
Abstract
Objective:
To investigate the association, in the United Kingdom, between having an episiotomy during childbirth and giving human milk by any modality as an infant's first feed. We also identified maternal demographic factors and perinatal experiences associated with increased chance of the infant's first feed being human milk.
Study Design:
Retrospective observational cohort study at two large maternity units within district general hospitals in the United Kingdom.
Population:
Mothers giving birth vaginally to singleton babies at ≥34 weeks and ≥1,800 g.
Methods and Main Outcome Measures:
Deidentified data from hospital records were analyzed. The odds ratio (OR) of a mother giving human milk for an infant's first feed after episiotomy versus no episiotomy was calculated using a chi-squared test. Logistic regression was used to investigate and then control for confounders known to affect breastfeeding.
Results:
A total of 13,906 women met the inclusion criteria (2,113 had had an episiotomy and 11,793 had not). Human milk was given as a first feed to 70% of infants in the study population. Women whose infants received their first feed as human milk were on average older, had lower body mass index, lived in an area of less socioeconomic deprivation, and had fewer previous births than those women who gave formula milk as the first feed to their infant. The occurrence of an episiotomy during delivery was not associated with a change in the odds of the infant receiving human milk for the first feed (OR: 1.12 [confidence interval, CI: 0.96–1.38]). Where a woman had skin-to-skin care with her infant straight after birth, the infant was more likely to receive human milk as a first feed (OR: 4.23 [CI: 3.59–4.98]).
Conclusion:
There is no link between episiotomy during delivery and the odds of a woman giving human milk as the first feed to her infant.
Introduction
The United Kingdom has one of the lowest rates of breastfeeding in Europe: only 81% of women initiate any breastfeeding, 1 and the rate of babies receiving any human milk falls to 34% by 6 months. 2 Babies who are initially breastfed are more likely to continue breastfeeding, while those who receive a prelacteal feed are less likely to receive human milk subsequently. 3 A wide range of sociodemographic and psychosocial covariates affect the rate of successful breastfeeding. 4 Factors that inhibit mothers from initiating and continuing breastfeeding include a lack of support/guidance, postnatal depression, lower levels of educational attainment, and perception of the birth as a traumatic experience. 5
An episiotomy (a surgical incision to widen the vaginal introitus and aid delivery) is perceived by many women as a traumatic procedure. Episiotomies are usually carried out to allow more space for delivery during complex births and to reduce the occurrence of obstetric anal sphincter injury that can complicate 2.8% of births. 6 Incidence of episiotomies in vaginal deliveries of singleton infants to nulliparous women in the United Kingdom is around 22%. 7 The rationale for their restricted use in clinical practice is that the procedure can have adverse maternal consequences, including increased pain after childbirth (with an increase in analgesic requirement), bleeding, scarring, dyspareunia, wound infection, and fistula formation. 8 These complications may have a negative impact on breastfeeding. 9 Initiation of breastfeeding could also be affected by fetal distress, which is the most common reason for birth to be expedited with an episiotomy.
The effect of a woman having had an episiotomy on breastfeeding is not well known. A 2017 Cochrane systematic review of selective versus routine use of episiotomy found that no data had been recorded for the outcome of breastfeeding initiation or continuation. We aimed to study the association between women having an episiotomy during birth and the likelihood of their babies receiving human milk as a first feed. We also looked at how maternal demographic factors and perinatal experiences affect this association.
Methods
Aims
This study investigated whether there is an association between a woman having an episiotomy at delivery and the chance that the first feed given to her baby will be human milk as opposed to formula milk. As donor milk is not used at either study site, human milk was assumed to have been maternal in origin.
Study design
This was a retrospective observational study using deidentified data from digital health care records at the maternity departments of two U.K. National Health Service district general hospitals in the East Midlands. Site 1, Royal Derby Hospital, has ∼6,000 births per year. It has a midwife-led birthing unit of 4 beds and a consultant-led unit of 17 beds. Derby Neonatal Unit cares for babies over 26 weeks of gestation. Births at other sites that were registered at Derby Hospital were also included. Site 2, King's Mill Hospital in Mansfield, has over 3,000 births per year, and also has facilities for both midwife-led and consultant-led care. Their neonatal unit cares for babies from 26 weeks and 6 days of gestation.
