
Abstract
A central goal of the Academy of Breastfeeding Medicine is the development of clinical protocols for managing common medical problems that may impact breastfeeding success. These protocols serve only as guidelines for the care of breastfeeding mothers and infants and do not delineate an exclusive course of treatment or serve as standards of medical care. Variations in treatment may be appropriate according to the needs of an individual patient.
Purpose
Bedsharing promotes breastfeeding initiation, 1 duration,2–7 and exclusivity.7,8 Medical and public health organizations in some countries recommend against bedsharing, citing concerns over increased risk of sleep-related infant death.9,10 However, bedsharing may only be a risk in hazardous circumstances as demonstrated by epidemiological study (Table 1). 11 We aim to clarify the currently available evidence regarding the benefits and risks of bedsharing, and offer evidence-based recommendations that promote infant and maternal health through increased breastfeeding duration. 12 The recommendations in this protocol apply to mother–infant dyads who have initiated breastfeeding and are in home settings, and are not intended for use in hospitals or birth centers.
Hazardous Risk Factors or Circumstances During Bedsharing
Amounts of alcohol causing impairment are discussed in the text.
SIDS, sudden infant death syndrome.
Summary and Recommendations
Summary
Levels of evidence (1–5) from the Oxford Centre for Evidence Based Medicine 13 are listed in parentheses, and are based on the citations as described below in the supporting material. See the supporting material for the ways in which we define “bedsharing,” “SIDS,” and “separate sleep” for purposes of this protocol. “Breastsleeping” is defined there as well.
Overall, the research conducted to date on bedsharing and breastfeeding indicates that nighttime proximity facilitates breastfeeding duration and exclusivity (levels 2–3).2,4,14 Discussions about safe bedsharing should be incorporated into guidelines for pregnancy and postnatal care.15–19 Existing evidence does not support the conclusion that bedsharing among breastfeeding infants (i.e., breastsleeping) causes sudden infant death syndrome (SIDS) in the absence of known hazards (level 3) (see Table 1). 11 Larger studies with appropriate controls are needed to understand the relationship between bedsharing and infant deaths in the absence of known hazards at different ages. Not all hazards are individually modifiable after birth (e.g., prematurity). Accidental suffocation death is extremely rare among bedsharing breastfeeding infants in the absence of hazardous circumstances (levels 2–3), 20 and must be weighed against the consequences of separate sleep. There are consequences to breastfeeding with separate sleep (even with room-sharing) that include the risk of early weaning, the risk of compromise to milk supply from less frequent nighttime breastfeeding, and unintentional bedsharing (levels 1–3).5,21,22 Recommendations concerning bedsharing must take into account the mother's knowledge, beliefs, and preferences and acknowledge the known benefits as well as the risks (level 5).23,24
Recommendations
All families should be counseled about safe sleep
Table 2 summarizes safe sleep advice in order of importance based on the strength of the evidence. In addition, we recommend the following:
Discussion with open-ended questions from health care providers concerning bedsharing safety should happen with all parents, as bedsharing is likely to happen whether intended or not (level 4).
25
These discussions should take place early in the perinatal course and continuously throughout infancy, and include as many caregivers as possible. Open-ended questions that have been found to be successful in opening conversations include: “What are your plans for where your baby will sleep?” “What does that sleep area look like?” “Does your baby ever end up in bed with you?” Screen families at increased risk of infant death with bedsharing: infants who were born preterm (level 2)
26
(level 3),
27
exposed to tobacco antenatally (level 1)
28
(level 4)
29
(level 5),
30
live with smokers (level 1)
28
(level 3)
11
(level 4),31,32 and those who live with people who consume alcohol (level 3)
11
or drugs and, therefore, might be in charge of an infant and could fall asleep with the infant. Information and counseling about safe bedsharing should be provided even to those parents for whom bedsharing should be discouraged (those with hazardous conditions or circumstances), as one must assume that parents may bedshare anyway, even if unintentionally (level 1).
33
See Table 3 for risk minimization strategies. These discussions can include how to make sleep areas as safe as possible, and can reflect how to minimize hazardous circumstances, even if they are not eliminated (See Table 2). For instance, if a parent who smokes is bedsharing, breastfeeding, sleep positioning, sleep surface, bedding, and where infant naps when alone can all be discussed.
Elements of Safe Bedsharing Advice, in Order of Importance
Risk Minimization Strategies for Families in Which Bedsharing Is High Risk
Conversations when a family is bedsharing should be nonjudgmental and acknowledge context
Ending stigma around bedsharing and educating all parents about safe bedsharing have the potential to reduce infant deaths. Bedsharing evolved from innate human biological and behavioral mechanisms. It is not a singular, discrete, or coherent practice, but is composed of a diverse range of behaviors, some of which may carry risks, making it particularly important to discuss bedsharing safety.
Discussing the concept of breastsleeping with breastfeeding parents allows a way to discuss safe bedsharing in this context. Using the theory of planned behavior, counseling about safe breastsleeping is most likely to be effective if it is consistent with both social norms and attitudes (level 2). 34
Scripting tools are important resources.35,36 Beginning with an open-ended inquiry helps to identify an understanding of patients' and families' lived experiences. It is critical to recognize that evidence-based medicine integrates “compassionate use of individual patients' predicaments, rights, and preferences” (level 5). 23 Nonjudgmental counseling helps to build trusting patient–professional relationships for both disclosure and effective counseling (level 5). 10
Public policy recommendations
Structural societal interventions are essential interventions regardless of counseling on sleeping arrangements. As many parents will have limited contact with the health care system,
33
advocating for structural changes is critical. Policymakers should address the following strategies that may lower infant mortality:
Increasing tobacco prices, a strategy associated with an immediate marked decrease in infant mortality in Europe (level 5).
