
Abstract
Background:
Little is known about intended breastfeeding duration of women who initiate breastfeeding. We describe the association between intended and actual breastfeeding duration among low-income, diverse mothers who report maintaining breastfeeding for the first 2 months postpartum.
Materials and Methods:
We included mothers (64% Hispanic, 17% non-Hispanic black) participating in Greenlight, a cluster randomized childhood obesity prevention trial, who were providing breast milk at the 2-month preventive service visit and reported intended breastfeeding duration at this visit. Breastfeeding status was assessed at subsequent visits, up to 24 months. Poisson regression with a robust variance estimator was used to estimate risk ratios and 95% confidence intervals for meeting breastfeeding intentions. Covariates included race/ethnicity, income, receiving benefits from the Special Supplemental Nutrition Assistance Program for Women, Infants and Children (WIC), education, age, employment, depression, maternal obesity, U.S. born, whether infant was first born, and study site.
Results:
Median intended breastfeeding duration was 11.5 months (interquartile range [IQR]: 6–12) and median actual breastfeeding duration was 8.6 months (IQR: 4–14) (n = 349). Approximately half (49%) met intended breastfeeding duration. Breastfeeding duration differed based on milk type provided at the 2-month visit in that mothers providing mostly or only breast milk had increased likelihood of meeting breastfeeding intentions. Regardless of milk type provided at 2 months, the longer a mother intended to breastfeed, the less likely she was to meet her breastfeeding intentions.
Conclusions:
In this diverse sample of women less than half met breastfeeding intentions despite maintaining breastfeeding for 2 months. Understanding factors that prevent mothers from attaining intended breastfeeding duration is critical to improving breastfeeding outcomes, especially in low income and ethnic minority populations.
Introduction
Breastfeeding is associated with a multitude of benefits for both mother and baby.1,2 The American Academy of Pediatrics recommends infants receive breast milk until at least 12 months of life. 3 Overall, breastfeeding duration has increased in recent years, with 57% of babies born in 2016 breastfeeding at 6 months and 36% at 12 months. 4 However, breastfeeding rates among non-Hispanic black women are consistently lower compared with other races/ethnicities, and fewer low-income women continue breastfeeding compared with those with higher incomes.5,6 More Hispanic women initiate breastfeeding compared with national and other race/ethnicity rates, but duration is lower than other populations and below national targets. 7
Prenatal breastfeeding intentions are strongly associated with breastfeeding duration.8,9 However, breastfeeding intentions can change postnatally, and many mothers who initiate breastfeeding stop earlier than initially planned. 10 Poor initial breastfeeding experiences, particularly in the first 2 months, are a strong predictor of early breastfeeding cessation. 11 However, beyond 2 months, breastfeeding intentions and rates after initial initiation are not well understood. Understanding whether women who continue providing breast milk beyond the early postpartum timeframe attain their intended breastfeeding duration is important to determine and address barriers to sustaining breastfeeding, particularly after many mothers return to work. Our goal was to understand the relationship between planned breastfeeding duration and actual breastfeeding duration in a population of low-income, ethnically diverse mothers who were feeding their children any breast milk at 2 months. Specifically, we aimed to: (1) describe intended breastfeeding duration (in months) among mothers providing breast milk at the 2-month preventive service visit and (2) examine the association between postnatal breastfeeding intentions and actual breastfeeding duration, over the first 2 years of the child's life.
