
Abstract
Background:
Nipple discomfort inhibits breastfeeding goals, particularly between 0 and 8 weeks postpartum (PP), and yet the specific dermatologic entities that contribute to nipple soreness have not been clearly delineated. Moreover, there remains a lack of evidence-based guidelines for nipple symptoms and skin diseases.
Methods:
A survey was distributed to 6–8-week PP women, 18–50 years of age, with an intent to exclusively or partially breastfeed (“at the breast” or “pump”). The study aimed to characterize nipple skin symptoms (pain and itching) and lesions (eczema, redness, cuts, or wounds) and any association between these nipple problems and past dermatologic history, breastfeeding outcomes, and the ability to meet her breastfeeding goals.
Results:
Findings paralleled Centers for Disease Control and Prevention (CDC) statistics with a 25% decline in breastfeeding rates between birth, 86.3% (189), and 6–8 weeks PP, 64.5% (145). By 6–8 weeks PP, exclusive “formula” and “exclusive feeding at the breast” showed the largest increase (+16.4%) and decrease (−22.9%), respectively. Although no significant difference was found in comparison of nipple problems to feeding methods or skin history, women who reported pumping or PP redness/eczema had higher odds ratios of a change in feeding practice, history of eczema, and sensitive skin. Strong pumping intentions were also associated with the highest risk of unmet breastfeeding goals.
Conclusion:
Regardless of feeding method, product, or provider use, PP nipple problems predominantly arose between 1 and 3 weeks PP. Clinical Trial Registration number 201901737.
Introduction
The stated intention to breastfeed is one of the strongest predictors of breastfeeding initiation, but the dynamic nature of breastfeeding is often affected by socioenvironmental factors and the experience itself. 1 Nipple pain and skin abnormalities are a major prohibitive factor for achieving breastfeeding goals, particularly within the 1–8 week postpartum (PP) period.2–5 Previous studies have identified the prevalence of self-reported nipple symptoms (pain and itch) in PP women to be as high as 79% and self-reported nipple damage at 58%. 6 Anecdotal evidence and self-reported data suggest several factors contributing to nipple soreness such as poor latch, low milk supply, flat or inverted nipples, mechanical stressors, infection, or exacerbations of inflammatory conditions (psoriasis or eczema).7,8 However, studies have not used discrete dermatologic entities to categorize the problem, thus also potentially limiting the ability to establish proper therapies. Topical products and medical devices (breast pumps, shells, or shields) are available over the counter (OTC), but they can inhibit the maternal-infant interaction and may even exacerbate pain.8–11 Second, there remains no clear, evidence-based guidelines regarding particular skin diseases of the nipple and their most effective treatment regimens, likely due to a lack and variability of data in current literature.
Although the majority of studies focus on infections of the nipple or breast tissue, the more prevalent complaints from breastfeeding include nipple dermatitis, fissures, pain, and itching.12,13 Comparisons between lanolin and other nipple products (all-purpose nipple ointment, warm/cold compresses, air drying, peppermint water, analgesics, and breast shields) have demonstrated equal effectiveness in reducing nipple pain and healing time, improving satisfaction and duration of breastfeeding.14–16 In a larger study by Dennis et al. in 2014 (656 PP women), no product superiority was observed when comparing glycerin pads, shells, lanolin, expressed milk, or ointment in treatment of nipple discomfort. 13 Despite evaluating 656 women in a trial of five products (glycerin pads, shells, lanolin, expressed milk, or ointment), Dennis et al. reported insufficient evidence to conclude which product was superior in treating nipple discomfort. Rather, they noted all therapies “mild-to-moderately” reduced symptoms, and all women reported a general reduction in pain 7–10 days PP regardless of product used. 13 A similar study was conducted by Morland-Schultz and Hill reporting no difference between topicals and commented on the dire need for early breastfeeding education, particularly anticipatory guidance regarding nipple pain. 17 In contrast, Gungor et al. identified olive oil as the preferred PP nipple treatment when compared to lanolin. 18
The purpose of this study was to characterize the incidence and risk factors for nipple symptoms (pain and itch) in 6–8 week PP women, and to characterize the incidence of self-reported skin entities (redness, eczema, cuts, and open wounds). It also aimed to evaluate any relationship between nipple skin symptoms/lesions (Fig. 1), dermatologic skin history, and breastfeeding outcomes. As secondary outcome measures, we sought to clarify which products are commonly utilized and which health care providers are primarily caring for this patient population.
