
Abstract
Introduction:
Breastfeeding (BF) duration remains problematic, especially among women returning to work. Given that use of workplace lactation support programs has not gained traction in improving BF duration, there appears to be elements missing from lactation support initiatives that need further exploration. The field of Implementation Science, in explaining organizational behavior, provides an opportunity to inform a better model for workplace BF support.
Materials and Methods:
To inform a new model for workplace lactation support, data from the Breastfeeding and Employment Study (BESt) were combined with Implementation Climate theory. BESt surveyed companies on their BF supports, and used hierarchical linear modeling to determine the association of those supports with company employee perceptions of and manager attitudes toward BF supports.
Results:
Employee scores were not associated with any company scores. Total company scores were associated with more positive manager attitudes (p < 0.01), due to structural supports, or those supports most visible to managers. Considering these results along with other studies, it is proposed that employees and managers are influenced by tangible (physical) as well as intangible (people) workplace lactation supports. Furthermore, strategies are needed to design and implement approaches to these components to increase workplace lactation support and improve BF durations.
Conclusions:
Implementation strategies will vary with the diversity of workplaces and how they function. A better understanding of the application of implementation climate for workplace lactation support will help tailor programs and their implementation to improve BF duration in employed women.
Introduction
One of the most difficult decisions pregnant women face is whether (and for how long) to breastfeed their infants. 1 Over 80% of U.S. pregnant women initiate breastfeeding (BF), indicating BF promotion has been highly effective. 2 However, BF duration remains problematic with 57.3% and 36.2% of infants born in 2016 being breastfed at 6 and 12 months, respectively. 2
One frequently expressed reason for stopping BF is that women need to return to work, although there is a paucity of data to demonstrate the extent of cessation due specifically to reentry into the workforce.3,4 Data from the Supplemental Nutrition Program for Women, Infants, and Children show that low-income women who return to work breastfeed at lower rates than those not employed. 5 In 2018, 57.8% of all women with an infant under 1 year of age were employed, with 73.7% of these working full-time. 6
Faced with limited maternity leave, working women must either abandon BF, supplement with infant formula, or strategize maintaining a milk supply during the workday. The 2010 Fair Labor Standards Act, Section 7 requires businesses to provide most BF mothers access to a clean private space and time to pump. In 2019, 51% of mid- to large-size companies reported having lactation rooms. 7 A 2017 systematic review of employer-based lactation support programs concluded that provision of space, breaks, and comprehensive lactation support resulted in sustained exclusive BF among nursing working women. 3
In contrast, Hilliard 8 determined that while corporate lactation support was a positive factor in consistently sustaining any BF, lactation spaces and breaks did not. More recently, designation of an Infant Friendly workplace did not demonstrate a difference in BF duration in workplaces in North Dakota. 9 Thus, despite implementation of workplace lactation support programs, many working mothers still face barriers to continued BF. 10
From a business perspective, BF support results in higher productivity, reduced absenteeism, and increased retention among working women. 11 When an employee leaves, company costs are numerous, with direct costs due to separation, replacement, and training along with indirect costs of lost productivity and intangible costs of disturbing the workplace environment. One estimate based on $45K (median 2018 U.S. salary) averages about $15K per lost employee, with higher costs when professional women leave. 12 Additionally, suboptimal BF has been estimated to cost $3 billion annually in maternal and pediatric medical costs. 13
Increasing BF duration of working mothers begins with understanding the workplace environment or “workplace climate,” which is defined as the shared perceptions of, and meaning attached to policies, practices, and procedures employees experience, as well as the behaviors they observe as expected, supported, and rewarded. 14 We previously proposed that the workplace climate could be measured with an instrument based on a model that employees' perceptions of workplace climate would be influenced by their managers' attitudes and workplace lactation supports. 15 Given that use of workplace lactation support programs has not gained traction in improving BF duration, there appears to be elements missing from our model (as well as other lactation support initiatives) that need further exploration.