Data collection
Women were only included in the study if they had a vaginal birth as this is the only route of delivery in which episiotomy is used. All women who delivered infants vaginally at ≥34 weeks of gestation and ≥1,800 g birthweight were included. These criteria were applied because infants outside of these limits would be routinely admitted to the neonatal intensive care unit (NICU) and this could influence the type of first feed. Mothers whose babies were taken into care were excluded where possible as this could affect mother/infant bonding and the type of first feed received by the infant.
Sample size calculation
In England, 74% of infants receive human milk as their first feed. 7 Of the total number of women who had babies during the study period, we anticipated that ∼26% would be excluded as they had a cesarean section. 7 Assuming that a mother having had an episiotomy would reduce the chance of the infant receiving human milk as the first feed by 5%, we required a total of 6,198 women to adequately power the study. Ideally, this would include 1,033 women with an episiotomy and 5,165 women who did not have an episiotomy.
The two hospitals included in this study together have about 9,000 births per year, 85% of which are ≥34 weeks of gestation. Approximately a quarter of these would be cesarean section and assuming 10% noncollection of primary outcome data, we found that data collected between May 7, 2016, and July 27, 2018, were sufficient to achieve the required sample size.
Data analysis
Data were accessed from the electronic clinical records held at the maternity units. The following data were recorded: mother's age, parity, presence of skin-to-skin contact, ethnicity, body mass index (BMI) (available for Site 2 only), and index of deprivation (used as a measure of socioeconomic status). All data were deidentified before analysis. The women's postcodes were converted into the Index of Multiple Deprivation using the resource available at http://imd-by-postcode.opendatacommunities.org/.
Women who had had an episiotomy were compared with women who had not had an episiotomy. A chi-squared test was used to compare the percentage of women whose babies received human milk as their first feed between groups. Logistic regression was applied to control for maternal factors known to influence breastfeeding (skin-to-skin contact, index of deprivation, parity, and BMI). These factors were included due to differences between groups of women who did and did not have an episiotomy, as given in Table 1, and also due to clinical relevance.
Demographics of Women in the Study
1 = most deprived; 10 = least deprived.
BMI, body mass index; IMD, index of multiple deprivation; SD, standard deviation.
Main outcome measures
The primary outcome was first feed being human milk (given by any modality) as opposed to formula milk.
Results
Data were collected for women who delivered between May 2016 and July 2018. These data included a total of 13,906 women, of whom 2,113 had an episiotomy and 11,793 did not (Fig. 1). Data on the women's BMIs were available from Site 2 only. The demographic characteristics of women included in the study are shown in Table 1.
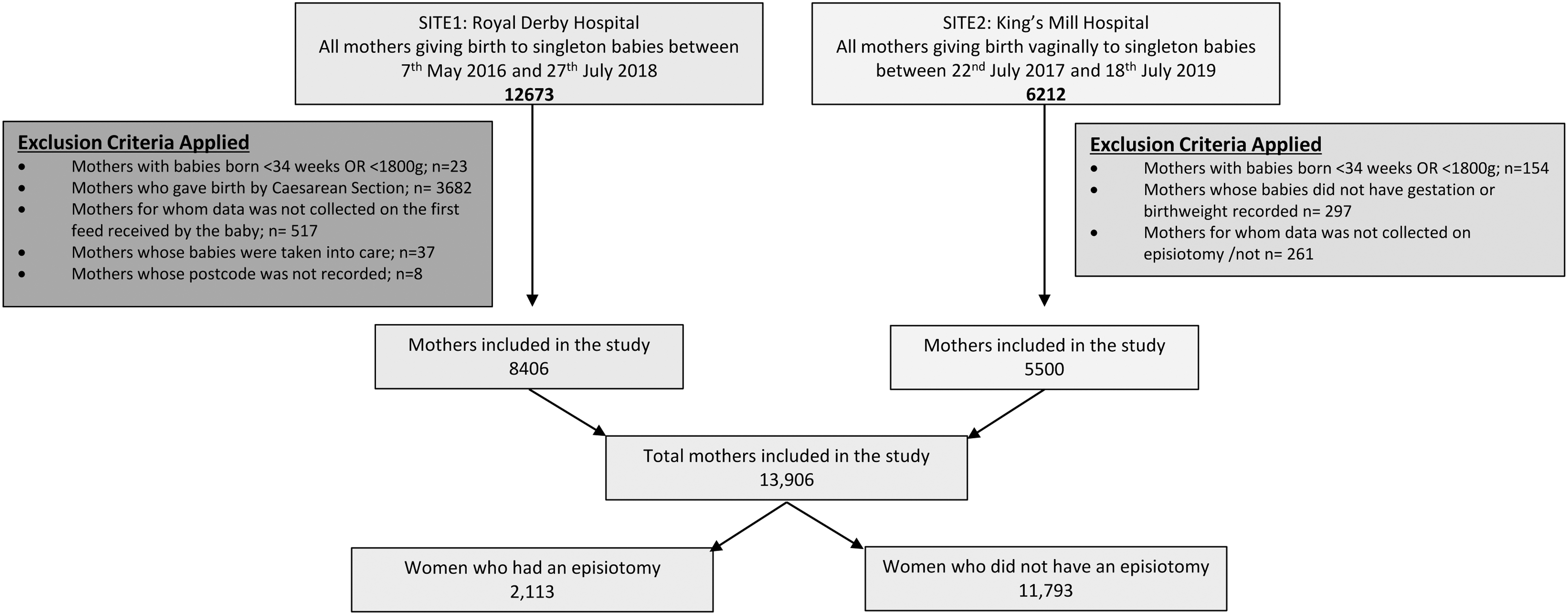
Mother/infant pairs included in the study. OR, odds ratio.