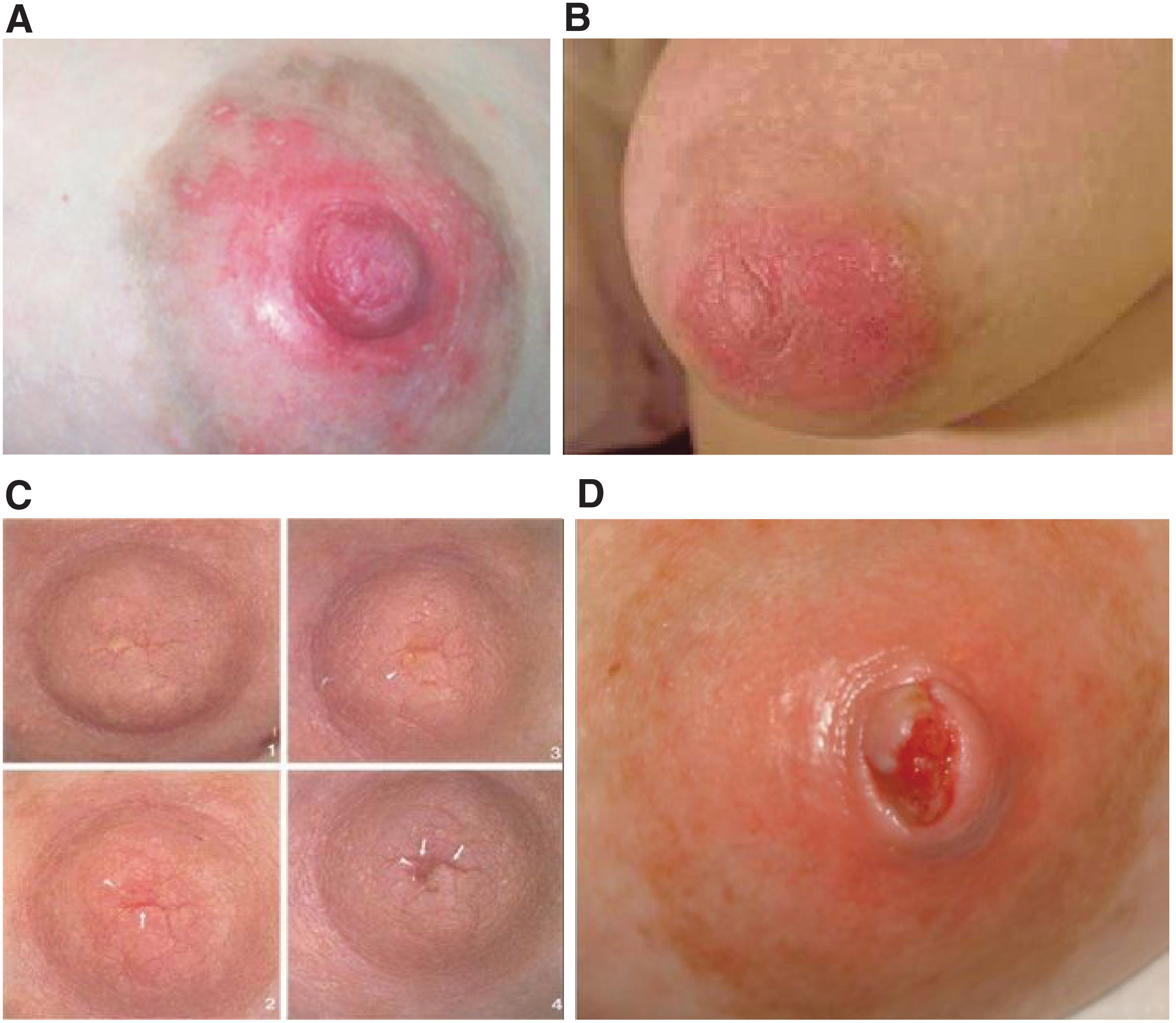
Nipple skin lesions.