The field of Implementation Science, in explaining not only individual change but organizational behavior, provides an opportunity to expand upon our original model.16,17 Implementation Science evolved as a research approach to address issues that occur when evidence-based interventions are put into practice. Implementation research aims to improve adoption, appropriate adaptation, delivery, and sustainability of interventions within organizations. In doing so, it has been noted that studies have often not been theory driven, thereby, “restraining opportunities to identify factors that predict the likelihood of implementation success and develop better strategies to achieve more successful implementation.”16(p. 1) One such theory that can be used to understand influences on outcomes from workplace programs is Implementation Climate.
Implementation Climate is defined by Klein and Sorra (p. 1060) as the aggregate of shared perceptions. 18 Thus, while Schneider defined workplace climate as expectations for individual behavior, Klein and Sorra describe implementation climate as the receptivity of all individuals in a targeted group to potential changes in behavior required to support a new intervention. Furthermore, implementation climate is intervention specific 17 whereby different combinations of policies and practices could result in equally positive climates. 16 Rather than separately determining the impact of workplace lactation programs on the working mother or on the manager or coworkers, it is the reciprocity between all entities regarding these programs, as well as their implementation that needs to be investigated.
Employing the underpinnings of Implementation Climate to workplace lactation support programs, we will first discuss findings from a study using our initial model. We then propose a revised Implementation Climate lactation support model that might be used to guide development, pilot testing, and optimization of intervention components. We propose that the components include those which are tangible program supports (e.g., policies and facilities), as well as the intangible supports (people). Variations on these components could be combined and implemented in a manner more suited to individual workplaces and thus increase BF duration among working mothers.
Materials and Methods
The Breastfeeding and Employment Study
Breastfeeding and Employment Study (BESt) was designed to assess the workplace climate for lactation support from the perspective of BF employees, attempting to account for attitudes of their direct managers along with their company's BF supports.
Survey instruments
Three previously validated instruments were used.* The Company instrument assesses workplace supports for BF employees and is designed to be completed by a human resources (HR) manager. The Manager survey assesses manager attitudes to providing employees under their direct supervision with BF support, their beliefs about BF benefits, and their demographics and job characteristics. The Employee survey assesses employee perceptions and includes questions on support from coworkers, direct managers, and the workplace overall, along with access to facilities and time to pump, as well as demographic and job characteristics.
Company supports include a Total Workplace Support scale (range 0–20), with two subscales: Structural Support (composed of Physical Supports and Policy/Climate Support) and Employee Support (composed of Resources and Time/Access). Employee and manager surveys are composed of Likert scale items (1-strongly disagree, 2-disagree, 3-agree, 4-strongly agree).
Recruitment
BESt included companies in three states: the investigators' home state at the time of the study (Michigan), and two states (Oregon and Washington) with high BF rates, to maximize the likelihood of obtaining measurable data. Companies were identified from two business databases, as previously reported. 19 To ensure sufficient sample size, companies with <250 employees were excluded, along with those in industries employing few women (agriculture, mining, construction). 20 Companies were recruited through an invitation postcard addressed to the HR manager identified in the databases at company headquarters. Packets containing questionnaires for the HR manager and employee/direct manager pairs were mailed to 825 companies followed by reminder postcards 1 month later. Questionnaires were returned from May to August 2011.
In addition to reporting their company's lactation supports, HR managers were asked to request up to four female employees who were pregnant or had a baby in the past 2 years, as well as their direct managers, to complete either the employee or manager survey. Postage-paid envelopes were provided for survey return. Respondents could provide a return address for a $25 gift card.
Data analyses
R statistical software 21 was used for all analyses. Hierarchical linear modeling with the lmer package was used to determine the personal and employment-related characteristics associated with employee perceptions and direct manager attitudes, as well as company lactation supports associated with these perceptions and attitudes. We were unable to obtain multiple employees nested under one direct manager; therefore, manager and employee BF outcomes were modeled separately. However, we did examine the relationship between employee perceptions and direct manager attitudes.