37
Ending racial bias in the health care system that undermines breastfeeding and leads to poor maternal and infant outcomes(level 2)38,39 (level 3).
40
Advocating for the allocation of research funding and resources focusing on the risk factors for sleep-related infant death commensurate with the evidence-based level of risk.
Evidence Base and Supporting Material
Definitions
SIDS is defined as the sudden death of an infant that is unexplained after a case review and/or autopsy and death scene investigation have been performed. SIDS has a specific code, R95, under the International Classification of Diseases, 10th Revision (ICD-10). 56 The code for “other ill-defined and unspecified causes of death” (R99) is used when the cause of death is unknown or there is inadequate evidence to classify as SIDS, as when SIDS is suspected but a full investigation has not been performed. Accidental suffocation or strangulation in bed (ASSB, W75) is coded when the death was due to asphyxia, strangulation, or suffocation, in a bed, crib, sofa, or armchair.
Sudden unexpected infant death (SUID), also known as sudden unexpected death in infancy (SUDI), is an overarching term for all unexpected deaths, both those that remain unexplained (coded as R95 or R99) and those in which a full causal explanation is eventually found.
Proxy measure for SIDS: For any international comparisons for the purpose of this protocol, we use a proxy measure for SIDS by adding deaths assigned to these three codes together (R95 + R99 + W75) as a composite measure of unexplained SUDI (or SUID). 57 This is due to our recognition of the diagnostic shift pointed out by Taylor et al. 58 and Shapiro-Mendoza et al. 59 over the past decade in which some pathologists and medical examiners seem reluctant to use SIDS (R95) because the diagnosis requires the exclusion of any other cause of death. Therefore, the use of codes R99 or W75 is preferred, despite incomplete or minimal evidence that overlaying (accidental smothering) may be the causal factor. Diagnostic shift toward ASSB (W75) is more common in the United States than in the United Kingdom. 60
Bedsharing is defined as an infant sharing an adult bed with an adult for sleep, and for this protocol we are defining this as with the infant sleeping next to a caregiver, most often the mother. The bed may consist of a mattress or futon with varying levels of firmness depending on the filling.
Cosleeping is a term that may include both sleeping on a shared surface and sleeping in proximity, but not necessarily on a shared sleep surface. For clarity, “cosleeping” is not used in this protocol.
Separate versus solitary sleep: We refer to “separate sleep” as room-sharing without bedsharing, whereas “solitary sleep” refers to sleeping in a separate room from parents.
History, context, and anthropology of infant sleep location
Human milk, lower in solute compared with milk of other species (e.g., bovine), 61 is digested very quickly. The rapidly growing infant breastfeeds at least 8–12 times in 24 hours. 62 Frequent feeding is difficult if the infant is not in close contact with his or her breastfeeding mother day and night.1,8 Parent–infant bedsharing with breastfeeding constitutes the human evolutionary norm as demonstrated in anthropological research.63–67
In industrialized countries until the early 20th century, most infants were bedsharing and breastfeeding. 68 After that time, solitary sleep developed as an ideal among the middle classes, reinforced by the growing trends of artificial feeding and medicalization of childbirth, separating infants from mothers.65,68 Sleep training also became increasingly popular in some industrialized societies. 68 Human milk substitutes (e.g., infant formula) helped this trend, as infants who receive them tend to feed less frequently 69 and may sleep more deeply than breastfed infants. 70
Concerns about infant sleep duration and location did not appear until after the late 19th and early 20th centuries in industrialized countries, 68 indicating that infant sleep research has taken place within an historical context in which feeding of human milk substitutes and solitary sleep promotion were normative. Although parents and caregivers in the majority of cultures sleep in proximity to their infants, organizations in some countries, including the United States, Canada, and Germany, recommend that even breastfeeding mothers should never share a sleep surface with their infants.10,71–73
The concept of “breastsleeping” was proposed to describe a biologically based model of sustained contact between the mother and infant, starting immediately after birth, in which sleeping and breastfeeding are inextricably combined, assuming no hazardous risk factors.15,64 Described in cultures around the world, the breastsleeping mother and infant feed frequently during the night while lying in bed together, and by morning, the mother may not recall how many times she fed or for how long. 74 The breastsleeping concept acknowledges the critical role that immediate and sustained maternal contact plays in helping establish optimal breastfeeding63,75,76; and recognizes that the behavior and physiology of breastsleeping dyads may be different from that of bedsharing nonbreastfeeding dyads, signifying that the safety assessments for bedsharing with breastfeeding versus feeding human milk substitutes likely require different approaches.4,21,77,78
When breastfeeding mothers sleep with their infants, they protect them from potential physiological stressors including airway covering and overheating by their characteristic sleep position (curled around their infants, making a constrained sleep space with their bodies), known as the C-position 48 or “cuddle curl” 49 (Fig. 1). Their continued vigilance through microarousals prompts regular infant arousals throughout the night.21,78–80 In two small video studies, mothers who had never breastfed were observed to exhibit these protective behaviors less frequently.78,81

C-position or “Cuddle curl.” Breastsleeping mothers adopt a characteristic position (Protective C or Cuddle Curl) in which they make a safe space for their baby to sleep with their bodies. Mother's arm is above the baby's head preventing him/her moving up the bed into the pillows, and her knees are tucked under his/her feet to prevent him/her moving down the bed. Baby is positioned flat on his/her back on the flat mattress for sleep, and next to the mother's breasts for easy feeding. © Baby Sleep Information Source, licensed for use under Creative Commons, 2016. Color images are available online.