Materials and Methods
Study sample
This analysis includes a subset of mothers enrolled in the Greenlight Study, a cluster randomized obesity prevention trial conducted across four U.S. pediatric clinics that included 865 caregiver/child dyads during the first 2 years of life. The design and methods of Greenlight have been described in detail elsewhere. 12 Briefly, at baseline of the study at the 2-month preventive services visit, caregiver/infant dyads were enrolled if their caregiver spoke English or Spanish and was 18 years or older. Eligible infants were born ≥34 weeks' gestation, had birthweight >1,500 g, and had weight-for-recumbent length at the third percentile or higher per World Health Organization growth charts and no major health problems affecting growth. Two sites delivered a literacy- and numeracy-sensitive obesity prevention intervention, and two active control sites implemented an injury prevention curriculum designed by the American Academy of Pediatrics. For this analysis, mothers who reported providing their child any breast milk, that is, defined as breastfeeding or giving expressed breast milk, at the 2-month preventive service visit were eligible for inclusion (n = 460). All protocols were approved by Institutional Review Boards (IRBs) at all the sites and all participants provided written informed consent.
Breastfeeding duration
The main predictor variable was intended breastfeeding duration reported by mothers who were providing breast milk at the 2-month preventive service visit. To capture intended breastfeeding duration, the question was modeled after the Infant Feeding and Practices Study II. Mothers were asked in person by trained research staff “How old do you think [child's first name] will be when you completely stop feeding breast milk?” 13 Mothers who did not report an intended breastfeeding duration at the baseline visit were excluded from analysis (n = 14).
The primary outcome was actual breastfeeding duration. At each preventive service visit (2, 4, 6, 9, 12, 15, 18, and 24 months), mothers were asked to report the type of milk their child was receiving: “What type of milk does [child's first name] drink now?” Response options included: formula only; mostly formula and some breast milk; equal amounts of breast milk and formula; mostly breast milk, but some formula; and breast milk only. In addition to cessation of breast milk, we also report the extent of breastfeeding using these response options. Mothers who were missing responses at two or more consecutive preventive service visits (n = 27) and mothers who were lost to follow-up before reporting breastfeeding cessation were excluded (n = 70), leaving an analytic sample of 349 mothers. Breastfeeding duration was estimated by taking the midpoint of the child's age between the last reported intake of breast milk and the first reported intake of no breast milk. 13
A second outcome was whether intended breastfeeding duration was attained (yes/no). A mother was categorized as having met her breastfeeding intention if her last report of breastfeeding was greater than or equal to her intended duration. Similarly, mothers who were missing responses at two or more consecutive preventive service visits and mothers for whom we could not determine if breastfeeding cessation was before or after intended duration due to loss to follow-up were excluded (n = 71), leaving a sample of 375 mothers.
Covariates
Additional characteristics included in this analysis were selected based on existing literature and variables that were measured at the 2-month preventive service visit in the Greenlight Study. 14 These included the following maternal characteristics: age, race/ethnicity, education level, obesity (body mass index ≥30 kg/m2), employment (yes/no), household income, born in versus outside the United States, participation in the Special Supplemental Nutrition Assistance Program for Women, Infants and Children (WIC), and postpartum depression and whether the child was firstborn. The Center for Epidemiological Studies Depression (CESD) Scale was used to measure depression; a score of 16 or greater was used as a cutoff value for indication of being at risk for clinical depression. 15
Statistical analyses
Patient characteristics were summarized using frequencies and proportions for categorical variables or medians and interquartile ranges (IQRs) for continuous variables. The bivariate relationship of each covariate with intended and actual breastfeeding duration was assessed using Wilcoxon–Mann–Whitney tests for binary covariates and Kruskal–Wallis tests for categorical covariates. Intended breastfeeding duration was categorized and modeled using indicator variables with the shortest duration (<6 months) as the referent. Poisson regression with a robust variance estimator was used to estimate risk ratios (RRs) and 95% confidence intervals (CIs) for meeting intended breastfeeding durations. Regression covariates included baseline characteristics, such as race/ethnicity, income, receiving WIC benefits, education, age, obesity, employment (yes/no), depression, U.S. born, first born, and milk type at 2 months. We included a variable for study site to account for the Greenlight intervention effects. We assessed for effect measure modification for race, employment, and milk type at 2 months and categories of intended breastfeeding duration. All analyses were conducted using Stata 14 (StataCorp, College Station, TX).