Results
Sample description
One-hundred fifty HR Directors, 387 direct managers, and 486 employees returned surveys, representing 180 companies (21.8% response rate). Among company characteristics available, responders did not differ from nonresponders in company size; however, responders were more likely to be from the education industry and less likely to be from health care and service. Most employees were white (89%) while 5% reported being either Hispanic, African American, and/or Asian.
The majority (67%) had a college degree or higher, 96% were married, and 75% were >35 years of age. They had previous or current BF experience (85%) and 64% reported having a female direct manager. Few (5%) worked part time, 21% belonged to a union, 47% were hourly versus salaried, and 50% had worked in their company for >5 years. In general, direct managers were college educated (77%), married (88%), and the majority were female (71%) and white (94%). Over 70% were 40+ years of age, and 68% had at least 15 years of management experience in three or more companies, with 67% supervising 20 people or less. Seventy percent had some experience with a BF employee, and 30% had no personal experience with BF (themselves or a partner).
Findings
Individual company BF supports scales ranged from 3 to 17 in Total Company Support (Table 1). Oregon companies were more likely to have a written policy. Employees reporting greater levels of job autonomy, a better physical environment for BF support, and having female direct managers perceived significantly more lactation support (p < 0.01) (Table 2). There was no association between employee perceptions of support and actual company supports reported by HR managers.
Company (n = 145) Scoring for Breastfeeding Supports
Company scoring: Responses from human resource managers from companies in three states (Michigan, Oregon, and Washington).
Breastfeeding supports: As measured by Hojnacki et al. 19
SEM, standard error of the mean.
Predictors of Employee Perceptions and Manager Attitudes for Breastfeeding Support
For employees—nonsignificant variables are married, education, race/ethnicity, union membership, hourly/salary, and quality of leave (length and pay).
For managers—nonsignificant variables are married, race/ethnicity, education, and being female.
LCI, lower confidence interval; SE, standard error; UCI, upper confidence interval.
Gender, race/ethnicity, and marital status were not significant predictors of positive BF attitudes for direct managers. Managers who reported personal experience with BF (themselves or a partner), or experience with a BF employee, were more likely to have positive attitudes toward BF (Table 2).
Controlling for personal characteristics (demographics, work experience, BF experiences), we analyzed for the types of company supports related to direct manager attitudes (data not shown). Higher levels of Total Company Support were positively associated with better manager attitudes (p < 0.01). However, only Structural Support (and its subscales of Physical and Policy/Climate Support) was positively associated with more positive direct manager attitudes (p < 0.01). Associations between employee perceptions and direct manager attitudes, in total or subscores, were not significant.
Discussion
For BF employees in this study, some tangible lactation supports (e.g., space to pump or support groups) appear less important to their perceptions of lactation support than their work situations, whereas stronger manager attitudes were associated with tangible (and more visible) lactation supports. We found that managers' attitudes toward lactation support were associated with having previous BF experience, either personal or with an employee; however, we did not see an association between direct manager attitudes and employee perceptions for lactation support.
This disconnect suggests a weak implementation climate. When the implementation climate for a program is weak, personal values and individual work situations drive employee behavior, including both employees using the program and those employees (coworkers and direct managers) who must assist anyone needing the supports. 17 In our study, it is possible managers were unaware of factors hindering their employees' use of these supports, for example, lactation rooms. In such a climate, BF employees may rely on help from employees in their immediate workplace environment to use supports, rather than on a company policy.