Compared with breastfeeding infants who sleep alone, breastsleeping infants spend less time in stages 3–4 (deep) sleep, and more time in stages 1–2 (lighter) sleep, facilitating rapid infant awakening and termination of apneas. Additional time nurturing through breastsleeping, as compared with less time nurturing when sleeping separately, may affect epigenetic responses to stress in the infant through the possible influence of maternal care on infant regulatory responses. 82
Despite decades of advice to avoid mother–infant sleep contact, researchers report that on any given night, 20–25% of U.S. and U.K. infants <3 months of age share a bed with a parent for sleep at least some of the nights,83,84 and >40% of infants in Western * societies, in general, do so at some point in the first 3 months.83,85–91 These proportions may be underreported due to the stigma associated with bedsharing, especially in the United States. Parents express various reasons for sleeping with their infant, including deeply rooted cultural or religious beliefs and parenting philosophies, physiological links between lactation and nighttime breastfeeding, and a biological compulsion that drives the urge for close contact.25,89,92–94 They explain that sleeping with their infant makes nighttime care easier, helps them monitor their infant, provides comfort, and still allows them to sleep.8,25,95 Sometimes parents report having nowhere else to put their infant at night, or that they have fallen asleep with their infant unintentionally.25,89,96 Others report bedsharing in response to either the mother or her infant being deaf, to keep infants safe from environmental harms (i.e., vermin, gunfire, and earthquakes) and to protect them from SIDS.97–99
Breastfeeding mothers comprise the largest group of bedsharers. 92 Sleep contact between mother and infant facilitates nighttime breastfeeding, with multiple studies demonstrating that bedsharing is associated with more frequent nighttime feeds (promoting milk production), and more months of breastfeeding2,4,14,90 (Fig. 2). Those women with the strongest prenatal intention to breastfeed are more likely to bedshare, 4 whereas breastfeeding women who did not initially intend to bedshare often end up doing so.8,100 Although bedsharing breastfeeding mothers wake frequently to feed, they are awake for shorter periods and fall back to sleep more rapidly. 79 Thus they achieve greater sleep duration 101 than nonbedsharing mothers. 14 Bedsharing is a strategy used by breastfeeding mothers to reduce physical and social costs, for example, sleep disruption. 