
Abstract
Background:
The rates of “any” human milk use in neonatal intensive care units have improved during the last decade. However, efforts to help mothers in expressing and maintaining mother's own milk (MOM) through discharge remain a concern. This study aims to improve MOM in preterm neonates.
Methods:
The study was a quality improvement (QI) initiative conducted from May 2018 to April 2019. All preterm neonates <34 weeks were included. In the “initiation phase” (May 2018 to August 2018), a breastfeeding support group was formed and mothers were given structured antenatal and postnatal counseling regarding MOM using videos and leaflets. This improved MOM rates when compared with retrospective controls. In the continuation phase (August-2018 to April-2019), various plan-do-study-act cycles were conducted to test strategies such as frequent telephonic reminders, standardization of Kangaroo mother care, nonnutritive sucking protocols, and involving family members during daily counseling sessions. The initiation and continuation phases were compared with the retrospective baseline data.
Results:
Of a total of 125 preterm neonates, 27 were excluded for various reasons. Within 3 months of initiating the study, the proportion of neonates who received MOM within first 24 hours improved from 24% in retrospective controls to 82.9% in the initiation phase (p < 0.0001) and remained stable at 90.3% in the continuation phase. The amount of MOM received on day 1 increased significantly (p < 0.0001) from a median of 0 mL to 1 mL in the initiation phase and was maintained at 3 mL in the continuation phase. Amount of MOM increased significantly on day 3 (p = 0.0003) and day 7 (p = 0.03). Babies discharged on MOM also improved significantly (p = 0.005) from 48.3% in the retrospective cohort to 77.4% in the continuation phase. The number of babies receiving total parenteral nutrition decreased significantly (p = 0.02) from 54.6% to 26.7%.
Conclusions:
QI has shown promising results in improving MOM in preterm neonates.
Introduction
The importance of mother's own milk (MOM) as the principal source of nutrition for infants is undisputed and constantly emphasized in the literature.1–3 MOM in the preterm population has several advantages such as lower risk of various morbidities (necrotizing enterocolitis, retinopathy of prematurity, and late-onset sepsis); establishing gastrointestinal maturity and normal microbiota; and improved neurodevelopmental and cognitive outcomes.2,4,5 However, mothers of preterm babies have difficulty in initiating and sustaining MOM for a long time after birth of the baby. This remains a global concern as evidenced in the existing literature.6,7 Several factors are responsible for the decrease in MOM, depriving preterm babies of MOM. Earlier studies reported that very few preterm babies were discharged on MOM. 8 We faced similar challenges of establishing and maintaining MOM through discharge in our neonatal intensive care unit (NICU). Our quality improvement (QI) initiative attempts to increase MOM rates in preterm babies. We had earlier demonstrated a significant improvement in the milk expression with a team approach and well-planned antenatal and postnatal interventions. 9 As a continuation phase of the QI initiative, we conducted various Plan-Do-Study-Act (PDSA) cycles to improve the number of preterm babies on MOM through discharge.
Materials and Methods
The study was conducted at a tertiary care level IIIB NICU in India from May 2018 to April 2019. Inborn preterm (<34 weeks) neonates were included in the study. Neonates of critically ill mothers requiring intensive care admission, neonates with major congenital anomalies, or neonates requiring gastrointestinal surgeries were excluded from the study (Supplementary Fig. S1). The procedures followed were in accordance with the ethical standards of the Institutional Committee on human experimentation and with the Declaration of Helsinki. The study was approved by the Institutional Ethics Committee and informed consent was obtained from parents of the babies.
A MOM support group was formed, including a senior neonatologist, NICU resident, a nurse in charge, three staff nurses (one in each work shift), and a lactation counselor. A driver diagram (Fig. 1) was developed, and a detailed root cause analysis (Fig. 2) was done in discussion with this group. From May 2018 to August 2018 (initiation phase), mothers received structured antenatal and postnatal counseling regarding MOM through videos and leaflets explaining the methods of milk expression and importance of MOM, respectively.
