
Abstract
A central goal of The Academy of Breastfeeding Medicine is the development of clinical protocols, free from commercial interest or influence, for managing common medical problems that may impact breastfeeding success. These protocols serve only as guidelines for the care of breastfeeding mothers and infants and do not delineate an exclusive course of treatment or serve as standards of medical care. Variations in treatment may be appropriate according to the needs of an individual patient.
Introduction
Breastfeeding women may develop breast masses or complaints at any point during lactation. Symptoms may be related to lactation, such as a lactating adenoma, or may be due to a condition that coincidentally has manifested during the postpartum period. Understanding the importance of appropriate workup and imaging, as well as indications for referral to breast surgery, is essential to establishing a diagnosis and avoiding delay in care.
Breast symptoms require evaluation by physicians and/or lactation consultants and may also require diagnostic breast imaging and/or biopsy. The American College of Radiology (ACR) released new guidelines in 2018 regarding breast imaging of pregnant and lactating women. 1 These guidelines state that all breast imaging studies and biopsies are safe for women to undergo while breastfeeding, and also provide recommendations for maximizing examination sensitivity and minimizing biopsy-related complications in this patient population.
When approaching a breastfeeding woman with breast symptomatology, it is helpful for providers to frame the workup based on the presence or absence of a palpable mass on examination (Fig 1). Some conditions always present as a mass, whereas others rarely have a palpable finding. However, several conditions have variable presentations and may manifest as a mass and/or another sign/symptom such as nipple discharge (Fig. 2).

Suggested approach for the evaluation of breast complaints in lactating women.
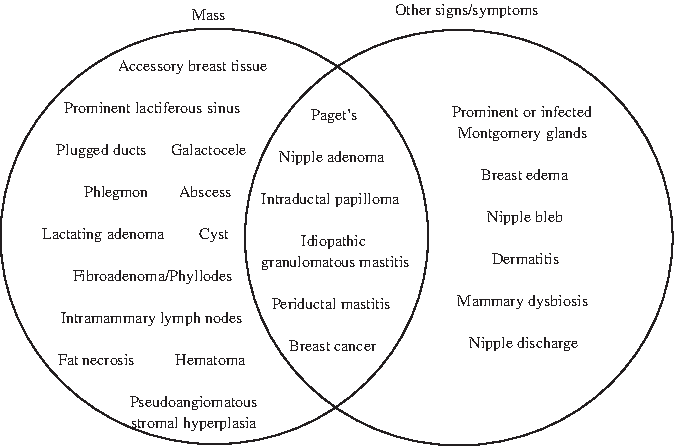
Presenting signs/symptoms of common breast conditions that may affect lactating women.
Quality of evidence is based on the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence 2 (levels I–IV) and is noted in parentheses.
Breast Masses
The majority of persistent breast masses warrant diagnostic imaging. Although several breast masses may occur in the setting of lactation and are benign, imaging generally is required to distinguish these from non-lactation-specific breast masses. Both benign and malignant masses unrelated to lactation also may present during the postpartum period. Thus, clinicians should perform axillary and supraclavicular lymph node examinations on all women presenting with a breast mass. Specific masses and/or associated symptomatology may warrant referral to a breast surgeon for biopsy or intervention. The most common breast masses diagnosed during lactation are highlighted in Table 1.
Most Common Breast Masses Diagnosed During Lactation
Lactation-specific masses
When history and examination by an experienced breastfeeding medicine physician are consistent with a lactation-related condition that the provider is comfortable managing, imaging can be deferred. If the condition presents atypically or does not resolve with standard treatment, diagnostic imaging is indicated. Examples of such conditions include the following:
Lactation-specific masses that require imaging for diagnosis include the following:
Non-lactation-specific masses
Benign masses that are not specific to lactation include the following:
Non-Mass Breast Complaints
Breastfeeding women seeking medical evaluation of breast symptoms who do not have a palpable mass on examination may present with a variety of conditions, some of which require diagnostic imaging. These conditions can be categorized into skin conditions, nipple discharge, and breast pain.
Skin conditions
A number of skin conditions can be diagnosed by history and physical examination and thus do not require diagnostic imaging. Benign lesions that are interfering with breastfeeding, such as a skin tag on the nipple–areolar complex (NAC), warrant referral to a breast surgeon. Lesions that raise suspicion for Paget's disease, inflammatory breast cancer, or other malignancy require both diagnostic imaging and referral to a breast surgeon.