102 One observational study has shown that, compared with mothers who room-shared without bedsharing, mothers who bedshared were more likely to report exclusive breastfeeding (adjusted odds ratio [OR]: 2.46; 95% confidence interval [CI]: 1.76–3.45) or partial breastfeeding (adjusted OR: 1.75; 95% CI: 1.33–2.31).7,103 Therefore, advice to avoid bedsharing has the potential to undermine breastfeeding goals,3,8,104,105 and may increase risk of sleeping in unsafe environments such as sofas. 106

Bedsharing is strongly associated with breastfeeding continuation. Source: Ball et al., 2016.
Although mothers and infants can sleep apart and still breastfeed exclusively, doing so results in fewer sessions of breastfeeding per night: bedsharers have double or triple the number of breastfeeding sessions and total amount of breastfeeding time compared with solitary sleepers. 6 Fewer than half as many feedings occurred for mothers whose infants slept alone in a bedside bassinet (Fig. 3a) in the postnatal ward compared with a sidecar (Fig. 3b) or with bedsharing in a randomized trial examining breastfeeding initiation. 1 In one study among a population with low breastfeeding rates, advice to room-share without bedsharing achieved a similar duration of “any” breastfeeding, but not exclusive breastfeeding. 22
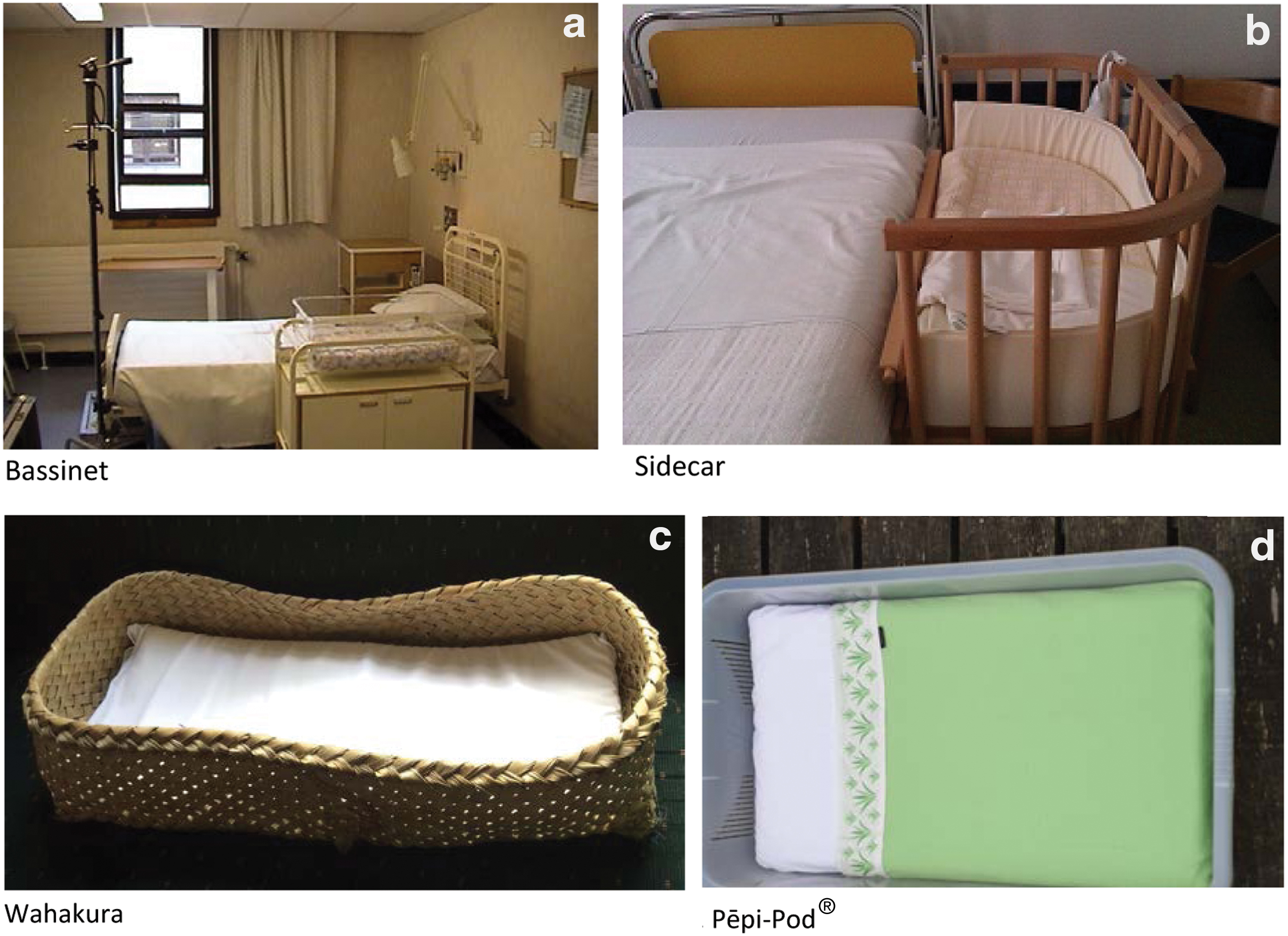
Bassinet, sidecar, wahakura, and Pēpi-Pod®.
Bedsharing and SIDS: epidemiological/observational evidence
Feeding of human milk substitutes (formula) is associated with a markedly increased risk of SIDS. 42 This may be due to lower infant arousal thresholds and increased infection risks compared with breastfeeding dyads. 52 In addition, videographic studies show that breastsleeping infants consistently sleep with their heads well below pillows as they are positioned near their mother's breasts,21,78,81 which might lower suffocation risk, in contrast to infants who are fed human milk substitutes, who have been noted to be placed intentionally on or around pillows. Videographic data show that breastsleeping infants rarely sleep prone.21,81 Hauck et al. made the case that breastfeeding is causally associated with a reduction in SIDS based on biologic plausibility, consistency of findings, strength of association (which has since gotten stronger 42 ), timing of association, and dose–response effect, and is not merely a marker for other protective factors including absence of tobacco smoke or sociodemographic factors. 52 The protective mechanism is unknown. However, it is likely to be a combination of maternal behavioral factors, immunological and nutritional properties of human milk, and the physiological influence of sucking on arousal.
