time mothers experienced the following eight concerns in the first 4 months: (1) breast refusal, (2) problems positioning and with hand-expression, (3) frequent feeding or sudden change in feeding behavior, (4) not knowing how to evaluate whether infant has breastfed sufficiently, (5) problems with coming to volume, (6) sore nipples, (7) changes in lifestyle due to breastfeeding, and (8) insufficient support or discouragement from closest community. 31
Hashizume et al. also reported that in Japan some mothers go to breastfeeding rooms in big supermarkets and use scales placed there to weigh their infants. 31 But other mothers who are not confident in their milk supply simply just start formula supplementation out of fear. 31 Our staff also heard similar stories from our mothers after discharge. Thus, we acknowledge that we have a great deal of work to do to improve long-term breastfeeding rates in Japan. This QI project implementing the first three steps of the Spatz 10-step model to promote and protect HM and breastfeeding in vulnerable infants was effective in improving the time to first milk expression, the number of milk expressions per day, and the overall exposure to HM both during the first four days and at 1 month postdischarge.
It is a common perception in Japan that newborns hospitalized in the NICU, including preterm infants under a certain gestational age, cannot breastfeed directly. Our next goal is to implement further the Spatz 10 steps to address the challenges of helping mothers and their preterm infants to establish direct breastfeeding earlier, as well as to improve the postdischarge support of NICU infants to ensure optimal nutrition and growth for these infants who may benefit most from HM.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.