
Abstract
Introduction:
Sexual problems have significant effects on individual sexual function. The aim of this study was to determine the effect of counseling on sexual function of lactating women with decreased sexual desire.
Methods:
This is a quasi-case research. The sample consisted of 104 lactating mothers with sexual desire disorder from 2 to 6 months after childbirth. Samples were randomly selected and divided into two control and case groups. Data were collected using questionnaires, including the decreased sexual desire scale, sociodemographic characteristics, and midwifery questionnaire, and female sexual function index (FSFI). Sexual function was measured before and 4 weeks after consultation based on the rapport building, exploration, decision making, and implementing the decision (REDI) model. The results were analyzed by using SPSS-24 software and a significant level of <5%.
Results:
The mean age of participants was 30.71 ± 6.23 years and 29.65 ± 5.66 years in the case and control group, respectively (p = 0.380), ∼50% had a diploma degree or more, 100% were living in urban areas, and 95.90% of women were housewives. Both case and control groups were homogeneous in terms of demographic and midwifery variables (p > 0.05). There was a highly significant difference between study and control groups regarding mean FSFI domains except for orgasm, as well as in the total FSFI score 4 weeks after the intervention (p < 0.001). The results of the linear mixed effects model for assessing the trend of mean total FSFI score present that the mean of total FSFI score in the case group was increased 2.26 in comparison with the control group. Estimated slopes for female indicate that the mean of total FSFI score was increased 3.44 for 1 month.
Conclusions:
The results of this study show that supporting lactating women with decreased sexual desire through sexual counseling based on the REDI model can make a significant difference in their sexual function.
Introduction
Female sexual dysfunction (FSD) is a common disorder that includes decreased sexual desire, reduced sexual arousal, painful intercourse, and difficulty in achieving orgasm. 1 Based on studies, 30–60% of women have experienced sexual dysfunction at least once in their lives. 2 In a study by Khajehei et al., approximately two-thirds of women (64.3%) experienced sexual dysfunction in the first year after delivery, the most common sexual disorders reported by women were sexual desire disorder (81.2%), orgasmic problems (53.5%), and sexual arousal disorder (52.3%). 3 Lactating women may be at greater risk for sexual dysfunction,4,5 breastfeeding exposes women to a number of physiological and psychological factors that can negatively affect their sexual function. 6 Breastfeeding increases plasma prolactin concentration that reduces the level of sex hormones. The reduction of estrogen leads to vaginal dryness, dyspareunia, and sexual desire disorders during lactation. 7 McDonald et al. (2015) reported that loss of sexual interest is the most common sexual health problem in the first 3 months postpartum. 8
Sexual dysfunction has many negative consequences including the improper relationship between spouses, mental diseases, divorce, and even sexual crimes, especially in family and social. 9 The main cause of many sexual disorders is the lack of sexual knowledge, sexual misconceptions, or couple inability to express their sexual interests. 10
According to studies, treatment options for FSD have many adverse effects. 11 A variety of approaches, including counseling, may be beneficial in treating FSD. 12 Counseling is a process that strengthens skills and empowers people to improve their health. 13
Counseling is done in different ways, the rapport building, exploration, decision making, and implementing the decision (REDI) framework provides a structure and guidance for talking with clients. 14
The majority of sexual dysfunction can be effectively treated by using counseling. This study aimed to determine the effectiveness of sexual health counseling program based on the REDI model on the sexual function of lactating women with decreased sexual desire 2 to 6 months after delivery.
Materials and Methods
This randomized controlled trial study with a pre- and post-test design was carried out between November 2018 and May 2019. The study was approved by the Iranian Registry of Clinical Trials (IRCT20120215009014N247), and the institutional review board of the University of Hamadan Medical Sciences of Iran.
Participants
This study was conducted on 104 women referred to comprehensive health centers of Sonqor city of Kermanshah provinance of Iran. The inclusion criteria included exclusive breastfeeding, 2 to 6 months postpartum, absence of complications during pregnancy and childbirth, decreased sexual desire based on decreased sexual desire scale (DSDS), no exposure to stressful events during pregnancy and after childbirth, living with the spouse, absence of mental and physical illness, as well as drug and alcohol addiction, ability to speak, read and write in Persian language, and to be available during the study.
Exclusion criteria were pregnancy, illness, or hospitalization of the infant, separation from the spouse, more than one absence in the counseling session, and finally optional exit from the study. Medical records were used to verify the informations.