Methods
A review of literature was performed using the key phrases “nipple dermatitis,” “nipple pain,” “nipple itching,” “nipple soreness,” “breastfeeding,” “formula feeding,” “breast pumping,” and “nipple treatments” on the following databases: PubMed, CINAHL, and ClinicalKey. This search could not identify literature addressing maternal skin history, such as atopic dermatitis, psoriasis, or other chronic cutaneous disorders, in the context of breastfeeding difficulties.
A single-site cross-sectional study was performed using a 13-question, paper survey developed by the University of Iowa Hospitals and Clinics (UIHC) Departments of Dermatology, and Obstetrics and Gynecology. The project was reviewed and accepted by the UIHC Institutional Review Board (ID: 201901726).
The survey was distributed to our population of interest: 6–8 week PP mothers, 18–50 years of age, with expressed intention to exclusively or partially breastfeed. The study excluded non-English-speaking patients, females younger than 18 years or older than 50 years, and respondents outside the 6–8 week PP window. It also excluded patients unable to independently complete the questionnaire. In a 4-month recruitment period, the study aimed to survey 200 eligible participants, a goal achieved with 220 respondents.
Upon survey dissemination, consent was implied and participants were instructed to leave questions blank, which they did not wish to answer. Accordingly, patients were not excluded for lack of survey completion. All surveys remained anonymous and no chart review was performed for this study. Accordingly, no names, medical record numbers, or other identifiers were collected. Survey responses were documented in a secure database (REDCap). The REDCap platform is managed by the Institute for Clinical and Translational Science at the University of Iowa and access is limited to IRB-approved research team members.
Statistical analysis was performed using the latest software of SAS (9.4, University of Iowa Institute for Clinical and Translational Science) with a significance level set at p < 0.05. Demographic and survey data, compiled in the REDCap database, included both continuous and categorical variables. Fisher's exact test and Cohen's kappa coefficient were used to determine significance and measure of agreement, respectively, among pairs of categorical variables. Stratified variables were listed as a percentage with corresponding “n” number. In regard to feeding methods, the term “breastfeeding” corresponded to feeding “at the breast.” Subjects were asked about all types of feeding, including (1) exclusive breastfeeding, (2) breastfeeding with pumping and bottle feeding of expressed breast milk, (3) breastfeeding and/or pumping with formula supplementation, and (4) exclusive formula. “Intended” practices (breastfeeding, pumping, and/or formula) represented day 0, while “current” practices represented 6–8 weeks PP. For data analysis, we also defined “change” in feeding practices as any deviation at 6–8 weeks from intended (day 0) method. Odds ratios (OR) with a 95% confidence interval were applied to categorical values with a binomial distribution. We also defined “nipple symptoms” as nipple pain or itching, as well as “nipple skin lesions” as redness, eczema (atopic dermatitis), cuts (fissures), or open wounds of the nipple.
Results
Among 220 survey respondents, 219 met inclusion criteria for statistical analysis. Upon survey distribution (6–8 weeks PP), the average age of mothers and infants was 30.0 years and 48.4 ± 5.5 days, respectively. The majority of women, 84.5% (185), identified as “white, non-Hispanic” for their race and ethnicity and had previously breastfed one or more infants, 46.6% (102). Review of dermatologic medical history identified a predominance of environmental allergies, 27.4% (60), asthma, 12.8% (28), and eczema 9.6% (21) (Table 1). Evaluation of feeding intentions (day 0) versus current practices (6–8 weeks PP) determined a majority, 52.5% (115), and minority, 5.0% (11), reported intent to exclusively “breastfeed” and “formula” feed, respectively. Feeding practices at 6–8 weeks, however, largely incorporated pumping and formula: 36.4% (80) reported “breastfeeding with pumping” and 21.4% (47) exclusive formula. By weighted Kappa analysis (SAS 9.4), the interrater reliability among responders of planned versus current feeding practices was 0.2442, 95% confidence interval (CI 0.1407–0.3437), SE 0.0518, correlating to a “fair” degree of consistency (Table 1). Among respondents who changed their intended versus current method at 6–8 weeks, “exclusive breastfeeding” showed the greatest reduction in frequency, −22.9%, while “exclusive formula feeding” showed a net +16.5% increase (Table 2). Findings also showed none of the women, 5.0% (11), who intended to exclusively formula feed deviated from this plan by 6–8 weeks PP. By Fisher's method (SAS 9.4), statistically significant differences were identified when comparing intended versus change in method (p = 0.0003) as well as current versus change in method (p < 0.0001).