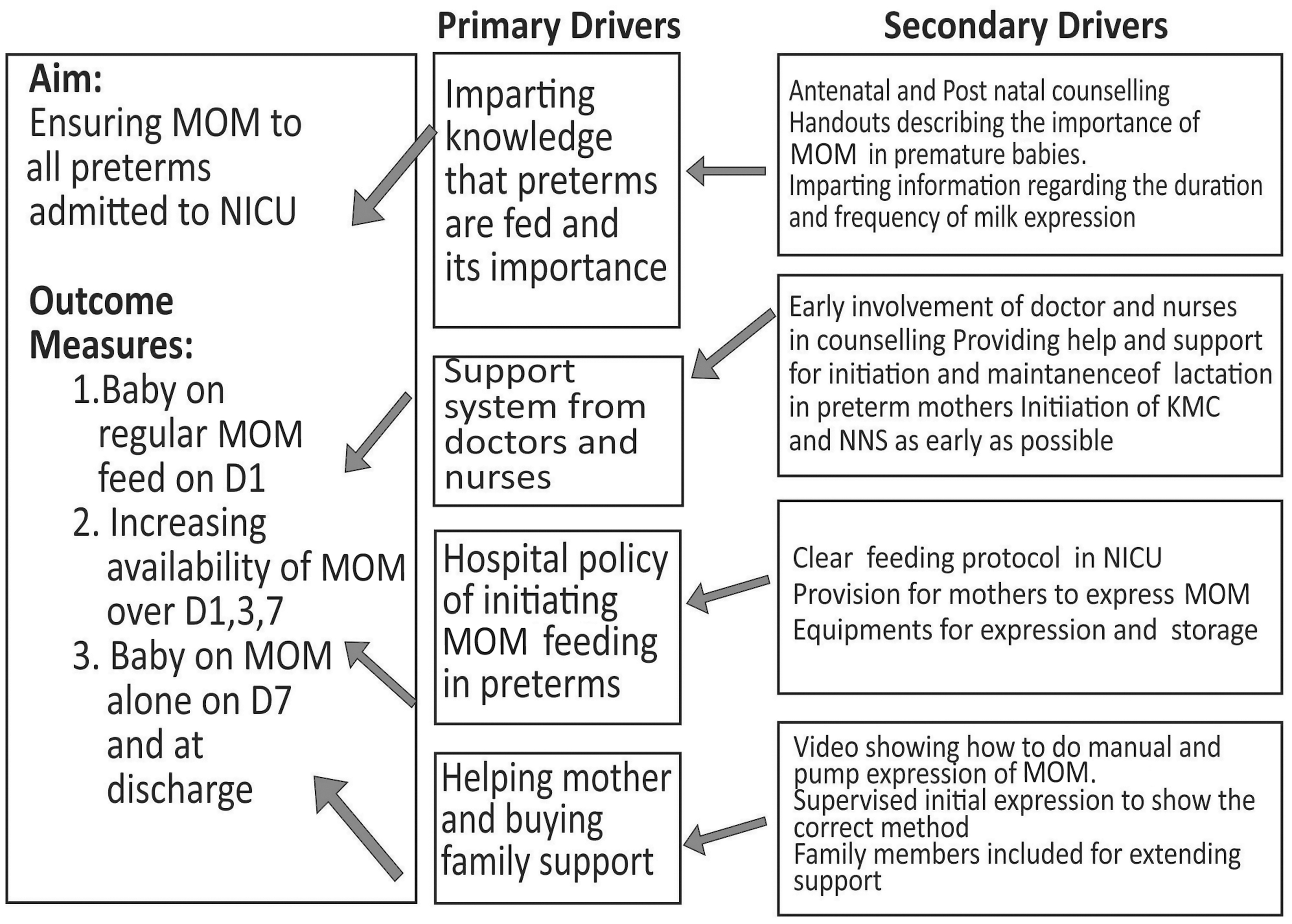
Driver diagram. MOM, mother's own milk; NICU, neonatal intensive care unit.