Sampling method
Sampling was done first by using the available sampling method of all health centers of Sonqor city, including five centers, then with a randomized block design, subjects were divided into case and control groups. The sequence of allocation with four blocks and six different sequences was determined by removing the card and replacing it with 26 times, according to which 52 people were assigned to the control group and 52 people were in the case group. A trained midwife selected the participants and the researcher trained them.
For selecting 104 lactating women with low sexual desire and other inclusion criteria, 363 subjects were examined, in addition to preventing communicating with each other; with the cooperation of the centers, the care of the control and the case groups was adjusted to different odd/even days.
First, a total of 104 lactating women with sexual dysfunction and inclusion criteria were selected, 3 people in the case group were absent for more than 1 session and were excluded from the study, in the control group 3 people withdrew from the study and finally, 98 individuals were evaluated (Fig. 1).
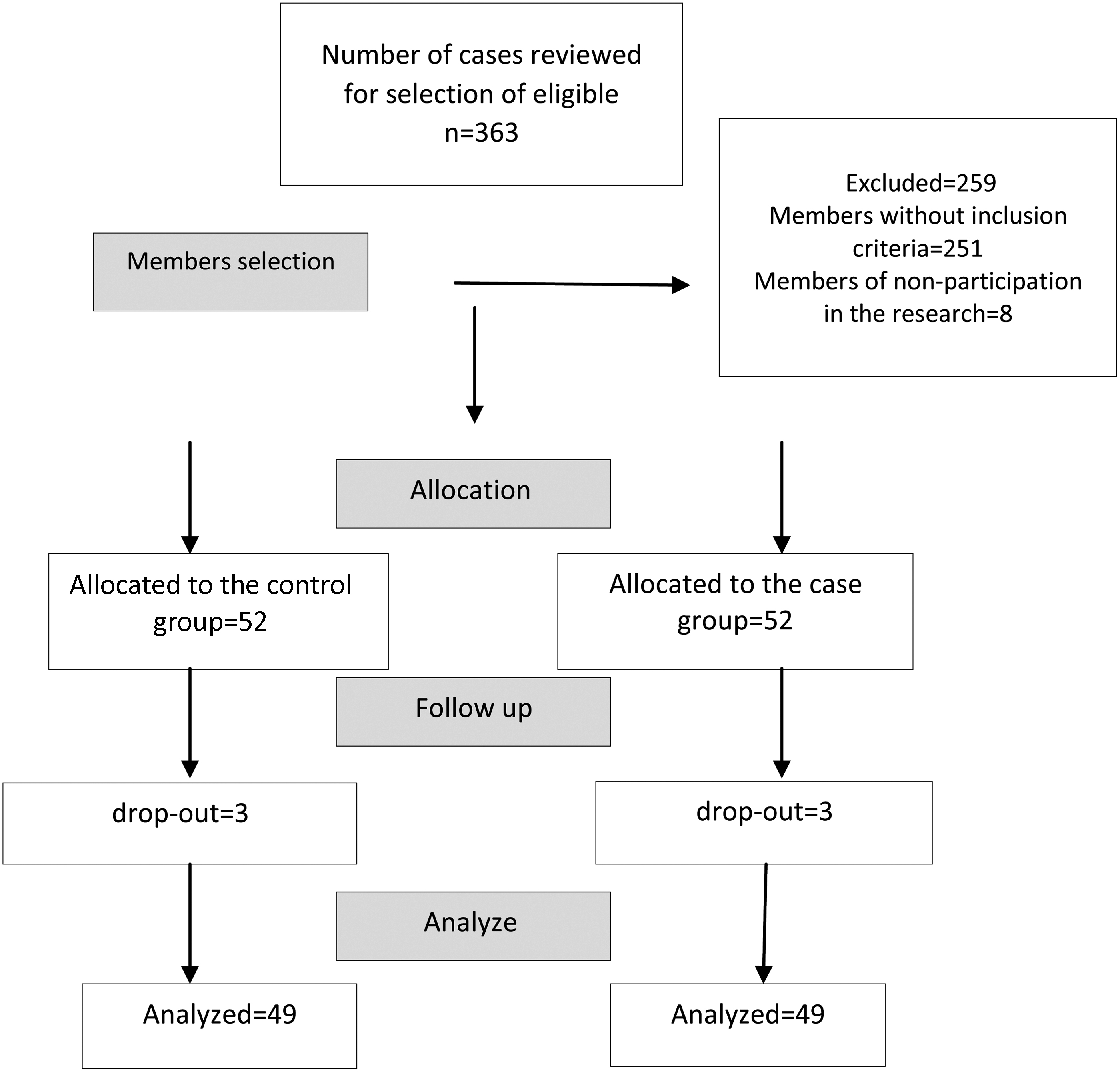
Selection of research participants.