Results
Over a third of mothers were providing breast milk only at the 2-month preventive service visit (34%), 38% were providing mostly breast milk, 2% were providing equal amounts of breast milk and formula, and 26% were providing mostly formula; most mothers who were providing breast milk were Hispanic (64%) with a mean age of 29 (standard deviation: 5.7) years. Over half of mothers were from households earning less than $20,000 per year (57%), over a quarter had less than a high school education (29%), and nearly a third had obesity (32%) (Table 1). Most were receiving WIC benefits (80%); 14% screened positive for depression at the 2-month preventive service visit; over two-thirds of mothers (67%) were not born in the United States; and over a third of the index participant infants were first born (38%). There were no significant sociodemographic differences associated with the type of milk provided at 2 months.
Baseline Characteristics of Mothers Providing Breast Milk at the 2-Month Preventive Service Visit Participating in the Greenlight Study and Intended and Actual Breastfeeding Durations (n = 349)
Missing 2.
Missing 10.
Missing 39.
Missing 7.
BMI, body mass index; IQR, interquartile range; SD, standard deviation; WIC, Special Supplemental Nutrition Assistance Program for Women, Infants and Children.
Intended breastfeeding duration
The median intended breastfeeding duration was 11.5 (IQR: 6.0–12.0) months. Intended breastfeeding duration varied by mother's age, with mothers younger than age 25 reporting the shortest intended duration (8.0 [IQR: 6.0–12.0] months), compared with mothers older than age 30 (10.3 [IQR: 6.0–12.0] months), and mothers 25–30 years of age (12.0 [IQR: 6.0–12.0] months) (p = 0.003) (Table 1). Intended breastfeeding durations also varied by level of education, with high school graduates reporting shorter intended durations, compared with those with less than a high school education or those with some college reporting longer durations (8.0 [IQR: 6.0–12.0] versus12.0 [IQR: 6.0–12.0] months, p = 0.005). Mothers with their first-born child reported shorter intended breastfeeding durations (9.0 [IQR: 6.0–12.0] versus 12.0 [IQR: 6.0–12.0] months, p = 0.044). Intended breastfeeding duration did not significantly differ by race/ethnicity, household income, obesity, employment, receiving WIC benefits, depression, or being born in the United States.
Actual breastfeeding duration
The median actual breastfeeding duration was 8.6 (IQR: 4.2–14.2) months. Mothers providing mostly formula breastfed for the shortest duration (3.4 [IQR: 3.2–7.4] months) compared with mothers providing mostly breast milk (9.5 [IQR: 5.3–14.3] months) and mothers providing breast milk only (11.4 [IQR: 8.5–17.3] months) (p < 0.001). Mothers younger than age 25 breastfed for the shortest duration (6.0 [IQR: 3.3–11.5] months), compared with mothers older than age 30 (9.3 [IQR: 5.2–14.3] months), and mothers 25–30 years of age (10.8 [IQR: 5.2–15.6] months) (p = 0.006). Non-Hispanic black mothers breastfed for shorter durations (5.8 [IQR: 3.4–10.8] months) than Hispanic mothers (10.2 [IQR: 4.9–14.6] months) (p = 0.029). Those born in the United States breastfed for shorter durations, compared with those born outside the United States (7.1 [IQR: 3.4–11.4] versus 10.1 [IQR: 5.1–14.5] months, p = 0.006). There was a nonsignificant difference in duration among mothers who were employed at infant age 2 months, compared with those who were not employed (7.7 [IQR: 3.9–12.5] versus 9.8 [IQR: 4.4–14.3] months, p = 0.228).