Similarly, recent work supports the existence of this disconnect between tangible and intangible factors influencing workplace lactation support on extending duration of BF. Studies continue to demonstrate that employees do not believe they can use lactation supports, perceiving a lack of support from coworkers.10,22 Employees felt that pumping led to unfavorable breastfeeding stigma from coworkers, while at the same time, acknowledging some coworkers were supportive (“breastfeeding compassion”). 23 A qualitative study of a well-resourced hospital employee lactation support program concluded that “a woman's personal experience may be both positive and challenging depending on her individual work culture and environment.”24(p. 693) Both BF and non-BF working mothers from childcare centers noted that their perception of workplace support for lactation was positively associated with perception of managerial support. 4
Researchers conducting focus groups of business representatives found that although workplaces may have BF programs, their implementation often rests at the level of direct managers, who are influenced by intangible factors affecting interpersonal communication, such as gender and power dynamics. 22 Mothers and managers in a rural community identified themes that also suggest issues with workplace climate, whereby policies or facilities for lactation support existed, but may not be communicated proactively by managers to those who may need them. 25 Women, in turn, hesitated to ask for accommodations because they did not want to disturb the workplace. 25 Elsewhere, women reported quality pumping space as a significant influence to combining BF and work; however, they also reported they were discouraged from using supports (e.g., inadequate break time for pumping) or there was ridicule from managers and coworkers. 23 Discouragement by coworkers was found even when only female coworkers were considered. 22
Research on the use of family-friendly workplace programs in general shows similar categories of facilitators and barriers as that found in the lactation support literature, including manager and coworker support, workflow, and stigma attached to use of supports. 26 For example, a greater amount of maternity leave for exclusive BF benefited only those women reporting their workplace as unsupportive. 27 Moreover, use of lactation supports may be even more problematic given that communication involves the word “breast” (which some may find uncomfortable), especially if communication occurs between female employees and male managers. 28
Since the creation of federal policy for workplace lactation support, it is clear that increased BF duration among employed mothers remains elusive. It is likely that inconsistencies in implementation of lactation supports both across and within organizations result in limited success. To move the field forward, research is needed to understand the climate for lactation support, so that programs can be both developed and implemented suited to individual workplace environments.
