
Abstract
Introduction:
Late preterm infants (LPIs) are at greater risk for short- and long-term morbidity compared with term infants. However, little is known about whether breastfeeding can reduce the adverse effect of late preterm (LP) birth on various diseases. Therefore, we examined the association of LP birth with the risk of hospitalizations from 6 to 18 months of age, then explored the possible modification of this effect by breastfeeding.
Materials and Methods:
Data were extracted from a nationwide population-based longitudinal survey in Japan. We restricted our analysis to term and LPIs with information on hospitalization (n = 31,578). Multivariate adjusted odds ratios (aORs) and 95% confidence intervals (CIs) were estimated to evaluate the association between LP birth and hospitalization using term birth as the reference. We then examined whether breastfeeding status modified the potential adverse effects of LP birth on each health outcome.
Results:
LPIs were more likely to be hospitalized for all-cause (aOR, 1.58; 95% CI, 1.35–1.86), respiratory (aOR, 1.52; 95% CI, 1.21–1.92) and gastrointestinal infections (aOR, 1.73; 95% CI, 1.14–2.62) than term infants. While LPIs had a higher risk of hospitalization for all-cause and respiratory infection regardless of breastfeeding status, we did not observe an increased risk of hospitalization for gastrointestinal infection among the exclusively breastfed LPIs, in contrast with increased risk among the non-exclusively breastfed LPIs.
Conclusions:
We found that LPIs had a higher risk of all-cause and cause-specific hospitalization compared with term infants. Moreover, exclusive breastfeeding probably reduced the adverse effect of LP birth on gastrointestinal infection.
Introduction
Late preterm infants (LPIs) are defined as infants born between, and including, the gestational ages of 34 weeks and 0 days and 36 weeks and 6 days. 1 This population is known to be at greater risk of morbidity than term infants, such as respiratory complications, temperature instability, hypoglycemia, hyperbilirubinemia, feeding problems, and neonatal intensive care unit admissions in the neonatal period.1,2 Some studies also found that late preterm (LP) births are associated with long-term health and neurodevelopmental sequelae in childhood.3–5 Indeed, several studies demonstrated the increased risk of adverse health outcomes including hospitalization among both preterm and LPIs after the neonatal period,6,7 however, few studies examined the cause-specific morbidity of LPIs during early infancy. 8
Meanwhile, there is strong evidence that breastfeeding protects against a variety of diseases and conditions in both term and preterm infants, such as respiratory infection, diarrhea, otitis media, necrotizing enterocolitis, childhood overweight and obesity, diabetes, sudden infant death syndrome, and developmental delay.9,10 However, most previous studies related to the beneficial effects of breastfeeding for preterm infants have mainly focused on the outcome of very preterm and extremely preterm infants. Thus, it remains unclear whether breastfeeding can reduce the adverse effect of LP birth on various diseases.
In this study, we therefore investigated the risk of all-cause and cause-specific hospitalization, such as respiratory and gastrointestinal infections, from 6 to 18 months between term and LPIs, using data from a nationwide longitudinal survey in Japan. Then, we further examined whether breastfeeding could modify the potential adverse effects of LP birth on cause-specific morbidity.
Methods
Study participants
The Japanese Ministry of Health, Labour and Welfare has conducted an annual survey among newborn babies and their parents, known as the Longitudinal Survey of Babies in the 21st Century, since 2010. 11 In brief, baseline questionnaires were distributed to all families throughout the country with 6-month-old infants born between the 10th and 24th of May, 2010. Follow-up questionnaires were sent to all participants who initially responded annually (at 18, 30, and 42 months, etc.). Of the 43,767 mailed questionnaires, 38,554 were completed and returned (response rate, 88.1%). Birth records were also linked to each child included in this survey. We excluded children without information on gestational week (n = 7) and children born before 34 weeks and 0 days (n = 443) and after 41 weeks and 6 days (n = 127) to focus on comparing the results between term and LPIs. The remaining 37,977 children were eligible for this study.
In this study, we used data from the initial survey for the baseline and from the second survey for the health outcomes because the respondents were asked about their past history of hospitalization between 6 and 18 months of age. Of the initial respondents, 6,399 infants were lost to follow-up at the second survey. Thus, we analyzed the remaining 31,578 infants for their health outcomes (30,237 term infants and 1,341 LPIs) (Fig. 1).