Intended and actual breastfeeding duration by milk type
Mothers providing mostly formula or equal amounts of breast milk and formula reported shorter intended breastfeeding durations (6.0 [IQR: 6.0–12.0] months and 6.0 [IQR: 6.0–8.0] months, respectively) compared with mothers providing mostly breast milk (12.0 [IQR: 6.0–12.0] months) or breast milk only (12.0 [IQR: 9.0–12.0] months) at 2 months (Fig. 1) (p < 0.001). Comparatively, mothers providing mostly formula or equal amounts of breast milk and formula breastfed for the shortest duration (3.3 [IQR: 3.1–7.9] months and 4.0 [IQR: 3.2–7.4] months, respectively) compared with mothers providing mostly breast milk (10.3 [IQR: 5.4–14.4] months) or breast milk only (11.4 [IQR: 8.5–17.3] months) (p < 0.001).

Median intended and actual breastfeeding duration by milk type among mothers participating in the Greenlight study (n = 349).
Meeting breastfeeding intentions
Overall, approximately half (49%) of mothers met their breastfeeding intentions. Among mothers providing breast milk only at 2 months, 60% met breastfeeding intentions compared with 52% of those providing mostly breast milk, 33% of those providing equal amounts of breast milk and formula, and 34% of those providing mostly formula. In an unadjusted model, the likelihood of meeting breastfeeding intentions decreased depending on the amount of breast milk provided at 2 months (Table 2). Compared with mothers providing breast milk only at 2 months, mothers providing mostly breast milk were 0.13 times as likely to meet breastfeeding intentions (RR: 0.87, 95% CI: 0.70–1.08), mothers providing equal amounts of breast milk and formula were 0.44 times as likely to meet breastfeeding intentions (RR: 0.56, 95% CI: 0.22–1.43), and mothers providing mostly formula were 0.43 times as likely to meet breastfeeding intentions (RR: 0.57, 95% CI: 0.42–0.78). These results were amplified in multivariable analyses adjusted for maternal sociodemographic factors (age, race/ethnicity, income, receiving WIC benefits, education, obesity, employment, depression, being born in the United States, and first-born child) and intervention