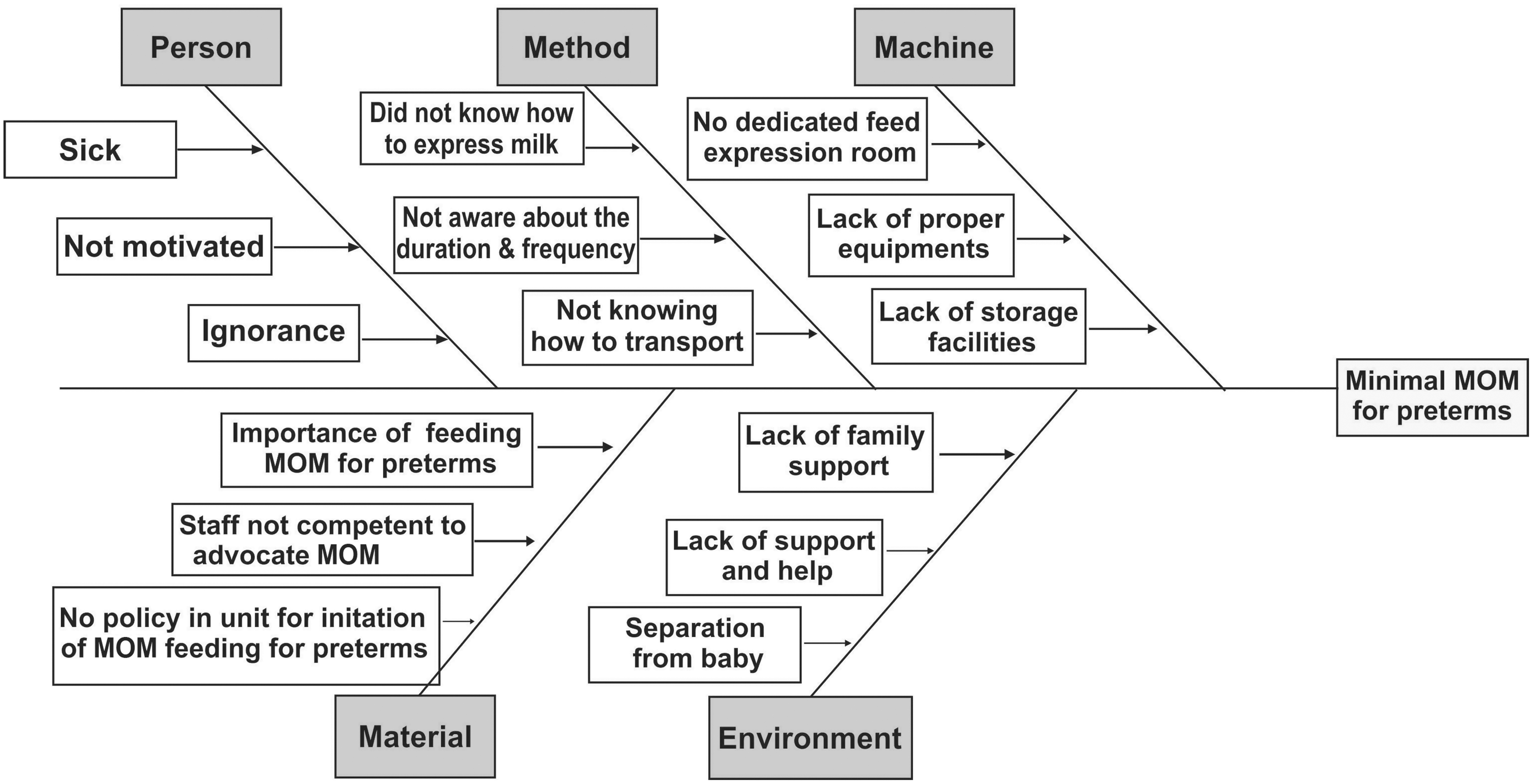
Fish bone analysis—detailed root cause analysis. MOM, mother's own milk.
The results of the initiation phase were encouraging when compared with those of the retrospective cohort (from February 2018 to April 2018), the details of which are available in an earlier study. 9 Some new evidence-based interventions were added, focusing on early milk expression and sustenance of MOM, and tested in the continuation phase (September 2018 to May 2019) for further improvement (Box 1 insert). In the continuation phase, Kangaroo mother care (KMC) and nonnutritive sucking (NNS) protocols were further standardized and assessed for every preterm baby during daily rounds. Mothers received telephonic reminders before every feeding even after they were discharged. NICU consultants were requested to include MOM counseling in the twice-daily routine counseling and involved other family members as well. Staff were trained rigorously, and all bedside nurses were trained to follow workflow. Regular feedback was obtained from mothers and staff. Changes were analyzed as a part of PDSA cycle (Fig. 3).