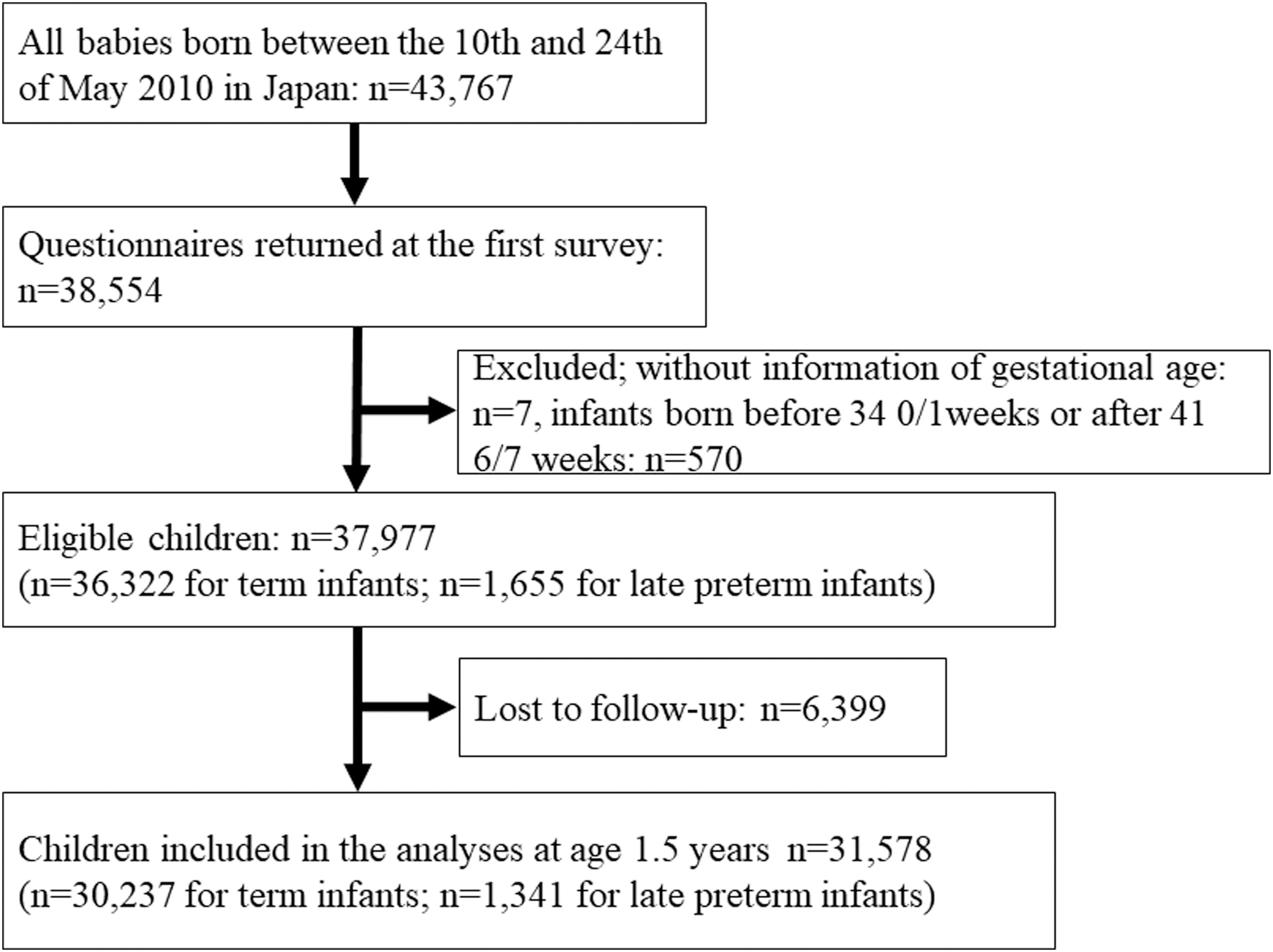
Flowchart of participants.