site. There were no significant sociodemographic predictors for meeting breastfeeding intentions and no evidence of Greenlight intervention effects. Lastly, regardless of milk type provided at 2 months, the longer a mother intended to breastfeed, the less likely she was to meet her breastfeeding intentions (Fig. 2). Mothers who were excluded due to loss to follow-up reported longer intended breastfeeding durations at 2 months compared those who were not excluded (12.0 [IQR: 8.0–12.0] months versus 11.0 [IQR: 6.0–12.0] months, respectively, p = 0.002).
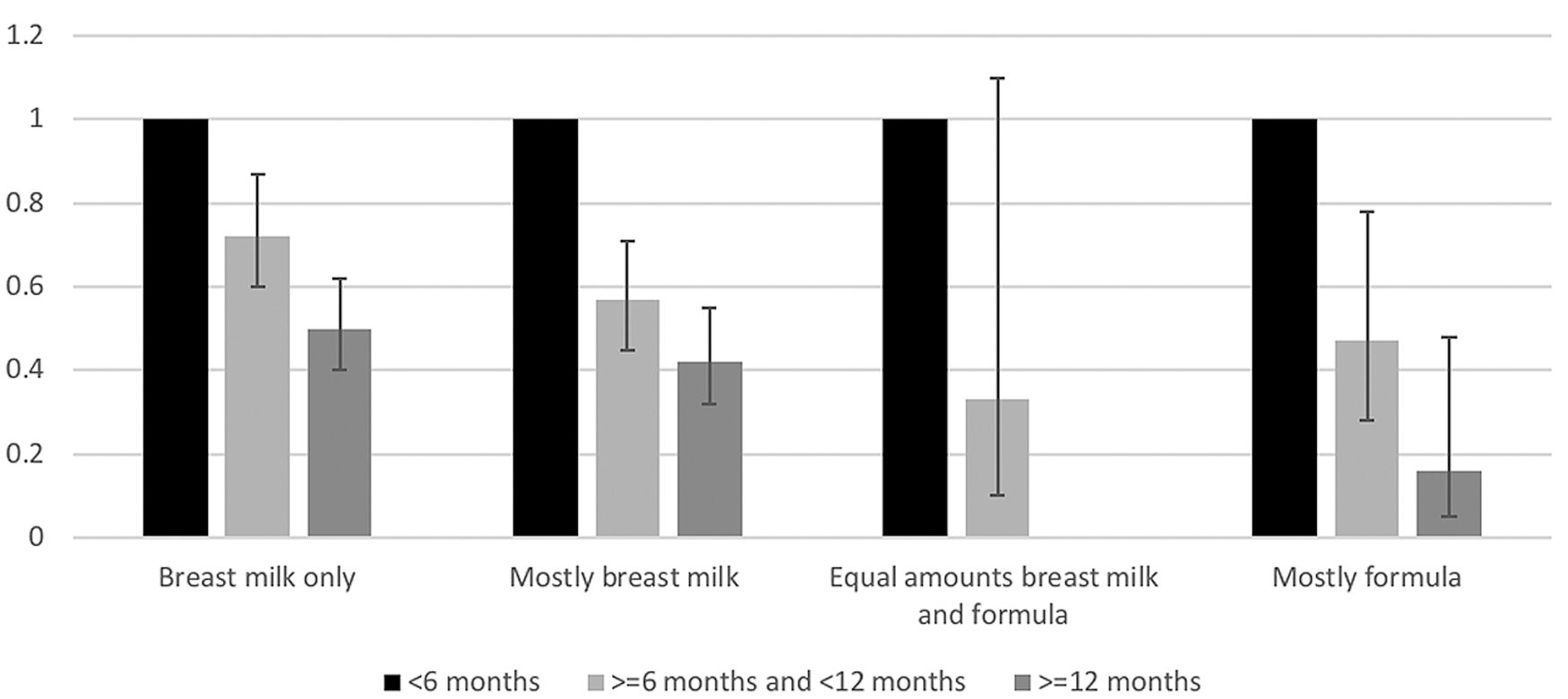
Risk ratios and 95% confidence interval for meeting intended breastfeeding durationsa by intended breastfeeding duration reported at 2 months, among mothers participating in Greenlight (n = 375). aMeeting intended breastfeeding duration was defined as actual breastfeeding duration > intended breastfeeding duration.
Risk Ratios and 95% Confidence Interval for Meeting Intended Breastfeeding Durations, Among Mothers Participating in Greenlight
Meeting intended breastfeeding duration was defined as actual breastfeeding duration ≥ intended breastfeeding duration.
Adjusted for maternal age, race/ethnicity, income, education, receiving WIC, obesity, employment, depression, being born in the United States, first born child, and intervention site.
CI, confidence interval; RR, risk ratio.
Discussion
Despite overcoming the well-documented barriers16,17 to initiating and maintaining breastfeeding in the early postpartum period, mothers still did not breastfeed as long as they planned. Approximately half of this diverse group of mothers who initially established breastfeeding actually achieved their intended breastfeeding duration. The more breast milk a mother provided at 2 months, the more likely she was to meet her breastfeeding intentions. However, it is still true that only 60% of mothers breastfeeding at the 2-month preventive service visit were able to meet their breastfeeding intentions. This study lends rich data to a scant literature assessing breastfeeding intention and breastfeeding duration after initiation and maintenance.
