
Abstract
Abstract
A central goal of the Academy of Breastfeeding Medicine is the development of clinical protocols for managing common medical problems that may impact breastfeeding success. These protocols serve only as guidelines for the care of breastfeeding mothers and infants and do not delineate an exclusive course of treatment or serve as standards of medical care. Variations in treatment may be appropriate according to the needs of an individual patient.
Background
When a cleft lip (CL) occurs, the lip is not contiguous, and when a cleft palate (CP) occurs, there is communication between the oral and nasal cavities (see Fig. 1 for a completely formed lip and palate). 1 CL may involve the lip only; lip and alveolus; or lip, alveolus, and a notch in the hard palate. The notch in the hard palate may extend all the way to the incisive foramen (Fig. 2). 2 Similarly, a CP may involve only the uvula (e.g., bifid uvula), the uvula and soft palate, or extend through both the hard and soft palates (Fig. 3). 1 In a complete cleft of hard and soft palates, there is no bone or muscle separating the oral and nasal cavities. A CP may be submucosal and not immediately detected intraorally if there are subtle or no corresponding clinical signs or symptoms. 1 Therefore, it is essential that health professionals check for palatal clefting (both overt and submucosal) on initial presentation, by visually inspecting and palpating the palate. This should be done using a tongue depressor and flashlight to allow for inspection of the entire palate, including the uvula. An oral examination is of relevance if an infant is presenting with feeding difficulties or not gaining weight.
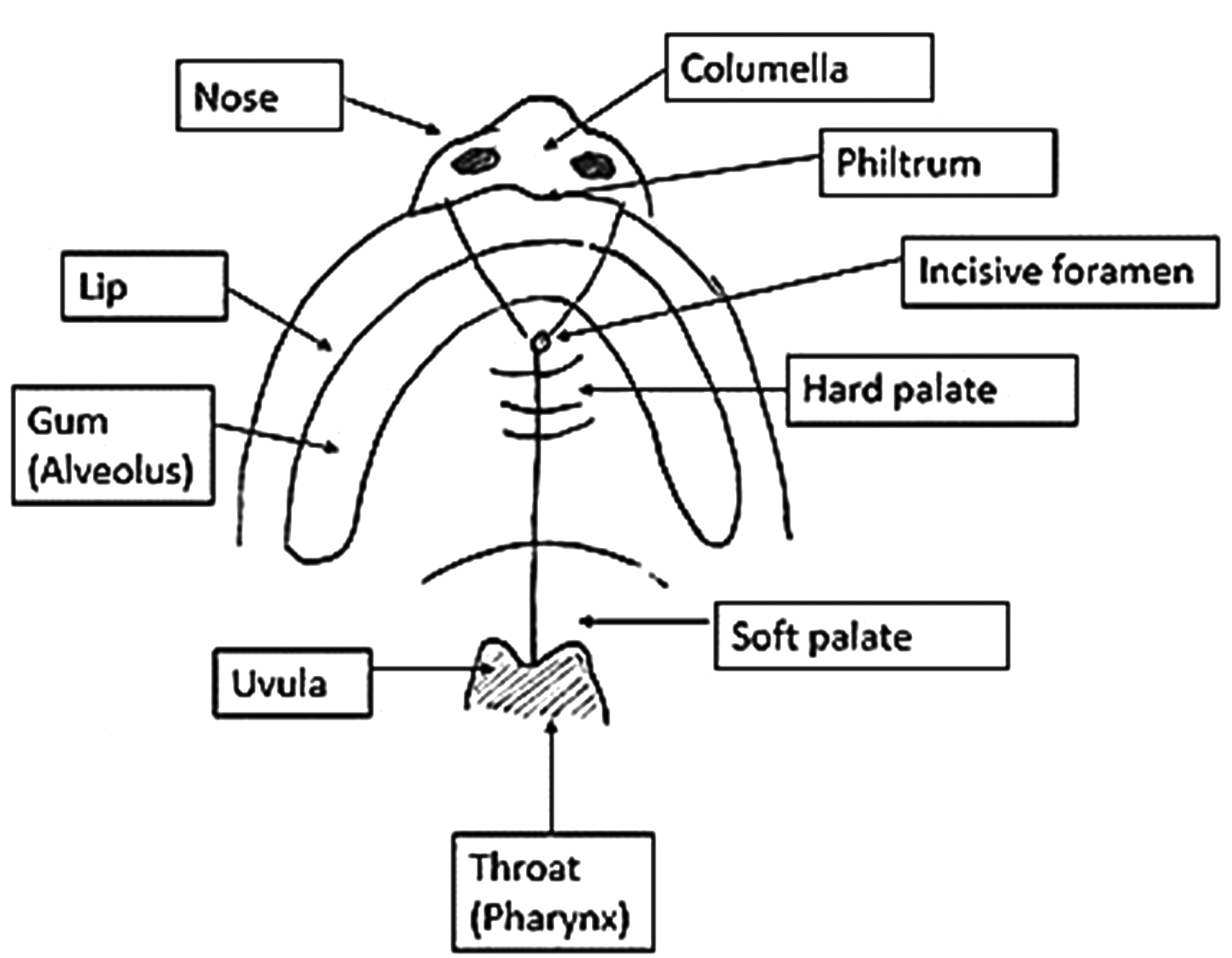
Completely formed lip and palate (no cleft). This illustration shows an intact inferior view of the nose, upper lip, and hard and soft palates. Note the y-shaped suture lines where the lip, alveolus, and palate fused during gestation. During gestation, the suture lines fuse from the incisive foramen toward the philtrum area of the lip (just below the nose) and from the incisive foramen toward the uvula. A cleft of the lip and/or palate occurs when this fusion is incomplete or does not occur. (Illustration courtesy of Aiden Farrow, copyright 2018).

Clefts of the lip. This figure illustrates
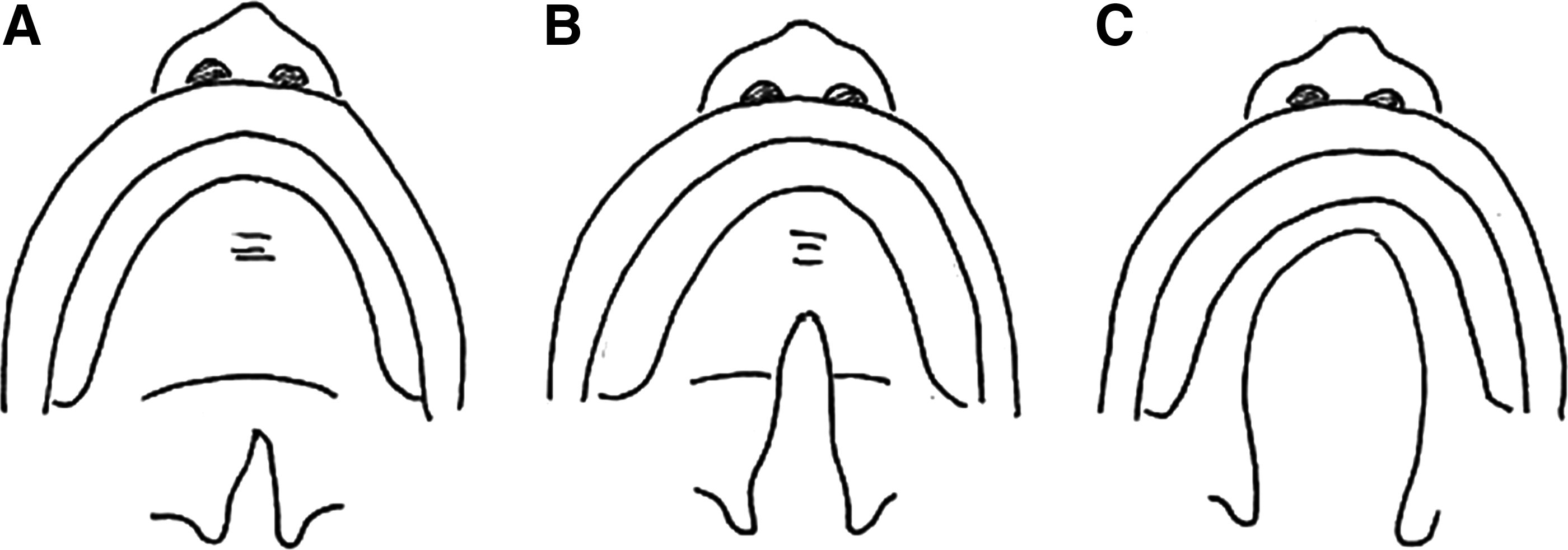
Clefts of the palate. This figure illustrates three presentations of a CP.