Gestational age and feeding status
We determined each infant's gestational age from their birth records and categorized them into two groups based on gestation duration: that is, 37–41 weeks, term infants; 34–36 weeks, LPIs. In Japan, gestational ages are routinely estimated by the date of the onset of the mother's last menstrual period and then corrected by the first trimester ultrasound in almost all pregnancy cases. 12
We also ascertained the infants' feeding status according to the first survey, which included questions on infant-feeding practices to specify whether the children had been breastfed, only colostrum-fed, or formula-fed. We created “exclusive breastfeeding,” “partial breastfeeding, “feeding colostrum only” and “formula feeding” categories using information on breast- and formula feeding. We categorized “exclusive breastfeeding” when parents answered that they had breastfed their babies and never formula-fed, “partial breastfeeding” when parents had breastfed and formula-fed, “colostrum only” when they had given only colostrum and formula-fed, and “formula fed” when they had formula-fed and never-breastfed. Although we used the term of “exclusively breastfeeding,” it might not be the same one defined by World Health Organization 13 in some cases because the questionnaire did not query whether the babies were provided other foods or liquids. There were 230 cases with missing information about infant-feeding practices.
Health outcomes
As health outcomes, we used the infants' past history of one or more overnight hospitalizations between 6 and 18 months of age. In this survey, “overnight hospitalization” means whether infants had been hospitalized during the previous 12 months for any reason. The questionnaires included 29 or more causes of hospitalization, such as infectious and allergic diseases, injuries, among others (e.g., bronchial asthma, food allergy, fracture, central nervous system diseases and congenital diseases). We selected three descriptions of hospitalization due to “all cause,” “respiratory infection (common cold, pharyngitis, adenoiditis, bronchitis, and pneumonia),” and “gastrointestinal infection (gastrointestinal diseases including enteritis, diarrhea, vomiting, and so on)” because respiratory and gastrointestinal infections are the most frequently observed causes for hospitalization in children aged under 5 years in Japan. 14 Unfortunately, we could not identify the duration or frequency of hospitalization and severity of illness from the questionnaire data.
Statistical analyses
We compared the baseline characteristics of eligible term and LPIs. We also compared the demographic characteristics of infants who were analyzed, but lost to follow-up. We then calculated the proportion of hospitalization for all causes, and respiratory and gastrointestinal infections between 6 and 18 months of age separated by feeding practices (i.e., exclusive or partial breastfeeding and formula feeding) to identify how feeding practices affected hospitalization.
To investigate the associations between LP birth and the hospitalization between 6 and 18 months of age, we used logistic regression models and estimated odds ratios (ORs) and 95% confidence intervals (CIs) for each outcome using the “term infants” as the reference category. We first estimated the crude ORs and 95% CIs for each outcome (Model 1). We then estimated the ORs and 95% CIs for each outcome after adjusting for the infant factors (Model 2) and for both infant and parental factors (Model 3) based on previous studies and clinical relevance. 6 The infant factors included sex (dichotomous), singleton or not (dichotomous), parity (dichotomous: 0 versus ≥1 birth), and daycare attendance (dichotomous). Parental factors included maternal age at delivery (continuous), maternal and paternal smoking habits (dichotomous: 0 versus ≥1 birth), and maternal educational attainment (categorical). The data for infants' sex, singleton or not, gestational week, parity, and maternal age at delivery were listed in their birth records. The maternal smoking status was ascertained at the first survey (when the infant was 6 months old). The maternal and paternal educational attainment were obtained from the second survey (when the infant was 18 months old) and classified into three categories: less than or equal to high school; junior college (2 years) or vocational school; and university (4 years) or higher. We excluded missing and incomplete cases in the analyses.
To evaluate how breastfeeding could modify the potential adverse effects of LP birth on each health outcome, we created four new categories by combining birth status with breastfeeding status: that is, term infants with exclusive breastfeeding; term infants with nonexclusive breastfeeding; LPIs with exclusive breastfeeding; and LPIs with nonexclusive breastfeeding. We evaluated the association between the new categories and hospitalization using “term infants with exclusive breastfeeding” as the reference category. We estimated the ORs and 95% CIs adjusting for the same set of confounding variables.
Furthermore, we conducted sensitivity analysis to remove possible residual confounding due to health status of infants, 15 so we excluded infants who had been hospitalized or visited doctors for congenital diseases between ages 6 and 18 months and repeated the same analyses.
All analyses were performed using Stata statistical software (Stata SE, version 16; Stata, College Station, TX). This study was approved by the Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences Institutional Review Board (No. 1506-073).
Results
The baseline characteristics of the eligible infants separated by term and LPIs are summarized in Table 1. LPIs tended to be male, multiple births, and have mothers who smoked and had lower educational attainment compared with term infants. Compared with term infants, the proportion of breastfed infants is lower in the LPIs, especially exclusively breastfed infants (34.2% versus 19.8%). Infants who were lost to follow-up at the second survey were more likely to attend daycare, formula-fed, and have parents who smoked (Supplementary Table S1).