Other studies have demonstrated that, when measured prenatally, positive intent and attitude toward breastfeeding is associated with better breastfeeding initiation, but few have assessed how intention influences duration, particularly in the past 6 months.18–20 Measuring breastfeeding intentions among women who have already established breastfeeding and therefore have more practical experience, could be more informative compared with prenatal predictions. DiGirolamo et al. highlight the importance of including initial breastfeeding experiences when assessing maintenance of breastfeeding duration, for women with negative initial experiences with breastfeeding are less likely to continue breastfeeding. 20 This in combination with our results show that among mothers with longer postnatal breastfeeding intentions meeting expectations was more difficult, suggesting mothers may need increased support throughout the postpartum period to attain their breastfeeding goals. Many mothers may not anticipate the challenges associated with sustaining breastfeeding, leaving them ill equipped to overcome them. The support needed to sustain breastfeeding comes from many places, including health care providers, family, and friends. 21 Mothers with a partner, relative, or close friend with breastfeeding experience are more likely to breastfeed. 6 Social support, an important modifiable factor, could explain mothers' inability to meet breastfeeding expectations. 14 Future studies would benefit from determining the presence of social support and its effects on meeting breastfeeding intentions.
The relationship between breastfeeding intentions and actual duration was modified by milk feeding type in that mothers providing formula at 2 months were the least likely to meet breastfeeding intentions, regardless of intended breastfeeding duration. In multivariable analyses adjusted for maternal sociodemographic factors, the more formula a child was receiving, the less likely mothers were to reach intended breastfeeding durations. There are a multitude of medical (hypoglycemia, severe maternal illness, poor weight gain) and nonmedical reasons (maternal request) infants receive supplemental formula; and short-term use of small volumes of formula may not impact breastfeeding duration. 22 But early and sustained formula introduction can interfere with maternal milk supply because breastfeeding is a supply-and-demand system. Studies have demonstrated the negative effect early formula feeding can have on breastfeeding duration. 23 Nickel et al. found that early supplementation with formula was associated with a 10.5-week shortened duration of breastfeeding. 24 We are unable to discern reasons for formula use in our dataset, but since formula supplementation, particularly in larger volumes, can cause unintentional harm to breastfeeding, it is important for clinicians to communicate guidelines and resources for breastfeeding support that match mothers' breastfeeding goals and intentions within the first week of life or before.
Unique cultural factors may have affected mothers' abilities to meet expectations as over three quarters of the mothers in this study were Hispanic or non-Hispanic black, many were not born in the United States, and nearly half spoke primarily Spanish. Culturally, specific factors that may affect breastfeeding among racial/ethnic minority women include acculturation, literacy, and cultural acceptance/support. 25 Additionally, some minority women believe formula is a safer, more convenient, and nutritious alternative to breast milk.26,27 For example, it has been reported that use of “las dos cosas” or a combination of breast milk and formula feeding is common among Hispanic women due to perceived benefits of adding formula.28,29 However, as combination feeding without additional pumping can lead to insufficient milk supply, mothers may inadvertently compromise their abilities to meet their breastfeeding goals. 23 Expressing breast milk is not a common practice among Hispanic and non-Hispanic black women, leading to increased formula use when separated from the baby, such as for work or school.29,30 Many women report concerns about not having enough milk to meet their infant's needs, latching difficulties, pain, and embarrassment as reasons for stopping breastfeeding or supplementing with formula.31,32 Addressing such issues that are specific to racial/ethnic minority women, and designing culturally sensitive education interventions will be important in improving breastfeeding duration in minority populations.
While WIC is an important resource for providing breastfeeding support, some studies have found that WIC participation is associated with early breastfeeding discontinuation, particularly among racial/ethnic minority women.33,34 Mothers, particularly Hispanic mothers, report mixed messages when getting formula supplementation from WIC. 29 Women who plan to formula feed may be more likely to enroll in WIC due to a perceived financial advantage given the high retail value of formula. 35 Most (80%) of the mothers in our sample were receiving WIC benefits and it is possible that free provision of formula was a barrier to breastfeeding. Changes to the WIC food package in 2009 aimed to ameliorate this discrepancy by providing stronger incentives to breastfeed. 36 Evaluating the impact of these incentives and implementing further support, such as increasing the uptake of lactation consultants available to WIC participants, may further improve women's abilities to meet their breastfeeding goals.