PDSA cycle. KMC, Kangaroo mother care; MOM, mother's own milk; NNS, nonnutritive sucking; PDSA, Plan-Do-Study-Act.
The neonatal resident in the support group collected data every day in the breastfeeding QI proforma, specially designed for the study. The assessment included the proportion of mothers expressing milk within 24 hours, number of babies on MOM on day 7, and number subsequently at discharge. Amount of milk expressed on days 1, 3, and 7, the time to reach full feeds, and the time to regain birth weight were compared. Data were collected on the rates of necrotizing enterocolitis (NEC), culture positive sepsis, hemodynamically significant patent ductus arteriosus (hs-PDA), periventricular leukomalacia, bronchopulmonary dysplasia (BPD), and number of babies requiring total parenteral nutrition (TPN).
The initiation phase and the continuation phase were compared with retrospective controls in a three-way analysis. The statistical analysis was performed using the software Origin v7.0 (OriginLab Corporation, Northampton, MA). Continuous data were checked for the normality of distribution by Shapiro–Wilk test. Since the distribution was nonnormal, data were described in medians and interquartile ranges (IQR) and compared among three groups by Kruskal–Wallis test. Categorical data were described in proportions and compared among three groups by Chi-square test. Post hoc analysis between any two groups was performed by Chi-square test or Fisher Exact test for categorical data and Mann–Whitney test for continuous data. A p-value of <0.05 was considered statistically significant. For post hoc analysis using multiple comparisons, a p-value of <0.025 was considered statistically significant after adjustments for Bonferroni correction.
Results
During the study period, a total of 125 babies <34 weeks were admitted, and 97 were included in the study as per inclusion criteria (Supplementary Fig. S1). Among these 97 babies, 35 were part of “Initiation phase” and 62 belonged to “Continuation phase” and were compared with 30 retrospective controls. Neonates in the initiation phase were slightly younger in gestation (p = 0.05) than those in the continuation phase, but comparable in terms of birth weight and gender. Within 3 months of initiating the study, the proportion of preterm neonates who received MOM within first 24 hours improved significantly (p < 0.0001) from 24% to 83% in the initiation phase and remained stable (90%) in the continuation phase.
The amount of MOM received on day 1 increased significantly (p < 0.0001) from a median of 0 mL (IQR, 0–0 mL) to 1 mL (IQR, 0.5–4 mL) during the initiation phase and maintained at a median of 3 mL (IQR, 1–7 mL) in the continuation phase. All mothers expressed milk within 24 hours. The amount of milk expressed on day 3 increased significantly (p = 0.012) from a median of 6 mL (IQR, 0–18 mL) to 15 mL (IQR, 8–36 mL) during the initiation phase and maintained at a median of 20.5 mL (IQR, 12–48 mL). By day 7, quantity of milk expressed increased (p = 0.005) from a median of 60 mL (IQR, 40–120 mL) in retrospective controls to a median of 100 mL (IQR, 60–156 mL) (Table 1).
Demographic Profile and Primary Outcomes
Bold values represent statistically significant p-values ≤0.05.
Table compares the demographic profile of neonates and the amount of MOM among the study groups and published work. The published data on retrospective cohort with no QI initiative intervention 9 were reproduced here with rights for reference.
Post hoc analysis showed that only initiation and continuation phases were significantly different from each other (p = 0.015).
Post hoc analysis showed that only published work was significantly different from initiation (p < 0.0001) and continuation (p < 0.0001) phases.
Post hoc analysis showed that only published work was significantly different from initiation (p < 0.0001) and continuation (p < 0.0001) phases.
Post hoc analysis showed that only published work was significantly different from initiation (p = 0.012) and continuation (p = 0.0001) phases.
Post hoc analysis showed that only published work and continuation phase were significantly different from each other (p = 0.005).
IQR, interquartile range; MOM, mother's own milk; N/A, not available; QI, quality improvement.
