
Abstract
Background:
The pasteurization is a mandatory step to inactivate pathogenic microorganisms of bank milk. For storage, freezing and thawing are necessary. The concentration of macronutrients and energy of bank milk could be influenced by these procedures which are routinely used in human milk bank.
Research Aim:
The aim of this study is to analyze the effect of bank milk processing (pasteurization and freezing/thawing) on the macronutrients (fat, protein, and carbohydrate) concentration and energy content.
Materials and Methods:
The samples of donor milk were collected and studied before/after pasteurization and after frozen for 3 months. Total 100 samples of bank milk were tested using an infrared analyzer. The measurements of fat, protein, carbohydrate, and energy were statistically analyzed by SPSS.
Results:
There was a prominent reduction of fat mean concentration following pasteurization and frozen (20.5% and 6.5%, respectively). The processing did not cause significant changes in protein content, but there were significant increase after pasteurization and decrease after frozen in carbohydrate (p < 0.05). Overall (postpasteurization and frozen storage), a 9.6% decrease was observed for energy content.
Conclusion:
This study revealed that the processing of bank milk (including Holder Pasteurization and frozen storage) decreased fat and energy content of human milk significantly, and this could not meet the specific needs of preterm infants.
Introduction
To protect the recipients against disease transmission, the safety of bank milk is based on strict protocols of donor screening and milk handling processes. Every recruiting donor would complete the detailed questionnaire, including the survey of life styles, medical condition, recent medication, risk behaviors for infection, and the perinatal history of her own baby. The serological screening with sexually transmitted disease (HIV, HTLV, and RPR for syphilis) and hepatitis (HAV, HBV, and HCV) should be all negative for eligible donors. The bank milk processes vary among countries or milk banks. Since establishment in December 2004, the Taipei City Hospital Milk Bank (TCHMB) had followed the practice guidelines of the Human Milk Banking Association of North America (HMBANA) and United Kingdom Association for Milk Banking (UKAMB). The donor milk is Holder Pasteurized at 62.5°C for 30 minutes before distribution, whereas some donor milk is distributed unpasteurized in other countries. 1
In the past 15 years, TCHMB kept providing bank milk to the premature babies or other high-risk infants with severe illness nationwide in Taiwan. The frozen human milk shipped to milk bank was processed via thawing, pooling, dispatch, pasteurization, and freezing again. Bacterial culture of raw milk was done to exclude possible pathological species to immunocompromised recipients, and the pasteurized milk should be germ-free. The average pass rate of donor milk in TCHMB is around 75–85%. Until now, neither adverse effect nor documented disease transmission had been reported from recipients after consuming bank milk.
The safety of bank milk is guaranteed by pasteurization and bacterial culturing. But multiple processing procedures, like repeated frozen and thawing, and pasteurization can also affect the nutrients in breast milk. The human milk is a bioactive body fluid with dynamic change in composition. The nutritional and non-nutritional part of human milk may be different from colostrum to late lactation, from foremilk to hindmilk within expression, and between mothers. With recent evidence from a systemic review demonstrating that milk processing has variable effect on the nutrients and biological components of bank milk, 2 it is important to understand the nutritional differences and energy gap of bank milk, which may have a critical impact on the recipient's growth and health. Therefore in this study, we aimed to investigate the effect of pasteurization and freezing on fat, lactose, and protein concentration in donor milk from TCHMB.
Materials and Methods
The study was approved by the Institutional Review Board of Taipei City Hospital. Since 2016 June, the eligible donors of TCHMB were invited to join the study. The informed consent was obtained from all participants. Total 100 donors were recruited, and the milk samples were collected from their donation to TCHMB. Frozen donor milk from participants was processed and screened following the protocols. After thawing, pooling, and dispatch of individual milk, 10 mL of milk samples (sample A) were reserved before pasteurization. After pasteurization (62.5°C for 30 minutes), 10 mL of milk samples (sample B) were obtained from the bottle indicated for bacterial culture. Then the indicated bottle was stored with frozen status in a −20°C freezer for 3 months. After thawing, 10 mL of milk was got as sample C (Fig. 1). Each sample was analyzed with infrared analyzer (MIRIS HMA, Uppsala, Sweden). The descriptive data for macronutrients and energy are recorded as the means and standard deviations (mean ± SDs). The results were also compared throughout each step of the process using paired t-tests. A value of p < 0.05 was considered significant.