Association between receiving an episiotomy and giving human milk as first feed
Of the 2,113 women who had an episiotomy, 1,597 (75.8%) gave human milk to their baby as the first feed; of the 11,793 women who did not have an episiotomy, 8,076 (68.5%) gave human milk to their baby as the first feed (Table 2). The odds ratio (OR) (95% confidence interval [CI]) of an infant receiving human milk as the first feed if the women had an episiotomy during delivery was 1.42 (1.28, 1.58). However, after adjusting results for skin-to-skin care immediately after birth, maternal BMI (where data were available), primiparity, and maternal index of deprivation, the corrected OR was not statistically significant (OR: 1.12 [CI: 0.91–1.37]) (Table 3).
The Relationship Between a Mother Having an Episiotomy During Delivery with the Type of First Feed Given to the Neonate
Given by any modality.
A Logistic Regression Model with First Feed of Human Milk As the Outcome and Occurrence of Episiotomy As the Exposure Corrected for Skin-to-Skin, Maternal Body Mass Index, Being a Primigravida, and Index of Deprivation
CI, confidence interval; OR, odds ratio.
Maternal demographic factors associated with giving human milk as first feed
Statistically, the babies who received human milk as first feed were more mature and heavier at birth compared with those that did not receive human milk as first feed. These differences were small and unlikely to be of clinical significance. Women who gave their first feed as human milk were on average older, of a lower BMI, from a higher socioeconomic group, and had fewer previous births than those women who gave their first feed as formula milk (Table 6).
Among the 12,718 women who had skin-to-skin care with their infant immediately after birth, 9,211 (72.4%) gave human milk as the first feed; meanwhile, among the 703 women who did not have skin-to-skin care with their infant immediately after birth, 265 (37.8%) gave human milk as the first feed (Table 4). The OR of a baby receiving human milk as first feed if the mother and baby had skin-to-skin care immediately after birth was 4.34 (3.71, 5.08). After including episiotomy, primiparity, maternal age, maternal BMI, and infant's birthweight in the model, this OR was changed to 4.23 (CI: 3.59–4.98) and remained statistically significant (Table 5).
The Relationship Between a Mother Having Immediate Skin-to-Skin Care with Her Newborn and the Type of First Feed Given to the Neonate
Given by any modality.
A Logistic Regression Model with First Feed of Human Milk As the Outcome and Immediate Skin-to-Skin Care As the Exposure Corrected for Episiotomy, Mother Being a Primigravida, Maternal Age, and Infant Birthweight
Association Between First Feed As Human Milk Given by Any Modality and Maternal Demographics
Discussion
Statement of principal findings
We found that there is no association between a woman having an episiotomy and the likelihood of her baby receiving human milk for the first feed. In the included population, the chance of an infant receiving human milk was 70%, which is considerably lower than the 81% rate of breastfeeding initiation reported in the U.K.-wide Infant Feeding Survey. 7
Strengths and weaknesses of the study
The main strength of this study is the use of contemporaneously recorded recent data obtained from electronic clinical records. The data are representative of the U.K. population as all eligible women who delivered in the two hospitals are included in the study. Information was available on several maternal and infant characteristics allowing for consideration of a number of covariates of the relationship between episiotomy and initiation of breastfeeding. In particular, the index of multiple deprivation allowed for inclusion of socioeconomic status, which is known to have a strong influence of both initiation and continuation of breastfeeding.