Approximately half of SIDS cases occur when infants are sleeping alongside an adult as shown in recent observational case–control studies, with the remainder of deaths occurring among infants who sleep alone in a cot/crib.9,11 In a longitudinal study in England of 300 consecutive SIDS deaths for a 20-year period, the total number of bedsharing SIDS deaths decreased by half after the “Back to Sleep” campaign. 107 However, in this cohort there was a sevenfold reduction in deaths that occurred in the crib/cot, which suggests that placing infants prone to sleep was far more common among those infants sleeping alone than among bedsharing infants.11,107 This trend also resulted in a higher proportion of deaths that occurred among bedsharing infants, despite a numerical decrease in bedsharing deaths, because of the lower number of overall deaths. This statistical rise in the proportion of bedsharing deaths led policymakers in some countries to recommend against bedsharing, including the American Academy of Pediatrics, beginning with its 2005 statement.10,108 In a meta-analysis of 11 SIDS case–control studies published in 2012, there was a pooled threefold risk associated with bedsharing, although this did not reach significance in older infants (>12 weeks) or those not exposed to tobacco smoke, and the risk was only significant for unintentional bedsharers, not routine bedsharers. In addition, breastfeeding was not included in the analysis. 109
The interaction between infants bedsharing next to mothers who smoked, as a risk for SIDS, first identified in the New Zealand Cot Death Study in 1993, 31 was more than fourfold (OR: 4.55 [95% CI: 2.63–7.88]) compared with no risk among infants sleeping next to nonsmoking mothers (OR: 0.98 [95% CI: 0.44–2.18]) in this case–control study. 32 Antenatal smoke exposure is not merely a marker for socioeconomic status as it is associated with reduced infant arousal, and with pathologic findings in the brains of exposed infants.29,30
A combined analysis of 400 SIDS infants and 1,386 controls from two English studies demonstrated an 18-fold increase in SIDS deaths if either an infant slept with an adult on a sofa or slept next to an adult who drank >2 U of alcohol within a 24-hour period (2 U equals 1 pint or large can of beer [440 mL], 1 glass of wine [175 mL], or 2 shots of spirits [50 mL]), with a 4-fold risk with bedsharing if parents smoked. 11 In the absence of hazards, there was no risk of SIDS with bedsharing compared with nonbedsharers (room-sharing or solitary sleeping) (OR: 1.08 [95% CI: 0.58–2.01]). When the data were divided into younger (<3 months) or older infants, an increased but not statistically significant risk in the younger infants (OR: 1.6 [95% CI: 0.96–2.7]) and a significant protective effect for nonhazardous bedsharing among the older infants (OR: 0.08 [95% CI: 0.01–0.52]) were apparent. Further study with larger number of infants would be needed to properly assess any differential effect by infant age or impact of other factors such as parental drug use, infant sleep positioning, or room-sharing.
In contrast, in a similar combined analysis, a fivefold increased risk was associated with younger infants bedsharing in nonhazardous circumstances. 9 However, the reference group for this study was female breastfed infants placed on their backs next to the beds of nonsmoking parents in the absence of any other risk factors. This magnified the risk difference and renders this explanation not generalizable and difficult to interpret, because both protective factors (detailed in the reference group) and potential risk factors (bedsharing) are being quantified at the same time.
Limited data exist on the risk of bedsharing with caregivers other than the mother. A single study from inner city Chicago in the United States found an increased death risk with multiple bedsharers (other children alone or other children with one or both parents) and nonparent bedsharers, 50 but a causal relationship is unclear. In a Scottish study, a markedly increased risk of death was found if the infant was sleeping between two parents, 51 but this study did not account for alcohol and/or drug use, which is notable as the United Kingdom has a high prevalence of heavy episodic drinking (27.1% among those aged 15 years and older) compared with other industrialized countries. 110
SIDS epidemiology