Examples of skin conditions for which breastfeeding women may seek care include the following:
Nipple discharge
Although breastfeeding women experience physiologic milk expression from their nipple orifices, they also may note other colors of
Bloody discharge may be due to several conditions including the following:
In addition, bloody nipple discharge may occur in up to 24% of women at any point during lactation
30
(IV). This phenomenon is related to proliferative epithelial changes and increased vascularity in the breast, and is usually self-limited. Persistent bloody nipple discharge presenting after the immediate postpartum period should be evaluated with diagnostic imaging. Although pink- or red-tinged expressed milk may raise concern for bloody nipple discharge, this phenomenon may be due to colonization with the pigment-producing bacterium Serratia marcescens and should resolve with antibiotic therapy
32
(IV).
Breast pain
The workup and treatment for breast pain in lactating women with no mass or other physical examination findings to suggest a diagnosis have been previously described and are beyond the scope of this protocol 33 (IV). Women with pain that does not resolve with appropriate intervention should undergo diagnostic imaging.
Diagnostic Breast Imaging and Breast Biopsy During Lactation
Few international organizations report specific recommendations regarding breast imaging during lactation. The ACR recommends that diagnostic breast imaging in lactating women follow the same guidelines as for nonlactating women 1 (IV), with the exception of ductography that is not recommended in lactation 34 (IV). As shown in Figure 1, we recommend diagnostic breast imaging of almost all breast masses and for several specific non-mass breast complaints.
For diagnostic imaging in a breastfeeding woman, ultrasonography is recommended as the initial imaging modality. If ultrasonography shows suspicious findings or is discordant with clinical examination, additional imaging with mammography or digital breast tomosynthesis (DBT, or “3D mammography”) may be indicated. 1 This is related to the fact that mammogram or DBT can visualize architectural distortion and/or calcifications not seen on ultrasonography, as well as delineate extent of disease in the setting of malignancy 35 (IV).
Core needle biopsy rather than fine needle aspiration should be performed after a full diagnostic imaging workup has been completed. Core needle biopsy generally can be performed under ultrasound guidance for a palpable mass. However, if the mass does not have an ultrasound correlate, a woman may be recommended to undergo a stereotactic core needle biopsy with mammographic guidance or a magnetic resonance imaging (MRI)-guided biopsy. Although there is a small but rare risk of milk fistula, this risk should not preclude biopsy of any suspicious lesion 36 (IV). Lactating women should also be counseled about a theoretical small increased risk of postprocedural bleeding secondary to hypervascularity 37 (IV). We do not recommend discontinuation of breastfeeding before biopsy in an effort to minimize these risks. In fact, the inflammation related to abrupt weaning 38 (IV) could increase the risk of fistula formation, and lack of alternative drainage routes (e.g., through the nipple) could promote fistula formation through the biopsy tract.
If a woman is diagnosed with a breast malignancy on initial imaging and biopsy, she may be recommended to undergo additional biopsy of suspicious lymph nodes in her regional nodal basins (axillary, internal mammary, and supra- and infraclavicular). Breast radiology and breast surgical oncology also may recommend breast MRI to rule out multifocal or multicentric tumors, contralateral disease, or pectoralis and/or skin involvement. Although MRI is less sensitive in the setting of lactation due to increased parenchymal density and vascularity, it nevertheless is not contraindicated and may provide diagnostic and treatment planning benefit. 1
Recommendations for Future Research
Although there is strong evidence for the safety and feasibility of nearly all breast imaging studies in lactating women, the data on the relative sensitivities of each modality are limited. There is a growing body of literature that describes normal imaging findings in the lactating breast compared with the nonlactating breast, but there is a paucity of data on the radiologic differences between lactating women with specific pathologies and lactating women without breast lesions. Another area for further study is the management of breast masses and breast complaints of transgender individuals who are chestfeeding. In the absence of specific data, it is reasonable to follow the algorithms described herein for lactating women.
Footnotes
ABM protocols expire 5 years from the date of publication.
Content of this protocol is up-to-date at the time of publication. Evidence-based revisions are made within 5 years or sooner if there are significant changes in the evidence.