Surgical cleft repairs can involve multiple procedures, depending on the nature and extension of the cleft (i.e., unilateral CL versus bilateral cleft lip and palate [CLP]). The primary repair(s) are generally completed within 18 months of life, with the lip being repaired before the palate at 3–9 months of age.3,4
Incidence
The worldwide prevalence of CL and/or CP (CL/P) ranges from 0.8 to 2.7 cases per 1,000 live births.5,6 There are differences in incidence rates across racial groups and geographical locations, with the lowest reported incidence among populations of African (∼0.5/1,000)6–8 and European descent (∼1/1,000 births) 5 and higher incidence among Native American (∼3.5/1,000) and Asian (∼1.7/1,000) populations.6,7
Although reports vary considerably, it is estimated that out of the total number of infants with CL/P, ∼50% have combined cleft lip and palate (CLP) (Fig. 4), 30% have isolated CP, and 20% have isolated CL; CL extending to include the alveolus occurs in ∼5% of cases. 9 Clefts are more commonly unilateral, but can also occur bilaterally. 10 Approximately 30% of cases are part of identified syndromes or multiple congenital anomaly disorders, such as 22q11 deletion syndrome, Van der Woude syndrome, or Pierre Robin sequence.6,7 The remaining 70% are nonsyndromic and occur in isolation of identified syndromes.6,7

Unilateral and bilateral CLP. This illustration shows
Breastfeeding and CL/P
In these guidelines, breastfeeding refers to direct placement of the infant to the breast for feeding, and breast milk feeding refers to delivery of breast milk to the infant through bottle, cup, spoon, or any other means except the breast. Babies use suction to breastfeed successfully. The ability to generate suction is necessary for attachment to the breast, maintenance of a stable feeding position, and, together with the let-down reflex, milk extraction. Normally, when babies are feeding, their lips flange firmly against the areola, sealing the oral cavity anteriorly. The soft palate rises up to contact the pharyngeal walls and seal the oral cavity posteriorly. As the tongue and jaw drop during sucking, the oral cavity increases in size, and negative pressure is generated, drawing milk from the breast. 11 Suction and wave-like movement of the tongue help milk transfer and delivery during breastfeeding.11–13
There is a relationship between the size and type of cleft, maturity of the infant, and amount of oral pressure generated during feeding. 13 Younger infants with larger clefts can be expected to generate less oral pressure. Most infants with isolated CL are often able to successfully breastfeed because they can generate suction and negative pressure. This is achieved when the nipple is compressed between the tongue and maxilla leading to milk being expelled into the oral cavity. 14 Some infants with small soft palate clefts can generate adequate negative pressure, but others with larger soft and/or hard palate clefts may not.15,16 In addition, term and preterm newborns may generate lower suction pressure than older infants.17,18 In general, infants with CP or CLP have difficulty creating suction and negative pressure because the oral cavity cannot be adequately separated from the nasal cavity during feeding.19,20 For these infants, negative consequences may include fatigue during breastfeeding, prolonged feeding times, nasal regurgitation, reflux, insufficient milk transfer, and impaired growth and nutrition.21,22
The literature describing breastfeeding outcomes in infants with CL/P is limited. Available evidence is anecdotal and sometimes contradictory, making it challenging to develop appropriate recommendations. 23 Recommendations are outlined below, and answers to frequently asked questions are detailed in Appendix A1.