Intervention
Counseling sessions comprised four sessions, one session a week for 45–90 minutes based on the REDI model; the researcher conducted these sessions for the case group on the health centers. The content of group counseling sessions for the case group is presented in Table 1. During the counseling sessions, the following issues were discussed.
Content of Counseling Sessions
Postpartum maternal health care and child care, genital anatomy, and physiology were taught using anatomical models and figures, the women's cycle of sexual responses, biological, psychological, and social factors influencing sexual issues during breastfeeding, effective communication skills and intimacy, postpartum maternal health care and child care, mental skills to improve sexual arousal, strategies to reduce life stress, including exercise, meditation, and other mind/body techniques, optimizing sleep and other interventions to reduce fatigue, improving communication, specific exercises to improve intimacy and mutual pleasure, sensual massage, different sexual positions, and mental skills to improve sexual arousal.
Four weeks after the counseling sessions, the female sexual function index (FSFI) questionnaire was completed again in case and control groups. The control group received the educational package including CD and educational pamphlets on postpartum sexual problems at the end of the study.
To determine the sample size, the article of Hezbian et al. 15 was used, sample size was obtained using α = 0.05, β = 0.20, and 10% loss of research samples based on the comparison of two independent groups formula. From 104 participants, 52 were assigned to each of the case and control groups using block randomization.
Data collection tools
Demographic and midwifery questionnaire, DSDS, and the standard questionnaire of the FSFI were used for data collection. The DSDS is a qualitative questionnaire with five questions, four first questions are “yes/no” and the fifth question is a multipoint question if the woman answers the first four questions as “yes”; the clinician should diagnose decreased sexual desire. 16 The validity and reliability of this questionnaire were confirmed in 2013 by Clayton et al. 0.85. 17 The validity of this questionnaire was confirmed by Boojarzadeh et al. in Iran. 18
The FSFI is a 19-item questionnaire that measures female sexual performance in six domains, including desire, arousal, lubrication, sexual pleasure, sexual satisfaction, and painful intercourse. The total score of the individual is the sum of each domain score; higher scores indicate better sexual function. Based on the maximum score of 6 for each domain, the total score of each sample can be 36. A score <28 indicates an impaired sexual function. The validity and reliability of this questionnaire have been confirmed in various studies. Based on Rosen's study, the reliability of the questionnaire was 0.79 to 0.86. 19 Wiegel et al. reported its reliability as 0.89. 20 The validity and reliability of the FSFI questionnaire in Iranian society were also assessed by Mohammadi et al., the Cronbach's alpha coefficient was 0.70. 21
Data collection method
Counseling was provided in the form of the REDI model, in four weekly sessions 45 to 90 minutes in groups of six people between November 2018 and May 2019.
Statistical analysis
Descriptive and inferential statistics were used for data analysis. Independent groups were compared using a paired t test and Mann–Whitney test. Paired t test and Wilcoxon post-test were used to compare the score of each group before and after the intervention and linear mixed effects model. A p-value of <0.05 was considered a statistically significant difference.
Ethical Considerations
This master thesis was approved by the Ethics Committee of Hamadan University of Medical Sciences (Ref. no: 1R.UMSHA.REC1397.482). Also, the participants were informed about the study objectives and ensured the confidentiality of their information, and written consent was taken from them in the native language (Persian) before the study.
Results
The mean age of participants was 30.71 ± 6.23 years and 29.65 ± 5.66 years in the case and control groups, respectively (p = 0.380), the mean of infant age of participants was 4.26 ± 1.22 months and 4.12 ± 1.61 months in the case and control groups, respectively (p = 0.613), ∼50% had a diploma degree or university education, 100% of participnts were living in urban areas, and 95.90% of women were housewives. Both case and control groups were homogeneous in terms of demographic and midwifery variables (p > 0.05) (Table 1).
According to Table 2, both case and control groups were similar in terms of the frequency distribution of the DSDS questions of the questionnaire and had no statistically significant differences (p > 0.05).
Comparison of Demographic and Midwifery Variables of Case and Control Groups
Chi-square test.
Fisher's exact test.
Significance level.