SIDS is most common among low-income46,107 and some marginalized communities in wealthy countries, with the world's highest prevalence of SIDS occurring among U.S. American Indians/Alaskan Natives (combined) and non-Hispanic blacks, New Zealand Māori, Australian Aboriginal and Torres Strait Islander peoples, and indigenous Canadians. 33 Bedsharing is often common and culturally valued in these marginalized communities. However, there are also many populations with high bedsharing rates that have low rates of SIDS,33,111 including Swedes, 33 U.S. Asians, and U.S. Hispanics (Fig. 4). These conflicting observations may be explained by the presence or absence of a variety of attendant hazardous risk factors. 33 The overlap of many of the hazardous circumstances with conditions of poverty, structural racism, and legacies of historical trauma must be noted, including antenatal smoking, alcohol use, preterm birth, poor prenatal care, and lack of breastfeeding (feeding human milk substitutes). In the United States, fewer than half of the mothers of infants who died of SIDS received timely prenatal care, 33 which has been demonstrated as associated with SIDS elsewhere.112,113 Structural racism also plays a role. For example, African American infants are more likely to be given human milk substitutes in the hospital without a medical indication,38,39 undermining breastfeeding. Racial discrimination of Māori and Australian Indigenous peoples and other minorities by health professionals and society is associated with a wide range of negative health outcomes in New Zealand and Australia.40,114
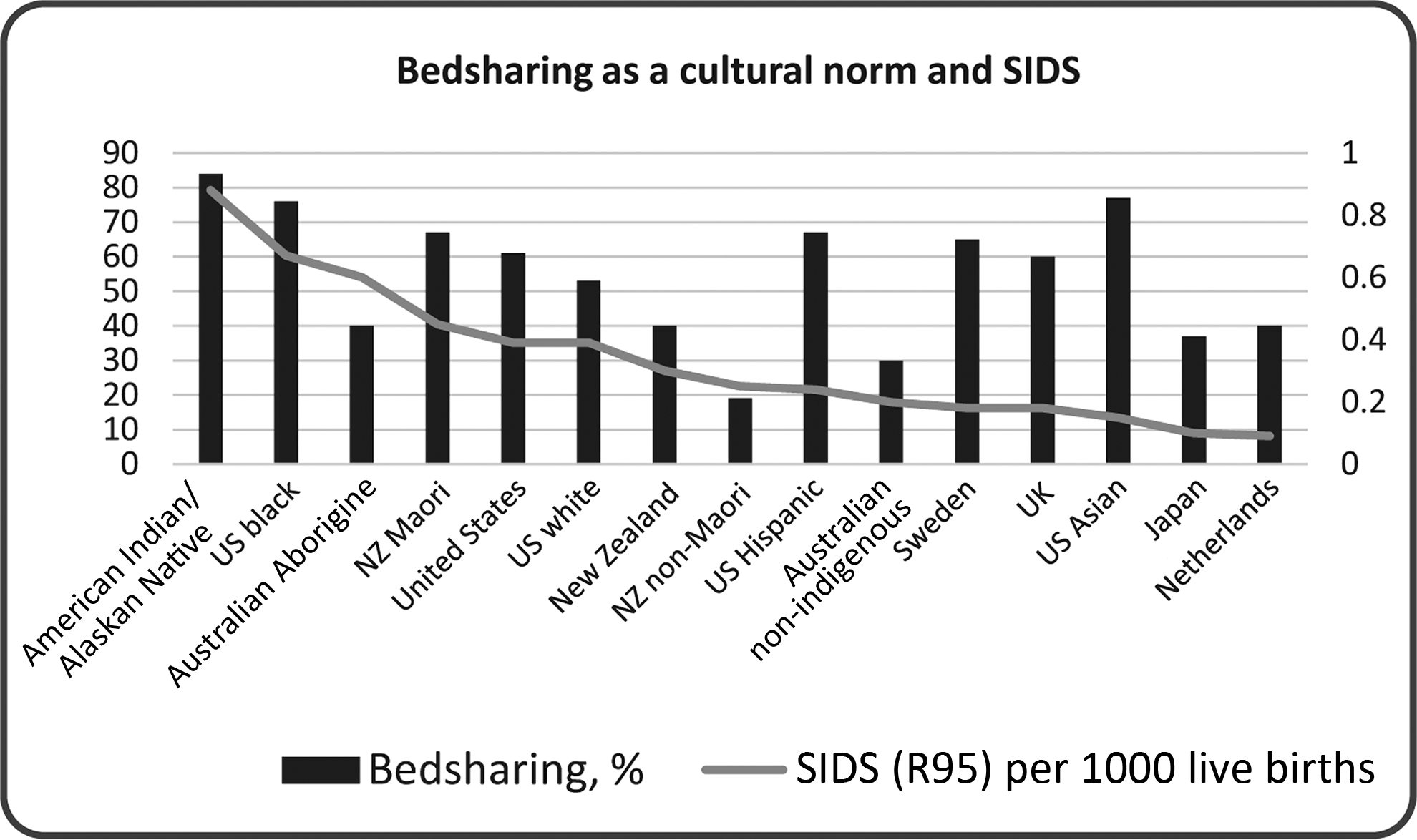
Bedsharing (any) as a cultural norm and SIDS. Source: Taken from data from Bartick and Tomori, 2019. Most SIDS data are 2014. Australia groups are 2008–2012, Japan is 2015, The Netherlands and Sweden are 2013. Aborigine here refers to both Australian Aborigines and Torres Strait Islanders (combined). SIDS, sudden infant death syndrome.
Risk minimization policies and strategies
Various policies have been adopted to advise parents about bedsharing over the past decade. Countries including the United States, Canada, and Germany 73 have opted to advise against bedsharing. The conclusion of a 2014 review of all international case–control studies for 20 years by the independent U.K. body, the National Institute for Health and Care Excellence, was that bedsharing in itself is not causal for SIDS, and that parents should be informed of the specific hazards associated with this practice. 115 In contrast to the countries advising against all bedsharing, countries such as the United Kingdom and Australia 116 acknowledge that bedsharing occurs both intentionally and unintentionally and is often linked to breastfeeding. Thus, they advise health practitioners to openly discuss the particular circumstances when it would be risky to bedshare.
Although the United Kingdom and Australian approach lacks the simplicity of the predominant U.S. approach, it is more closely aligned to the evidence, which acknowledges that bedsharing is widespread and may be culturally valued. This strategy allows the issue to be discussed without judgment, and for specific hazardous situations to be emphasized.48,117,118 The U.S. policy, while calling for nonjudgmental conversations with families about sleep practices, includes the recommendation to room-share without bedsharing. This is a clear direct message to the public that may appear easy to convey to policymakers. A disadvantage of this direct approach, as evidenced by the antibedsharing rhetoric in some campaigns, is the stigmatization that can prohibit honest discussion among parents and health professionals and offend bereaved parents who have lost an infant while bedsharing. Despite campaigns to decrease bedsharing, reported bedsharing has increased in the United States in recent years, especially among black and Hispanic communities.87,91 In one trial using enhanced messaging with high-risk families to avoid bedsharing, 119 bedsharing was no different than in the control group, and in both arms of the study, bedsharing increased over the first 6 months. Breastfeeding did not decrease, presumably because bedsharing was unaffected. 22 Taking into account diagnostic shift, the proxy SIDS rate (R95 + R99 + W75) in the United States with the strict “no bedsharing” policy appears to be almost unchanged (Fig. 5). In the United Kingdom, where parents are educated about safe bedsharing, the proxy SIDS rate has fallen over the past 10 years (Fig. 6). It is noted, however, that many different factors other than bedsharing may feed into these recent trends.