Babies discharged on MOM improved significantly from 48.3% in retrospective controls to 77.4% in the continuation phase (p = 0.005). Babies with culture positive sepsis showed a decreasing trend over the study period, although a three-way comparison was not statistically significant. The number of babies requiring TPN was significantly lesser during the continuation phase, 54.6% versus 26.7% (p = 0.02; odds ratio of 0.30 with 95% CI 0.12 to 0.74). Other outcomes such as time to reach full enteral feeds, time to regain birth weight, rates of NEC, BPD, hs-PDA, and duration of hospital stay were comparable in both phases (Table 2).
Secondary Outcomes
Bold values represent statistically significant p-values ≤0.05.
Table compares the secondary outcomes among the study groups and published work. The published data on retrospective cohort with no QI initiative intervention 9 were reproduced here with rights for reference.
Odds ratio: 0.30 (0.12–0.74).
Post hoc analysis showed that only published work and continuation phase were significantly different from each other (p = 0.005).
DOL, day of life; IQR, interquartile range; MOM, mother's own milk; N/A, not available; QI, quality improvement.
Discussion
We started our quality initiative to improve MOM with a structured approach, care bundles, and formation of a “MOM support group” as mentioned in previous literature.10–12 The support group developed detailed guidelines for overall MOM policy in the unit. They also observed problems related to early initiation of MOM and maintenance through discharge as in other studies13,14 and made a root cause analysis as depicted in Figure 2.
In our earlier QI initiative, 9 we successfully motivated most of the preterm mothers for early milk expression (within 6 hours) through structured antenatal and postnatal counseling and informative leaflets and videos. All mothers were able to express milk within 24 hours comparable to other studies.15,16 Timing of first milk expression is associated with lactation success. 10 Hence, the QI project was continued on a larger scale for 9 months, adopting additional evidence-based and potentially best practices reported in previous studies.3,17,18 This not only helped in early and frequent milk expression but also improved volume of early milk expressed on days 1, 3, and 7. A significant outcome of our study was more preterm babies with increased rates of MOM at discharge. During the initiation phase, 57.1% babies were discharged on MOM, as in previous reports. 19 However, this increased significantly to 77.1% during the continuation phase. A similar QI initiative by Bixby et al. demonstrated that a multidisciplinary approach improves MOM through discharge. 2 Early milk expression and sustenance of adequate volume of MOM helped babies in reaching full feeds sooner and significantly decreased the number of babies requiring TPN.
Spatz proposed 10 steps to promote and protect MOM in vulnerable infants. Our nursing staff adopted similar steps after rigorous training. KMC and NNS were performed more uniformly.20,21 Mothers received frequent telephonic reminders, and milk tracing was performed similar to Murphy et al. 10 Various PDSA cycles were conducted and tested. Our results were consistent with other studies.7,10,12,14
The strength of our study is that it is one of the few QI projects reported from India, performed in two phases: a systematic implementation of QI interventions in the first phase; and a continued one on a larger scale adding more evidence-based methods in the second phase. The results showed significant improvement in the usage of MOM in preterm neonates. Second, the study had the baseline pre-QI data as a starting point for comparison. Third, this study was performed with existing resources and manpower (neonatal nurses and available equipment). The nurses were adequately involved in various aspects of maternal counseling, focusing on the importance of MOM. The nursing staff underwent intense training sessions. They closely interacted with parents, attending to concerns of KMC, NNS, and frequent milk expressions. They also encouraged timely milk expressions through telephonic reminders. Our QI can be replicated globally, including resource-limited settings. A limitation of our study was the timing of two phases: there was no time gap between the initiation phase and the continuation phase.
Conclusion
Our QI initiative demonstrated substantial benefits with early expression and provision of MOM. A consistent structured and focused team approach not only ensured adherence to timeliness of MOM availability but also helped in increasing number of preterm babies on MOM through discharge.
Footnotes
Acknowledgments
The authors thank the nursing staff at Rainbow Children's Hospital, Hyderabad, India, who helped in counseling and follow-up of mothers. The authors thank Dr. Kurt O Gilliland, PhD, Cell Biology and Physiology, University of North Carolina, Chapel Hill, NC, for the article review.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.