Our analysis is notable given the diverse sample of mothers included. Our sample was largely Hispanic or non-Hispanic black with the majority receiving WIC benefits. A comparable study was conducted in a primarily white, educated population with greater loss to follow-up. 37 Our unique study sample from multiple geographical locations strengthens the generalizability of these results. However, this may not be a representative sample of low-income mothers in the United States. Further limitations to this work include potential misclassification bias as our method for estimating the outcome of actual breastfeeding duration assumed that breastfeeding ceased at the midpoint between the child's age at last report of receiving breast milk and first report of no longer receiving breast milk. This could have biased our results as children may have stopped receiving breast milk before or after that point. However, in sensitivity analyses using both the age at last report of receiving breast milk and the age at first report of no breast milk to determine actual breastfeeding duration, our method for estimating the outcome would have led to nondifferential misclassification. Additionally, mothers self-interpreted the level of breast milk they were providing; we chose to include all mothers who were providing some breast milk, however, we were unable to quantify the exact amount of breast milk or whether the child was breastfed directly or fed pumped breast milk in a bottle. In addition, as covariates were collected at the 2-month preventive service visit, it is possible that over the course of participation in the study, these covariates could have changed, such as depression, employment, and receiving WIC benefits; we were unable to account for these changes over time. In our multivariate analyses we only included those with complete data, but there is potential that our findings may be biased if those participants' missing data (n = 20) differed from those with complete data. Lastly, 16% of women who initially reported expected breastfeeding durations at their infant's 2-month preventive service visit dropped out of the study while still breastfeeding, but before their expected breastfeeding duration (n = 70). Since the primary outcome of actual breastfeeding duration could not be assessed for these women, selection bias may have been introduced, favoring women with shorter breastfeeding duration for which we were able to capture.
While we did not find significant sociodemographic predictors associated with meeting breastfeeding expectations, there may be important modifiable factors that we were unable to measure, such as breast pump usage, breastfeeding role models, and family history of breastfeeding. In addition, when assessing a WIC population, it is important to consider variations in sites in terms of breastfeeding support, from both medical providers and peer counselors, availability of pumps, and a lactation consultant that is on site. Lastly, in examining characteristics among mothers who were excluded from our study because they were not providing breast milk at the 2-month visit (n = 386), we found these mothers were far less likely to be Hispanic (34% versus 63%) and born outside the United States. (32% versus 70%). The excluded group was also less likely to make >$40,000 (11% versus 18%) and more likely to be depressed (21% versus 15%), employed (36% versus 27%), and receiving WIC benefits (91% versus 80%); they were also more likely to be younger (47% <25 years versus 30%). Characteristics, such as these are strongly associated with early breastfeeding cessation 38 ; therefore, future work should focus on engaging these women earlier in breastfeeding awareness and support.
Conclusions
In this racially/ethnically diverse cohort of low-income mothers who had established breastfeeding at the 2-month preventive service visit, most planned to breastfeed their child for at least 6 months, yet approximately half achieved their intended breastfeeding duration; this was influenced by the amount of formula mothers provided. In contrast to prenatal feeding intentions, which strongly predict breastfeeding initiation and duration, we found that many mothers were not able to meet their long-term breastfeeding intentions, particularly those with longer intentions. Further understanding of the factors that prevent all mothers, including economically disadvantaged and ethnic minority mothers, from attaining their intended breastfeeding duration, is critical to improving breastfeeding outcomes in the United States.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was supported by the National Institutes of Health (NIH)/Eunice Kennedy Shriver National Institute of Child Health and Human Development grant R01HD059794 with Centers for Disease Control and Prevention supplements 04S1 and 04S2; NIH grant UL1TR001111; NIH/National Center for Advancing Translational Sciences grant UL1TR000445; NIH/National Center for Research Resources grants U54RR023499, UL1RR025747, and UL1TR000038; Robert Wood Johnson Foundation Physician Faculty Scholars program (H.S.Y.); and Health Resources and Services Administration grant T32HP014001. Funded by the National Institutes of Health (NIH).