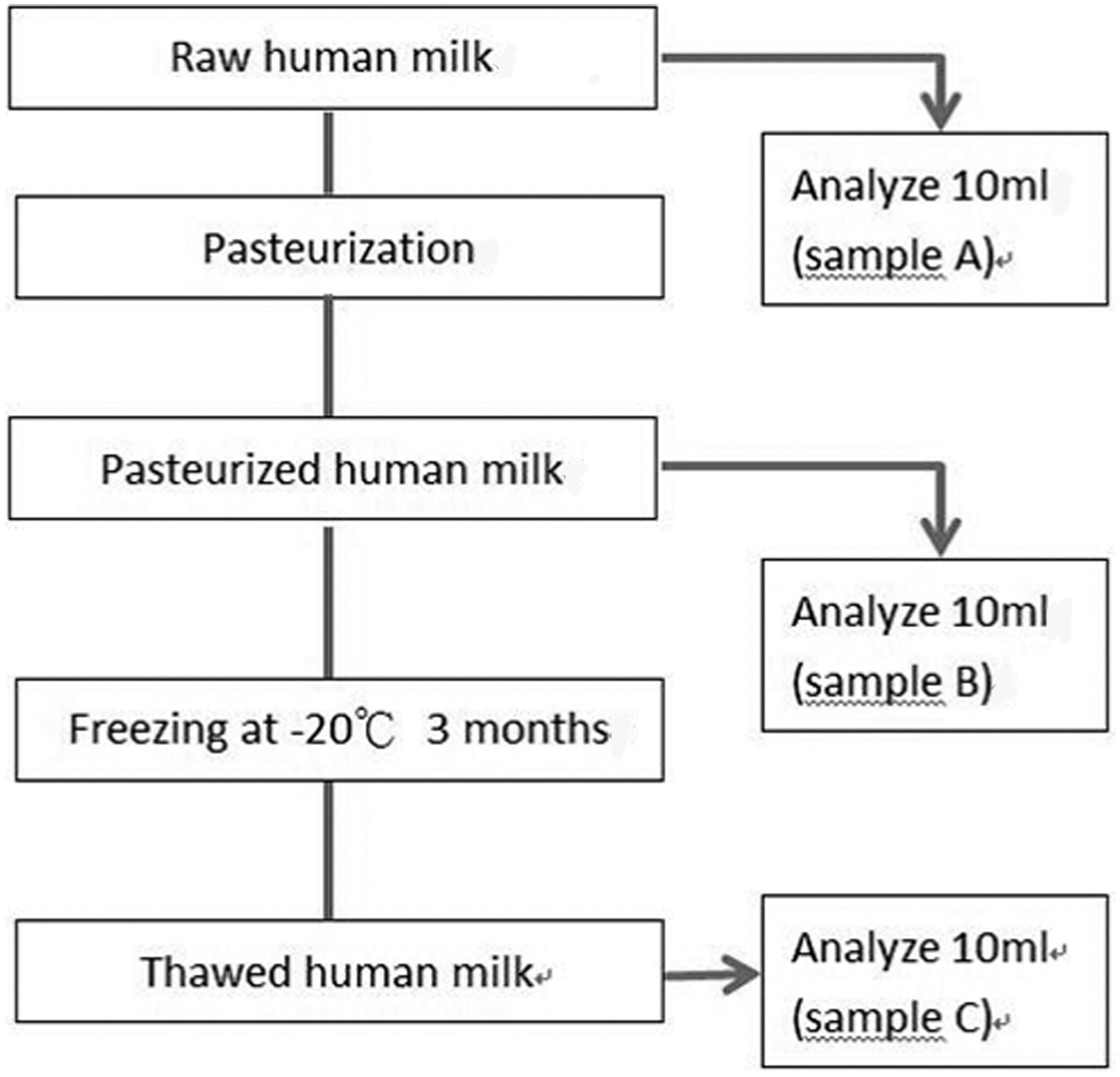
Description of the study design.
Results
The mean age of donors was 31.7 years (SD 4.0, range 22.3–41.5). The mean donation time was 2.5 ± 1.5 months after delivery (range 0.1–6.7 months).
Concentration of macronutrients and energy before pasteurization
The mean values of the initial samples (before pasteurization) are revealed in Figure 2. Of the total 100 samples of raw donor milk, 69% (n = 69) had a fat content <3.5 g/dL, whereas 72% had an energy content <67 kcal/dL. The protein content was <0.9 g/dL in 19%, between 0.9 and 1.2 g/dL in 61% of samples, and >1.2 g/dL in 20% of samples. The carbohydrate concentration was <6.7 g/dL in 34% of samples.