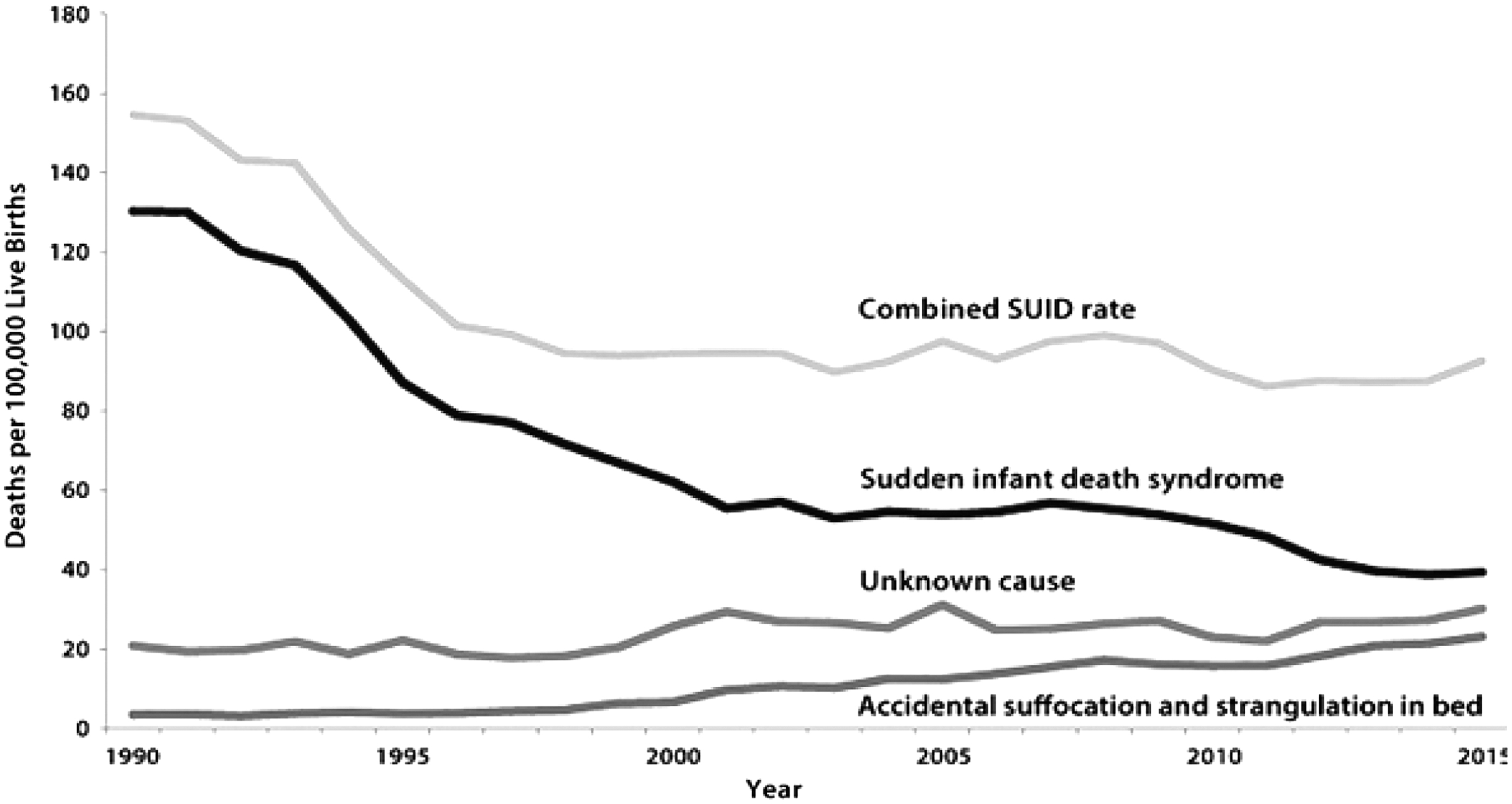
U.S. trends in SIDS and SUID (1990–2015). Source: Centers for Disease Control and Prevention/National Center for Health Statistics (CDC/NCHS), National Vital Statistics System, Compressed Mortality File. SUID, sudden unexpected infant death.

England and Wales trends in SIDS and SUID (2000–2015). Source: Office for National Statistics, England and Wales. SUDI, sudden unexpected death in infancy.
Risk minimization strategies include the recognition of the role of breastfeeding in SIDS prevention, the potential risk of bedsharing in the context of hazardous circumstances, and taking into account the importance of the partner and other support persons' involvement in sleep time activities (See Table 3).
Effectiveness of safe sleep interventions
A review of safe sleep interventions shows that most (primarily U.S.-based) one-on-one interventions are unsuccessful, including those addressing smoke exposure and sleep location. 120 One observational U.S. study showed that exclusively breastfeeding women were far less likely to adhere to advice not to bedshare than other women (65% versus 30.5%). 103 There has been some success reaching parents with text messages and e-mail with video, social networks, or other media,34,53,54,121 but this requires mobile phone and internet access. A simplistic “ABC-Alone, Back, Crib” approach is often rejected by families and caregivers, and has not been shown to decrease sleep-related deaths, leading to the adoption of a conversational approach, 35 which includes exploring patients' needs and perceptions and making informed decisions. 118 Annual U.S. surveys between 1993 and 2010 revealed that bedsharing rates among black and Hispanic families has continually increased, despite nearly half of U.S. nighttime caregivers discussing bedsharing with a physician. 91
New Zealand, whose Māori population until recently had the highest SIDS rate in the world, driven by high rates of smoking combined with bedsharing, 58 has seen reductions in infant death rates after a novel intervention. 122 It targets high-risk families with provision of the wahakura (Fig. 3c), a woven flax bassinet-like structure based on Māori traditions developed for this purpose, used on the bed, to create a separate sleeping space, and the Pēpi-Pod™ (Fig. 3d), a polypropylene box (food-grade plastic) of similar proportions. 123 Parents also receive one-on-one advice that promotes “Safe Sleep.” Importantly, the wahakura has the enhanced appeal of reclaiming a traditional Māori infant care practice that supports the highly valued proximity of mother and infant. 124 The high Māori SIDS rate dropped dramatically between 2009 and 2012, especially in targeted areas. 122 Interestingly, the wahakura did not decrease unsafe sleep behaviors compared with a bedside bassinet, but was associated with markedly increased breastfeeding rates at 6 months (wahakura: 22.5% versus bassinet 10.7%, p = 0.04). 55
Future areas of research
How can death investigation techniques be improved to determine whether the death of an infant can be fully explained by asphyxia?