The BESt study did have limitations. Companies responding may have had better lactation support policies than nonresponders, and HR managers may have given surveys to employees they felt would respond positively. There was a lack of diversity among employees and managers, which may be due to self-selection bias, or the mailings to larger company headquarters. This limits generalization to populations that may require more help to combine BF and employment. However, even with these limitations, we did not find many associations of attitudes or perceptions with lactation support. This reinforces the likelihood for the need to improve support for all employees, and warrants a closer examination of workplace lactation support.
A new model of workplace lactation support
As noted, lactation support implementation climate is influenced not only by physical (tangible) supports, but also by the quality and accessibility of these supports. We propose this climate also has an intangible or people (i.e., managers and coworkers) component that may encourage or discourage use of supports. We have selected strategies 22 that may improve implementation for lactation support through impact on the intangible component, and through improvement in the ability of employees to access and fully use the tangible supports (Figure 1).
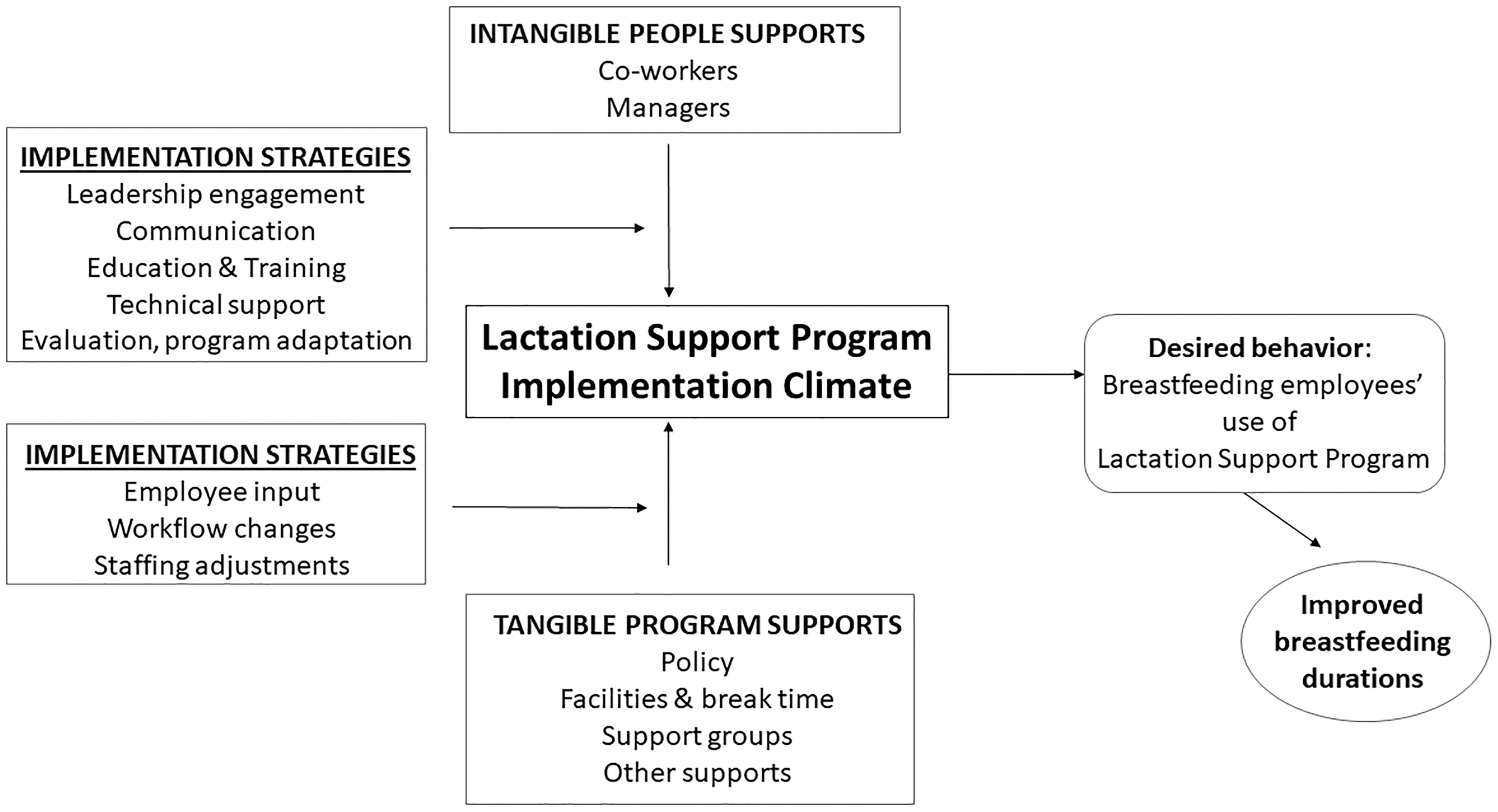
A new model of workplace lactation support.
Lactation support overlays the business environment with a health intervention that some employees and managers note involves an embarrassing and sensitive topic. Ensuring that workplace lactation efforts move forward may require strong company leadership on the importance of such support to the company, the education of all employees, and persuasive and ongoing communication. Until the workplace climate for lactation support is entrenched, follow-up and evaluation must be maintained.
Development of tangible supports must involve all workplace employees, but focus on those most immediately involved (pregnant and lactating women, their direct managers, and HR). Rojjanasrira et al. found that manager attitudes toward supporting employees to breastfeed improved following implementation of a lactation support program tailored to address manager concerns. 29 Employees note use of pumping facilities, inaccessible by either distance or time, may be improved by changes in workflow and staffing. 10 Research is needed to determine if other relevant implementation strategies are missing from this model.
Conclusion
Implementation strategies will vary with the diversity of workplaces and how they function. A better understanding of the application of implementation climate for workplace lactation support will help tailor programs and their implementation to improve BF duration in employed women.
Footnotes
Acknowledgments
The BESt results were presented at Experimental Biology 2013, Boston, MA.
Disclosure Statement
M.S.-G. serves as a consultant to The Pennsylvania State University, Cornell University, Nemours, and the Robert Wood Johnson Healthy Eating Research Program. No competing financial interests exist for the remaining authors.
Funding Information
USDA NRI 2006-35215-16703.