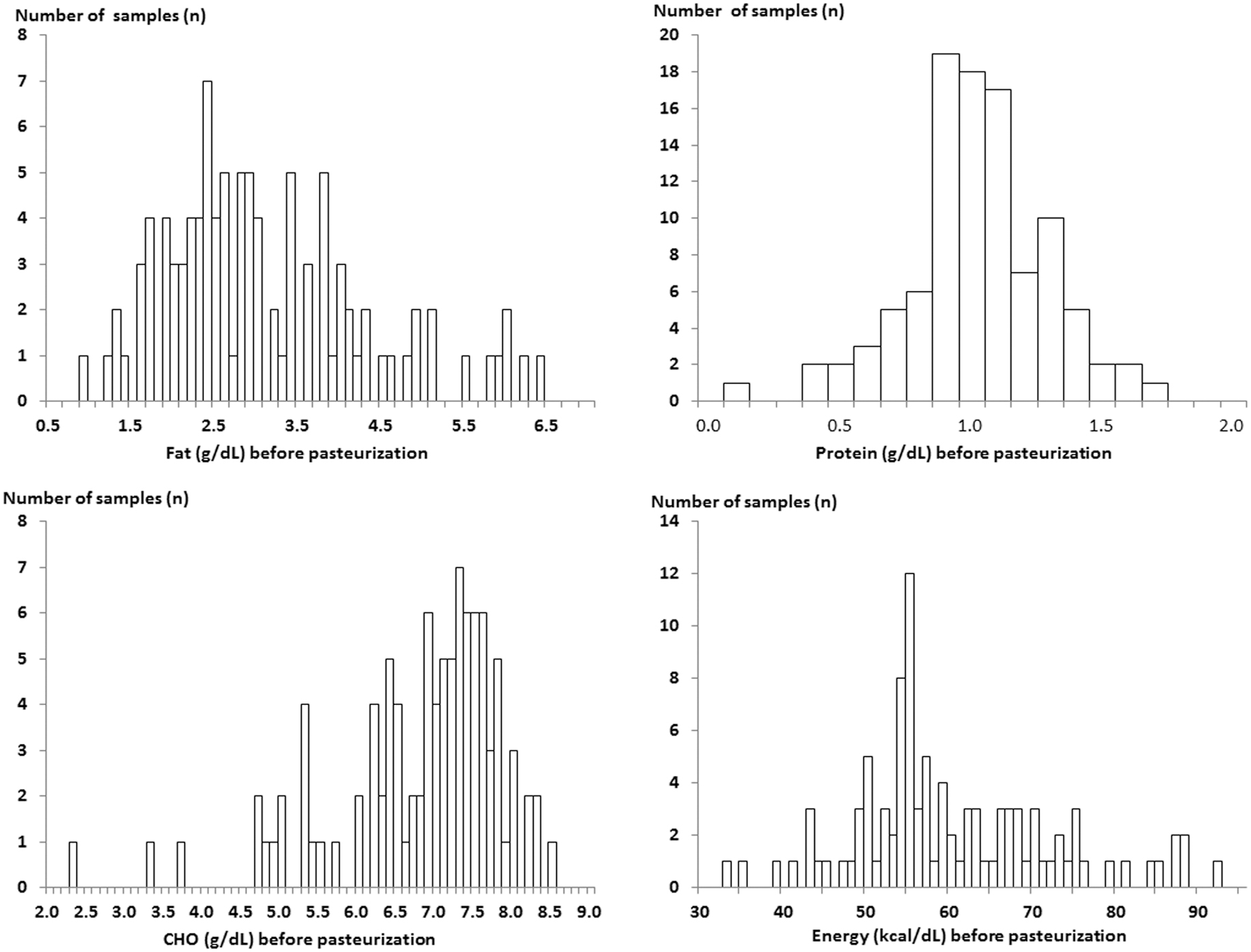
Variable distribution of macronutrients and energy in raw milk samples.
Effect of milk processing with pasteurization and freezing
Mean (±SD) values for fat, protein, carbohydrate, and energy content of raw donor milk (n = 100), postpasteurized milk (n = 100), and postfrozen pasteurized milk (n = 100) are shown in Table 1. The most variable macronutrient concentration in the analyzed samples was fat (0.9–6.4 g/dL).
Fat, Protein, Carbohydrate, and Energy Concentrations of Raw Donor Milk, Postpasteurized Milk, and Postfrozen Pasteurized Milk
p < 0.05 for raw milk versus pasteurized milk or frozen milk.
p < 0.05 for pasteurized milk versus frozen milk.
SD, standard deviation.
There was a prominent reduction of fat mean concentration following pasteurization and freezing (20.5% and 6.5%, respectively, p < 0.05). The processing did not cause significant changes on protein content. However, there were significant increase after pasteurization and decrease after freezing in carbohydrate (p < 0.05). Overall (postpasteurization and frozen storage), a 9.6% decrease was observed for energy content.