Demographics of Survey Participants
Feeding Intentions and Current Practices
To further evaluate breastfeeding outcomes, we examined possible associations between feeding plan, nipple problems, and dermatologic history (eczema or allergies) (Fisher's exact, SAS 9.4). No significant difference was identified in comparison of intended (p = 0.1039) or current (p = 0.7485) breastfeeding method to self-reported nipple skin lesions (cuts/open wounds and redness/eczema) experienced between 0 and 8 weeks PP (Fig. 1). Similarly, no significant difference was determined among women who changed their feeding method and reported nipple skin lesions (p = 0.9753). Comparison of formula use, history of eczema (p = 0.1520), or allergies (p = 0.5383) to nipple skin lesions also revealed no significance difference. Although 36.1% (79) of total participants (219) reported a history of “environmental” allergies, only 2.7% (6) identified skin sensitivities to lanolin, lotions, soaps, or fragrances.
We also sought to determine possible associations between nipple complaints and change in feeding practices, history of eczema, or sensitive skin (Table 3). Nipple complaints were again characterized as nipple lesions (cuts/open wounds and redness/eczema) or nipple symptoms (pain or itching) arising in between 0 and 8 weeks PP (Fig. 1). Irrespective of breastfeeding method, nipple complaints predominantly occurred between 1 and 3 weeks PP. Among women who reported nipple pain with breastfeeding (53.2%) and pumping (38.3%), the latter method had a higher OR, 2.00, 95% CI (1.09–3.67), of change in PP feeding practices. Pain with breastfeeding had a greater association with a history of skin allergies (sensitive skin), although did not achieve statistical significance, OR 1.39 (0.74–2.62). In comparison of nipple itching with pumping (14.2%) and breastfeeding (21.0%), the former had a greater association to all categories: change in feeding practice (OR 2.46 [1.00–6.04]), history of eczema (OR 3.66 [1.23–10.89]), and sensitive skin (OR 0.72 [0.27–1.92]). Categories were also compared to nipple skin lesions, including 10.2% (22) who reported PP cuts/wounds and 14.4% (31) who reported redness/eczema, irrespective of breastfeeding method (Fig. 1). Development of redness/eczema had a higher risk association with both change in feeding method, 1.08 (0.50–2.31), and history of eczema, 2.70 (0.96–7.61), while cuts/wounds were more associated with skin sensitivity, 1.59 (0.63–4.01) (Table 3).
Associations Between Nipple Symptoms, Dermatologic History, and Change in Feeding Practice
“Breastfeeding” refers to feeding “at the breast.”
OR, odds ratios.
To further elucidate determinants of breastfeeding success, survey measures (categorical variables) were compared in relationship to women who did and did not meet their breastfeeding goals. Regardless of intended plan versus outcome, 7.3% (16) women stated their breastfeeding goals had not been met at 6–8 weeks due to nipple problems. Comparison of demographic variables or feeding plan to breastfeeding goals revealed no significant difference. Nipple symptoms (pain or itching) by method (breastfeeding or pumping) revealed one significant association to impaired goals. Nipple pain with pumping was reported in 38.5% (67) women, of which 16.4% (11) reported unmet goals with a significance of p = 0.0138, OR 1.31 (1.33–12.11). Few women, 7.9% (3) and 8.0% (2), reported impaired goals with nipple itching while breastfeeding and pumping, respectively. Comparisons to self-reported nipple skin symptoms (cuts/wound and redness/eczema) were statistically significant (p = 0.0003) with a higher prevalence, 31.8% (7), of unfulfilled goals among women with cuts/wound. Evaluation of products (nipple shields, lanolin; n = 148, p = 0.0256) and provider use (MD and non-MD; n = 154, p = 0.0018) also revealed statistically significant differences. A higher prevalence of unmet goals was identified in women using both nipple shields and lanolin, 20.8% (5), as well as those seeking care from both MD and non-MD providers, 38.5% (5).