The results of this study indicated that there was no statistically significant difference between mean scores of total sexual function and its domains between the two groups before intervention (p < 0.05), but significant difference between the two groups was observed after the intervention (p < 0.05). In the case group, the mean total score of sexual function and its domains increased and showed a statistically significant difference after intervention (p < 0.05). In the control group, only the orgasm domain showed a statistically significant increase after the intervention (p = 0.043), and the difference before and after the intervention in other domains was not statistically significant (p < 0.05) (Table 3).
Comparison of Frequency of Decreased Sexual Desire Scale Questionnaire Items Between Case and Control Groups Before the Intervention
Chi-square test.
Fisher's exact test.
The result in Table 4 presents that the mean of total FSFI score and libido in the case group were increased 2.26 and 0.24 in comparison with patients in the control group. Estimated slopes for female indicate that the mean of total FSFI score and libido were increased 3.44 and 0.54 during 1 month, respectively. Also, estimated variances of random terms show that there were fluctuations among patients change (slope) before and after the intervention in case and control groups Table 5.
Comparison of Sexual Function Between Case and Control Groups Before and After the Intervention
Significance level.
Wilcoxon test.
Paired t test.
Mann–Whitney U test.
FSFI, female sexual function index.
Results of Linear Mixed Effects Model for Assessing the Trend of Mean Total Female Sexual Function Index Score and Libido According to Group
Could not be computed.
Discussion
This study was a clinical trial with the aim of determining the effect of counseling based on the REDI model on sexual function of lactating women with decreased sexual desire. In this study, all lactating women in both case and control groups had decreased desire according to the results of DSDS, they reported that stress, fatigue, and pain during intercourse were the main cause of their sexual desire disorder. Olsson et al. showed that postpartum changes are caused by the change of sexual activity patterns, fatigue, and lack of time for sexual activity due to the presence of infants and altered body image, therefore, couples are more affected by stress. 22 Other studies have also referred to breastfeeding as an effective factor in sexual desire.23,24 In the Schlagintwei et al. study, the majority of participants were concerned about having different levels of sexual desire than their partner after the arrival of the baby. 25
The World Health Organization recommended that education and counseling on sexual life in postpartum care are identified as one of the women's needs. 26 After 4 sessions of intervention based on the REDI model, the mean score of libido was increased in the case group compared to the control group; this indicated the effectiveness of the intervention, which is consistent with another study. 27
The current study findings illustrated that there were highly statistically significant differences regarding mean of total scores of FSFI, libido, sexual arousal, vaginal discharge, sexual satisfaction, and pain before and after the consultation training based on the REDI model between case and control groups. Results of the linear mixed-effects model present that the mean of total FSFI score in the case group was increased 2.26 in comparison with the control group. Estimated slopes indicated that the mean of total FSFI score was increased 3.44 for 1 month.
In the Iranian society, talking about sexual issues are taboo 27 ; it appears that counseling sessions by increasing women's awareness of sexual dysfunction, anatomy, and physiology of the genital system, misconceptions about sexual life during breastfeeding, and infant nursing care plans have been effective in improving women's sexual function.
No similar study was found in line with assessing the effect of group counseling based on REDI model on sexual function of lactating women; however, researchers have investigated the effect of permission, limited information, specific suggestions, intensive therapy (PLISSIT) model counseling on sexual function and reported that it has a positive effect on sexual function.28–31 Contrary to the results of this study, Yörük et al. reported that intervention did not have an impact on reducing postpartum women's sexual problems. 32
Based on the research finding, there was no statistically significant difference between the two groups in orgasm, its score increased in both groups. Some researchers reported that breastfeeding stimulates sexuality, some women reported contractions similar to orgasm during breastfeeding.33,34
Limitations of this study included women's concerns about child care during counseling sessions and lack of counseling with participants' spouses.
Conclusions
The results of this study show that supporting lactating women with decreased sexual desire through sexual counseling based on the REDI model can make a statistically significant difference in their sexual function and improve it.
Footnotes
Acknowledgments
The authors thank all pregnant women who participated in this study and the staff of Hamadan University of Medical Sciences and Sonqor City Health Centers, who provided research conditions.
Authors' Contributions
All authors equally contributed to the design of the research, wrote the article, and approved the article for publication.
Disclosure Statement
No potential conflict of interest was reported by the authors. This article is the result of a master's degree thesis in midwifery of Hamadan University of Medical Sciences; the authors are faculty members and are affiliated with this organization.
Funding Information
The authors would like to appreciate the Vice-chancellor of Research and Technology, Hamadan University of Medical Sciences, Iran, for financial support of the study (research ID: 9708225070).