Recommendations
Quality of evidence for each recommendation is noted in parentheses. Levels of evidence are listed as 1-5, with level 1 being the highest, as defined in the Oxford Centre for Evidence-Based Medicine 2011 Levels of Evidence. 24
Recommendations for clinical practice
Based on the reviewed evidence, the following recommendations are made:
Encourage parents to breastfeed and provide breast milk when possible Parents should be educated about the protective benefits of breast milk. Evidence suggests that breastfeeding protects against acute otitis media, which is highly prevalent in this population25–27
(level 2). Breast milk feeding has also been shown to have long-term health and developmental benefits above that of artificial breast milk substitutes for both infants and their breastfeeding parents.28–30
Breast milk feeding (through cup, spoon, bottle, syringe, etc.) should be promoted in preference to artificial breast milk substitutes if breastfeeding is not possible.
21
Bottles that facilitate milk flow may be necessary for short- or long-term use if compensatory techniques are not sufficient for growth. These bottles may have specially designed teats, be squeezable, or use one-way valves to control milk flow. There are various brands available. Parents should be provided with anticipatory guidance regarding effective techniques for milk expression, alongside the quantity of milk needed and storage methods.31,32 Parents of infants with CL/P should be advised of expected feeding outcomes based on the infant's cleft type and what has been documented in the available literature.31,33 This guidance should be provided during the antenatal and postnatal periods.
34
Consistent and expert counseling should be provided by health professionals with clinical expertise in feeding infants with CL/P31,33–35 (levels 4 and 5). There is moderate evidence to suggest that infants with CL may be able to generate sufficient suction
19
(level 4), and descriptive reports suggest that these infants are often able to breastfeed successfully36–38
(levels 4–5). There is moderate evidence that infants with CP or CLP have difficulty generating sufficient intraoral suction
15
(level 2) and may have inefficient sucking patterns
16
(level 3) compared with noncleft infants. Overall, infants with CP or CLP are observed to have lower success rates for breastfeeding than infants with CL or no cleft. This applies even after surgical repair
39
(level 3). Nonetheless, breastfeeding attempts may still be beneficial for maintaining milk supply if a mother is also expressing breast milk.15,16 Breastfeeding may also provide comfort and bonding opportunities for infants and mothers, while allowing infants to experience feeding from the breast.40,41 Evidence suggests that breastfeeding can commence/recommence immediately after CL repair3,4,42 (levels 2–3). Breastfeeding can commence/recommence 1 day after CP repair without complication to the wound.
4
In a survey of surgeons regarding postoperative care after palatoplasty, two-thirds of surgeons allowed mothers to breastfeed immediately after surgery
43
(level 4). However, as cleft repairs do not occur immediately after birth, infants may require additional support to be taught how to breastfeed with their newly repaired clefts. Therefore, parents should be counseled that alternative means of feeding may still be required postsurgically to meet growth and nutritional goals.
35
Personal and social supports are also important during this time.31,32 Provide timely assessment and support Parental education and supports should be provided in a timely manner. Surveys have indicated that parents of a child with CL, CLP, or CP desire more instruction on feeding challenges as early as possible; this commences in the antenatal period and should be ongoing
32
(level 4). Involving partners and other caregivers in the feeding process is also recommended.
31
Several studies have suggested that there are benefits from having access to a health professional who specializes in CL/P and breastfeeding, such as a clinical nurse specialist or lactation specialist (including International Board Certified Lactation Consultants [IBCLC]), during the newborn and later periods. Specialists can determine the feasibility of breastfeeding and advise about managing milk supply and expressing for supplemental feeds. Early advice is key, as mothers may be encouraged to initiate milk expression within the first few hours of birth.