Is there a significant risk from bedsharing in the absence of all hazardous circumstances?
Is there a relationship between bedsharing risk and infant age and mode of feeding (adjusting for all hazardous circumstances) (breastfeeding, expressed milk feeding, donor milk feeding, and human milk substitutes)?
What is the best advice for a safe sleep environment for nonbreastfeeding infants?
How do multiple bedsharers in the absence of hazardous risks, including bedsharing of twins, impact the safety of the infant? Does the location of the infant in the bed, for example, between the parents or on the edge of the bed next to the mother, make a difference for safety?
Are in-bed devices and sidecars safe and efficacious, especially for infants in high-risk situations, and if safe, what are their effects on breastfeeding?
Can the C-position (“cuddle curl”) be adopted by nonbreastfeeding bedsharers and is it effective in reducing SIDS?
Is providing supportive information to parents on “breastsleeping,” as defined in this protocol as a separate category of bedsharing, protective or risky to provide these parents with better specific guidance?
Is there autopsy evidence of the effect of feeding human milk substitutes that can establish a causal link between feeding human milk substitutes and SIDS?
Do the risks of death from SIDS due to early weaning and potentially related to the lack of safe bedsharing outweigh the risk of death from SIDS from bedsharing in nonhazardous circumstances? There are many confounders and this will be difficult to study.
To what extent does maternal obesity modify the risks and benefits of bedsharing?125,126
Footnotes
Disclosure Statement
J.J.M. serves as safety consultant for the Arms Reach co-sleeper for which he is paid a small honorarium but no royalties. No other competing financial interests exist. P.S.B. serves as the chair of the International Society for the Study and Prevention of Perinatal and Infant Death (ISPID) and is a scientific advisor to UNICEF UK, neither of which are funded positions. H.L.B. is scientific advisor to Lullaby Trust and chair of the Lullaby Trust Scientific Committee, board member of ISPID, and member of editorial review board for Journal of Human Lactation, which are all unfunded positions. As part of her academic role, she is co-founder and co-director of Basis, the Baby Sleep Information Source (www.BasisOnline.org.uk). J.J.M. serves as psychological advisor to Fit Pregnancy magazine, an unpaid respondent for the website Kids in the House, ![]() , and a board member of Speaking of Kids; L.F.W. works as a consultant and physician lead for Communities and Hospitals Advancing Maternity Practices (CHAMPS), Boston Medical Center, Boston, Massachusetts, and as a consultant to National Institute for Children's Health Quality (NICHQ)-National Action Partnership to Promote Safe Sleep Improvement and Innovation Network (NAPPSS-IIN). She is chair of the Section on Breastfeeding for the American Academy of Pediatrics (AAP) and also serves on the AAP Task Force on SIDS.
*
K.A.M. serves on the clinical advisory board of the US Baby-Friendly Hospital Initiative and is associate editor of the Journal of Human Lactation; M.C.B. has received funding from the W.K. Kellogg Foundation for research in breastfeeding and economics and co-leads the Massachusetts Baby-Friendly Collaborative. L.F.W. and M.C.B. serve on the board of the Academy of Breastfeeding Medicine.
, and a board member of Speaking of Kids; L.F.W. works as a consultant and physician lead for Communities and Hospitals Advancing Maternity Practices (CHAMPS), Boston Medical Center, Boston, Massachusetts, and as a consultant to National Institute for Children's Health Quality (NICHQ)-National Action Partnership to Promote Safe Sleep Improvement and Innovation Network (NAPPSS-IIN). She is chair of the Section on Breastfeeding for the American Academy of Pediatrics (AAP) and also serves on the AAP Task Force on SIDS.
*
K.A.M. serves on the clinical advisory board of the US Baby-Friendly Hospital Initiative and is associate editor of the Journal of Human Lactation; M.C.B. has received funding from the W.K. Kellogg Foundation for research in breastfeeding and economics and co-leads the Massachusetts Baby-Friendly Collaborative. L.F.W. and M.C.B. serve on the board of the Academy of Breastfeeding Medicine.
Funding Information
This work was unfunded.
ABM protocols expire 5 years from the date of publication. Content of this protocol is up-to-date at the time of publication. Evidence-based revisions are made within 5 years or sooner if there are significant changes in the evidence.
*
We understand “Western” as an ideological construct, not a geographic one.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.