Demographic Characteristics of Eligible Term and Late Preterm Infants (n = 37,977)
There were 5,105 cases missing in daycare attendance, 109 cases missing in maternal smoking, 254 cases missing in SGA, 405 cases missing in LGA, 5,156 cases missing in maternal educational attainment, 896 cases missing in paternal smoking, and 331 cases missing in infant-feeding practices (317 in term infants and 14 in late preterm infants).
SGA: birth weight is <10th percentile for gestational age, LGA: birth weight is more than 90th percentile for gestational age.
Obtained from the birth record.
Obtained from the first survey (at the age of 6 months).
Obtained from the second survey (at the age of 18 months).
SD, standard deviation; SGA, small for gestational age; LGA, large for gestational age.
Table 2 presents the proportion of hospitalization between 6 and 18 months of age as separated by infant feeding practices. Among all hospitalization categories, exclusively breastfed infants tended to have lower proportions of hospitalizations.
Proportion of Hospitalizations Between Six and Eighteen Months Separated by Feeding Methods in All Infants (n = 31,348)
There were 230 cases missing in infant-feeding practices.
The ORs and 95% CIs for association between LP birth and history of hospitalization between 6 and 18 months of age are presented in Table 3. LPIs were more likely to be hospitalized between 6 and 18 months even after controlling for potentially confounding variables. The adjusted ORs using Model 3 for hospitalization were 1.58 (95% CI: 1.35–1.86) for all-cause hospitalization, 1.52 (95% CI: 1.21–1.92) for respiratory infection, and 1.73 (95% CI: 1.14–2.62) for gastrointestinal infection.
Unadjusted Odds Ratios and Adjusted Odds Ratios with 95% Confidence Intervals for the Associations Between Late Preterm Birth and Hospitalization During This Period (n = 31,578)
Crude model.
Adjusted for infant factors (e.g., sex, singleton birth or not, parity, daycare attendance).
Adjusted for infant factors (e.g., sex, singleton birth or not, parity, daycare attendance) and parental factors (e.g., maternal age at delivery, maternal and paternal smoking status, maternal educational attainment).
CI, confidence interval; OR, odds ratio; aOR, adjusted odds ratio.
When we used the combined categories for LP birth and breastfeeding status (Table 4), LPIs had a higher risk of hospitalization for all causes and respiratory infection regardless of breastfeeding status. Although the effect estimates for gastrointestinal infection had wide confidence intervals due to small number of cases, exclusively breastfed LPIs did not have elevated risk for the hospitalization.
Adjusted Odds Ratios with 95% Confidence Intervals for the Associations Between Combined Late Preterm Birth and Feeding Status and Hospitalization Between Six and Eighteen Months (n = 31,348)
Adjusted for infant factors (e.g., sex, singleton birth or not, parity, daycare attendance) and parental factors (e.g., maternal age at delivery, maternal and paternal smoking status, maternal educational attainment).
CI, confidence interval; aOR, adjusted odds ratio.
In the sensitivity analysis, the exclusion of infants with congenital diseases did not alter the main findings substantially (Supplementary Tables S2 and S3).
Discussion
In this study, we compared the risk of all-cause and cause-specific hospitalization, such as respiratory and gastrointestinal infections between 6- and 18-month-old term and LPIs, and examined whether breastfeeding could modify the potential adverse effects of LP birth using data from a large nation-wide longitudinal study in Japan. We found that LPIs had a higher risk of all-cause and cause-specific hospitalization than did term infants, but breastfeeding seemed to reduce the adverse effect of LPIs on gastrointestinal infection.
LPIs had a higher risk of all-cause hospitalization compared with term infants, which was consistent with previous studies.6,7,16 Moreover, LPIs had a higher risk of cause-specific hospitalizations, such as respiratory and gastrointestinal infections in the postneonatal period, which is partly consistent with a previous meta-analysis that showed an increased risk for several cause-specific hospitalizations including respiratory problems among LPIs. 8 However, this study highlighted the increased risk of gastrointestinal infection among LPIs, which was not reported in previous studies. This possible mechanism could be related to the infants' immature physical and physiological development, such as their immune system and the development of various organs. For example, fetal lungs and intestines develop rapidly during the third trimester of pregnancy17,18 and would not be well developed in LPIs.