44
Specialists can also assist with suitable supportive techniques (outlined in the “Implement Strategies to Support Breastfeeding” section).31,33,45 It is important to consider the size and location of the infant's cleft, breast anatomy, the parent's wishes, and previous experience with breastfeeding. Families may benefit from peer support around breastfeeding or breast milk feeding found through local support groups and associations, such as Wide Smiles,
46
in addition to routine referral to breastfeeding support groups. An infant's hydration and weight gain should be monitored while a feeding method is being established. If breast milk feeding alone is inadequate, supplemental feeding should be implemented or increased if indicated (see “ABM clinical protocol #3: Hospital guidelines for the use of supplementary feedings in the healthy term breastfed neonate, revised 2017”
47
). Infants with CL/P may require supplemental feeds for adequate growth and nutrition20,38 (level 4). Evidence from a single study demonstrated that additional maternal support by a clinical nurse specialist can both improve weight gain and facilitate early referral to appropriate services
48
(level 4). When CL/P occurs as part of a syndrome/sequence, the potential for breastfeeding should be assessed on a case-by-case basis, taking into account any additional features of the syndrome that may impact breastfeeding success. If a palatal prosthesis is used for orthopedic alignment before surgery, caution should be taken in advising parents to use such a device to facilitate breastfeeding. Rather, parents should be informed that the device likely will not significantly increase breastfeeding efficiency or effectiveness (levels 1–4).49,50 Implement strategies to support breastfeeding Modified breastfeeding positions may increase the efficiency and effectiveness of breastfeeding. There are many recommendations about physical positioning of the infant to support breastfeeding. However, they are supported by weak evidence (clinical experience or expert opinion). Specific recommendations that require future evaluation include: For infants with CL. The infant should be held so that the CL is oriented toward the top of the breast50,51 (level 4). For example, an infant with a right CL may feed more efficiently in a cross-cradle position at the right breast and a “football/twin style” position (i.e., the body of the infant positioned alongside the mother, rather than across the mother's lap, with the infant's shoulders higher than his or her body) at the left breast (Fig. 5). For bilateral CL, a “face on” straddle position may be more effective than other breastfeeding positions
51
(level 4). For infants with CP or CLP. In addition to modifying positioning of the infant, parents can implement the following strategies. These strategies are supported by similarly weak evidence (clinical experience or expert opinion): For infants with CL. For infants with CP or CLP. For infants with CP, it may be useful to position the breast toward the “greater segment” of the palate. That is, the side of the palate that has the most intact bone. This may facilitate better generation of negative pressure and thus milk extraction, while preventing the nipple from being pushed into the cleft site
57
(level 4). If the cleft is large, some experts suggest that the breast be positioned downward to stop the nipple being pushed into the cleft
51
(level 4). Some experts suggest supporting the infant's chin to stabilize the jaw during sucking
52
and/or supporting the breast so that it remains in the infant's mouth (Fig. 6)56,58 (level 4). Mothers may need to manually express breast milk into the baby's mouth to compensate for absent suction and compression and to stimulate the let-down reflex
15
(level 4).

“Football Hold” feeding position. This illustration shows the “Football Hold” breastfeeding position that may be used for infants with CL, CP, or CLP. (Illustration courtesy of Children's Minnesota Hospital).

Supporting the infant's chin during breastfeeding. This illustration demonstrates how a mother may use her free hand to support an infant's chin and/or breast to maintain a semi-upright position. This can help to stabilize the jaw during breastfeeding and ensure that the breast remains in the infant's mouth. (Illustration courtesy of Children's Minnesota Hospital).
Recommendations for future research
The most pressing issue for health care professionals working with parents who wish to breastfeed their infants with CL/P is the lack of evidence on which to base clinical recommendations. Well-designed data-driven investigations are imperative to generate high-level evidence and inform future guidelines. Future research is needed, covering the areas of feeding rates, management strategies, economic outcomes for breastfeeding infants with clefts, and health and developmental outcomes for infants with CL/P (e.g., communication, parent satisfaction, and rates of upper respiratory tract infections). Furthermore, investigators must clearly describe their sample of infants and intervention techniques so that the research outcomes can be generalized. Differentiation between cleft types and sizes is particularly important in this cohort.
Footnotes
Acknowledgments
We thank international reviewers, Dr. Sandra Massry, Dr. Makiko Ohyama, and Aiden Farrow, BSc, Cert PPH, IBCLC, for their valuable input toward the revision of this protocol. We extend our gratitude to Aiden Farrow and Children's Minnesota Hospital for permission to use their illustrations.