Among all participants (n = 219), the most commonly used products included, lanolin 62.1% (136), gel pads 25.6% (56), and nipple shields 16.0% (35). Survey results regarding health care providers utilized in this population were more variable. In the mother-baby-unit, 46.2% (101) of women sought care from lactation consultants and 37.0% (81) from nurses. Although women received care from OB and pediatric physicians, no women were evaluated by internal medicine or dermatology specialists.
Discussion
Nipple pain is common in the early PP period and a common contributing factor to premature cessation of breastfeeding, particularly as traumatized nipples can become exquisitely tender as reported by several women in survey study by Williamson et al. 19 In evaluation of 219 PP women, our survey data parallel the 2018 Centers for Disease Control statistics with a majority, 86.3% (189), reporting intent to exclusively feed at the breast with or without pumping, and a 25% decline in breastfeeding rates, 64.5% (145), as early as 6 weeks PP. Trends among breastfeeding patterns also demonstrated a decrease in women “breastfeeding exclusively,” 52.5% (115) to 29.6% (65), with a predominant increase in formula use followed by pumping (Table 2). Many a times, the reality of unmet expectations contributes to difficulties during this time, and this study provides data that could inform potential nursing mothers about these challenges. Pain during breastfeeding has been linked to new-onset depression, anxiety, and mastitis, all of which contribute to formula supplementation or lack of breastfeeding with subsequent infants.6,20–22 Additional risk factors reported for nipple pain include cesarean sections, Raynaud's syndrome causing vasospasm of the nipple, various medications, breast cancers, and autoimmune diseases.23–29
Analysis of breastfeeding cessation, intended plan versus method at 6–8 weeks, showed a significant decline in feeding at the breast by 6–8 weeks regardless of the presence or absence of nipple skin problems or dermatologic skin history. Notable differences were, however, identified in comparison of nipple problems by feeding method and skin history. Women who reported pumping or PP redness/eczema had higher OR of a change in feeding practice (0 to 6–8 weeks PP), history of eczema, and sensitive skin (Table 3). In contrast, women with cuts/wounds had a higher prevalence of unmet breastfeeding goals. Interestingly, the contribution of nipple itching, redness, wounds, and/or dermatitis to cessation or change in breastfeed method was not identified in previous literature, although a few studies showed a decline in breastfeeding secondary to “nipple cracks” and the broader category of “nipple soreness.”30–32 The majority of research otherwise focuses on “nipple pain” as a primary cause of breastfeeding difficulties. Our findings suggest that antenatal review of the dermatologic history may identify individuals at increased risk for nipple problems during lactation, and that anticipatory guidance surrounding nipple wound care is an important lever to prevent cessation of breastfeeding.
Because our study supports a correlation between changes in nipple skin and breastfeeding practices, management of breastfeeding women should include skin health and symptom management. Common practices for nipple comfort include natural or OTC products that have little, if any, rigorous scientific support and may even be dangerous. Natural therapies include warm compresses and moist heat. Women are also encouraged to continue breastfeeding to relieve milk supply and breast engorgement, as well as alternate breastfeeding positions and ensure a proper latch.13,33 The most commonly recommended OTC products include glycerin pads, peppermint water, and lanolin- and dexpanthenol-containing creams.9,14,34,35 Study findings corroborate previous literature, in which lanolin and nipple shields were most commonly utilized by survey respondents; however, a significant difference was also shown in comparison of nipple product(s) and respondents' abilities to meet their breastfeeding goals. Some women are also counseled on the common occurrence of nipple tenderness, and that nipple skin will simply “adjust” within 1–2 weeks of breastfeeding.