Data were not available for some potentially important factors that affect the chances of a women giving human milk as first feed such as antenatal class attendance, intention to breastfeed, and availability of breastfeeding support.5,10 We assumed that all participants would have had access to similar services within the NHS and some potential variations may have been accounted for by including the index of multiple deprivation in the analysis. We have commented above on the importance of skin-to-skin care; however, accurate data on the duration of time spent skin-to-skin were also not available for this study.
There are mixed reports on a possible link between methods of analgesia and breastfeeding initiation. For example, it has been stated that women who receive pethidine in the delivery room could then become too sleepy to initiate breastfeeding.11,12 Wetzl et al. found that women who more distinctly prioritized pain relief during delivery were less likely to breastfeed their infants. 13 Reassuringly, Xu et al. found no association between a women having an epidural and a change in the prevalence of breastfeeding. 14 We did not have the data to investigate the effect of analgesic use in our analysis.
Data on BMI were available only for women who delivered at Site 2. More complete information on maternal BMI may have allowed the demonstration of a stronger relationship with breastfeeding initiation.
We excluded infants who would have required NICU admission as per birthweight and gestational age criteria (<34 weeks and <1,800 g). As admission to NICU data was not available in the database, we were unable to exclude the mature and heavier infants who may have been admitted to the NICU for other reasons.
Comparison with previous studies
A Malaysian study published in 1997 showed that there was no association between women receiving an episiotomy and exclusive breastfeeding at 6 weeks, 15 which is in keeping with our findings of no association in the first feed being human milk.
A recent Norwegian study investigated the association between breastfeeding and maternal factors, including socioeconomic status and BMI. In that study, babies of more highly educated mothers had higher odds of being breastfed than those whose mothers had received a shorter duration of education, and babies of overweight/obese mothers had reduced odds of both being breastfed at all and being exclusively breastfed when compared with mothers with normal BMI. 16 Davie et al. 17 agreed that initiation of breastfeeding is affected by maternal BMI. Our study also supported these findings: among our population, the mean (standard deviation) BMI of women whose babies received human milk as a first feed was 26.3 (6.0) compared with 27.5 (6.8) in women whose babies did not receive human milk for their first feed. We also found that women who had an episiotomy on average weighed less than women who did not have an episiotomy. Women with a larger BMI are known to be less likely to sustain perineal trauma during delivery.18,19 Any effect of having an episiotomy on initiation of breastfeeding is likely to be confounded by maternal BMI, and we found that in a model including both having an episiotomy and maternal BMI, there was no association between having an episiotomy and initiation of breastfeeding.
Early skin-to-skin care has many benefits, including increased initiation and continuation of breastfeeding.20,21 Sharma, for example, found that breastfeeding was established on average after around 50 minutes of skin-to skin time. 22 Our findings also highlight the crucial importance of immediate skin-to-skin care between mother and infant in increasing the chance of successful initiation of breastfeeding.
Meaning of the study: unanswered questions and future research
We found, reassuringly, that having an episiotomy does not adversely affect the odds of the first feed being human milk. In our study population, the breastfeeding initiation rate was lower than the national average. We found that women whose babies did not receive human milk as a first feed were typically from areas of higher socioeconomic deprivation, which could represent a health inequality for these infants. Our findings suggest that providing the opportunity for skin-to-skin care is an essential component of promoting breastfeeding. Further research is required to find optimal evidence-based approaches to delivering such interventions and providing adequate antenatal, perinatal, and postnatal support for breastfeeding mothers and babies.
Conclusion
There is no association between a woman having an episiotomy during delivery and the likelihood that her baby will receive human milk as the first feed. Infants who received skin-to-skin care immediately after birth were significantly more likely to receive human milk as their first feed with an OR of 4.23 (CI: 3.59–4.98).
Footnotes
Acknowledgments
The authors would like to thank the staff at both the Royal Derby Hospital and King's Mill Hospital for their support with data collection. They would also like to acknowledge statistician Andrea Venn (University of Nottingham) for her advice regarding the sample size selection and methods of statistical analysis.
Authors' Contributions
J.S., S.O., and J.A. came up with the concept and study design. J.S. was then responsible for data collection. Statistical analysis was performed by J.S. and S.O. with the initial discussion and conclusion being written by J.S., S.O., and K.W. All authors contributed to drafting and proofreading the article.
Ethics Approval
IRAS/HRA: IRAS Project ID 240543. R + D approval: DHRD/2018/060
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.