As expected, exclusively breastfed infants (including both term and LPIs) were likely to have lower proportions of hospitalizations (Table 2), which was consistent with previous studies, even those in high-income countries. 19 However, it should be mentioned that this was a crude analysis and we did not consider potential confounders such as gestational age or health status of infants.
Moreover, despite the wide confidence intervals, exclusively breastfed LPIs did not have a higher risk of hospitalization on gastrointestinal infection compared with breastfed term infants, in contrast with increased risk among nonexclusively breastfed LPIs (Table 4). In other words, breastfeeding tended to reduce the adverse effect of LPIs on gastrointestinal infection. This finding is plausible because breast milk contains bioactive components combined with nutritional, anti-infective, anti-inflammatory, antioxidative, epigenetic, and gut-colonizing substances, which are particularly important for vulnerable infants, such as preterm and LPIs. 9 However, it should be noted that we only had three cases of hospitalization due to gastrointestinal infection among exclusively breastfed LPIs. By contrast, exclusively breasted LPIs had higher ORs for hospitalizations of all-cause and respiratory infection than nonexclusively breastfed LPIs (Table 4). This might show that breastfeeding does not have prolonged beneficial effects on respiratory infections among LPIs. However, further investigation is necessary to elucidate those findings.
The main strength of this study is that we used a large nationally representative cohort of children in Japan. The response rate of the baseline survey was high (88.1%) and we had a high follow-up rate (83.2%) at the second survey. We could also extensively adjust for potential confounders from child and parental factors. The breastfeeding information was also accurate because the parents were asked about feeding practices at their infant's age of 6–7 months and almost all parents keep a record of breastfeeding on the Maternal and Child Health Handbook, which is distributed under the Japanese law. 20 Moreover, because most patients are readily accessible to primary and tertiary medical facilities under the health insurance system in Japan, the information on hospitalization was also accurate.
By contrast, this study has several limitations. First, several participants were lost to follow-up; infants who were lost to follow-up at the second survey were more likely to be LP, attend daycare, be formula-fed, and have parents who smoked (Supplementary Table S1). This differential loss could underestimate the adverse effects of LP birth on hospitalization. Second, residual confounding factors may be a concern because we do not have information on pregnancy complications, maternal comorbidities (e.g., caesarean section, gestational diabetes), and health status of infants (e.g., past history of neonatal intensive care unit admission, mechanical ventilation, surfactant therapy, and antirespiratory syncytial virus monoclonal antibody administration or rotavirus vaccination). These factors may partly explain the increased risk of LPIs on cause-specific morbidity, but the results did not change substantially even after excluding infants with congenital diseases. Third, there is a possible misclassification on breastfeeding information because of recall bias, especially among mothers who stopped breastfeeding shortly after birth, and social pressure, by which some mothers may have reported longer breastfeeding duration. Finally, there was a low number of exclusively formula-fed infants in Japan (Table 1), so it is difficult to investigate how breastfeeding affects health outcomes compared with infants who were never breastfed (i.e., formula-fed only).
In addition to the higher risk of morbidity among LPIs observed in the present study, LP births comprise a large percentage of preterm births in many countries (e.g., ∼80% in Japan in 2015),16,21 which leads to a large public health burden and sizable health service costs due to LP births.8,22 Therefore, some public health or medical actions should be conducted to mitigate this problem. One of the actions could be a population-level increase in breastfeeding among LPIs. Because it would be more difficult to establish breastfeeding for LPIs compared with term infants due to their immaturity and higher proportion of multiple births (Table 1),23,24 additional breastfeeding support for LPIs and their mothers are necessary not only for their optimal growth and development, but also for the public interest.8,25
In conclusion, this study revealed that LPIs had higher risk of all-cause and cause-specific hospitalization, such as respiratory and gastrointestinal infection, compared with term infants in a nationally representative longitudinal study in Japan. Moreover, exclusive breastfeeding probably reduced the adverse effect of LP birth on gastrointestinal infection; thus, breastfeeding should be recommended for LPIs and their mothers and the support for establishing breastfeeding is crucial.
Footnotes
Disclaimer
The sponsor was not involved in the study design, collection, analysis, or interpretation of the data, writing of the report, or decision to submit the article for publication.
Acknowledgments
We appreciate the valuable comments provided by Dr. Hiroyuki Doi. We also appreciate the valuable support of Saori Irie in collecting the data.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was partly supported by a Grant for Strategies for Efficient Operation of the University (#2007030201).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.