While many different interventions for nipple pain are available, it is unclear which are most effective. 13 In addition, controversies remain in regard to their safety profile of OTC products. Peppermint oil may present safety hazards for young nursing infants, and while temporarily providing a “cooling” effect, can also have a drying effect on skin that leads to weakening of the skin barrier, making the delicate nipple skin even more subject to irritation. Furthermore, if peppermint is applied to the nipple, it should be cleansed before next feeding to avoid inadvertent ingestion by the infant. Likewise, the prevalence of hypersensitivity reactions to lanolin is gradually increasing so avoidance of potential allergens such as lanolin is recommended.36,37
These products stand in contrast to standard therapies recommended by dermatologists for itching, eczema (atopic dermatitis), wounds, or burns on skin surfaces, which include topical anti-inflammatory corticosteroids, topical calcineurin inhibitors, phototherapy, and/or oral antihistamines.38–40 For skin with barrier compromise, less is more when it comes to washing the skin and avoiding soap is de rigueur. Instead, frequent application of bland emollients is recommended along with use of moisture retentive dressings when the skin is open with cuts, abrasions, or ulcers. Blisters heal better when unbroken and maintaining a moist wound healing environment benefits all skin, including nipples.41–43
Because previous studies, corroborated by our data, identify a predominance of nipple pain, itching, or skin changes in the first (1–3) weeks of breastfeeding, it suggests anticipatory guidance and early intervention may optimize breastfeeding outcomes.2,4,13 On average, mothers and infants undergo 36 health care visits with their health care providers in the first year, most involving their general practitioners. 2 Our data demonstrate that the majority, 70.3% (154), received prenatal/postnatal breastfeeding counseling, particularly from nursing staff or lactation consultants in the mother-baby unit. Despite the prevalence of nipple pain/itching or skin lesions, only 6.0% (13) sought care from a licensed physician, and 0% respondents were seen by a dermatologist or internists. Although primary care providers should be well equipped in assessing and addressing breastfeeding problems, an obvious gap exists as studies demonstrate incorrect advice or treatment failure is another major cause of breastfeeding cessation.44–46
In addition to establishing evidence-based guidelines for antenatal or PP nipple care, a greater understanding of nipple skin conditions is imperative as malignancies of the breast can easily be mistaken for benign conditions. To enhance current practices, we propose improved education and earlier intervention of breastfeeding complications due to skin changes. Furthermore, an integrated approach between specialists should be considered, such as pediatricians, obstetricians, and dermatologists. For example, Naimer et al. identified a benefit in use of dermoscopy in identification of microscopic/macroscopic nipple skin issues. 46
Strengths of this study include the large sample size of women surveyed within the 6–8-week PP window. In future work, we plan to address the weaknesses of this study by expanding our survey population to multiple sites, including community-based facilities, larger metropolitan areas, and regions with added diversity. Our survey could be expanded to include additional personal history, such as previous breastfeeding difficulties and utilized products, history of C-section(s), complications in birth, or skin conditions, and social demographics such as working status. Additional reasons for ceasing breastfeeding may also be queried; for example, working mothers may choose formula over breastfeeding due to time constraints. A similar survey design, but prospective analysis, could be pursued to identify prenatal breastfeeding intent with follow-up at either or both 1 and 8 weeks PP. These historical variables would help to identify potential confounding variables. Finally, we hope to further categorize breast pathology in PP women using accurate dermatologic terms that will give precision to the clinical analysis of these entities, thereby opening up further avenues for treatment.
Conclusion
Treatment options and provider guidelines for nipple discomfort and skin issues arising in breastfeeding PP women remain limited. To enhance understanding, key factors contributing to nipple trauma must first be established, hence the creation of this survey study. Findings suggest nipple pain, itching, and skin trauma most commonly arise in the first (1–3) weeks PP, despite receiving breastfeeding guidance from one or more lactation consultants. Over 1/4th of women with intent to breastfeed had to forgo feeding at the breast, and supplement with formula or a pump. The survey also revealed OTC products, including lanolin cream and nipple shields, as mainstay treatment for nipple complaints. Although the study design cannot define a correlation between types of nipple trauma and most effective treatments, these data will add to the existing body of knowledge on management practices for nursing mothers, which may ultimately aid women in meeting their personal breastfeeding goal and improve overall breastfeeding rates. The value of the information gathered in this study is revealing a potential relationship between underlying dermatoses (eczema), sensitive skin, and incidence of nipple problems.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported, in part, by the University of Iowa Institute for Clinical and Translational Science (UI CTS), which is granted with Clinical and Translational Science Award funds from the National Institutes of Health (UL1TR002537).