Discussion
Bank milk is now recognized as a good source of nutrition for infants whose mother's milk is not sufficient or available. Especially for the premature babies, it can reduce the incidence of necrotizing enteritis with the same effect of own mother's milk.3–7 However, the gap of nutrition and energy between the bank milk and the high nutritional requirements of prematurity cannot be ignored. The quantity and quality of nutrient of bank milk can be influenced by two main factors: the characteristics of the milk donors and the effect of milk processing. Some nutrients may depend on variations in donor's diet. In a single donor, the composition of human milk may vary throughout the course of lactation, diurnally, or even within one expression. In TCHMB, most milk donors are mothers with full-term delivery, and breast milk expressed at 2–4 months postpartum is usually surplus enough for donation. 8
For all macronutrients, the concentration of fat in breast milk is most variable between subjects.9–12 Before processing, the total fat content of donor milk measured with infrared analyzers revealed 3.08 ± 1.23 g/dL in average (range 0.9–6.4 g/dL), which seemed slightly lower than the reference data of 3.5 g/dL from expressed fresh mature human milk, 13 but more close to the lipid level (3.22 ± 1.0 g/dL) of 415 samples from 273 donors on previous study. 12 The main consideration is that the lipid component will decrease gradually with the lactation time. The other concern is that the donor's surplus expressed milk was frequently stored frozen in bags, causing fat component attachment and lost during milk pooling procedures.
The protein of human milk, composing of α-lactalbumin, casein, lactoferrin, secretory immunoglobulin IgA, and some enzyme, is crucial for infant growth and immunologic maturity. From colostrum, transitional milk to mature milk, the protein concentration decreases in human milk gradually and reaches the steady level around 0.9 to 1.2 g/dL. 13 The protein content of human milk from bank donors mostly with term delivery is much less than the mothers who deliver preterm. 14 The mean protein value for pooled donor milk from our data was around 1.02 g/dL, which was also slightly lower than the data from previous study. 12
Lactose, the main component of carbohydrate in human milk, contributes a readily usable energy source. Similar to protein, little variability existed and the data support previously published typical mature milk lactose levels of about 6.7 g/dL. 13 The value was slightly lower than the previous studies of bank milk with more cases, which reveals 7.8% in Wojcik's study (415 samples) 12 and 7.19 g/dL in Piemontese's study (460 samples). 15
Effect of pasteurization
The previous review study had showed that Holder Pasteurization had some effect on macronutrients and biologically active components in donor human milk. 2 But still some discordance of results existed, probably due to different sampling or variable test protocols applied in studies. Besides, some previous studies may use older pasteurizers, requiring longer for processing milk. The latest studies in recent 10 years (2009–2019) concerning about the pasteurization effect on macronutrients (fat, protein, lactose/carbohydrate) of breast milk were searched in PubMed and reviewed. The results are compared with our study in Table 2.
The Effect of Pasteurization on Macronutrients Concentration
Most studies showed significant reduction of fat components after pasteurization, ranging from 3.5% to 25%.15–21 Our study revealed that fat concentration of donor milk decreased significantly to 2.45 ± 0.75 g/dL (range 1.0–5.5 g/dL) after pasteurization. There is a profound reduction of fat components (20.5%) after pasteurization. Such great loss of fat components was also noted in Adhisivam's study. 21
The protein level of pasteurized milk significantly decreased than raw milk with 3.9% and 2.5% loss in the study by Vieira et al. 17 and Piemontese et al., 15 respectively. Such as fat, a profound decrease of protein concentration was also noted in Adhisivam's study. 21 In most studies, there was no difference in the mean protein concentration of raw and holder pasteurized bank milk samples. It is more important to note that although the difference of total protein concentration in raw and processed donor milk was within 0.3 mg/mL, activity levels of some specific proteins or amino acid level still can be influenced by heated process.2,20–22
Regarding lactose, most previous studies had consensus that the carbohydrates are not significantly affected by Holder Pasteurization, even using different analytical techniques.2,23 The significant increase in lactose concentration was only revealed in Ley's study and in our study, although the former study enrolled quite small number of samples.
The analyzer shows the content of fat, protein, and lactose, which provide the energy calculated as rules. So the measurements of energy depend much on fat change (9.25 kcal/g × fat g/dL). In Ley's study, even with the fat loss up to 8.9%, the energy showed no significant change. This may be contributed by the significant increased lactose level. The subtle balance between macronutrients and energy can also explain our result. The increased lactose concentration (3.95 kcal/g × lactose g/dL) with unknown reason could be the explanation that the energy loss limited to around 5% in our study, even with the profound decrease in fat components.
Effect of freezing
The breastfeeding mother or the donors are mostly educated to ensure the microbiological safety of human milk, the optimal freezing, and storage of expressed milk. The low temperature inhibits the growth of microorganisms while retaining the enzyme activity. How long can the bank milk be preserved and what temperature should be recommended for prolonged storage are not in consensus. A systematic review by Schlotterer and Perrin had focused the effects of refrigerated/frozen storage on bank milk. The results revealed that long-term storage of breast milk seemed safe without compromising its microbial purity. 24 But the effect of frozen storage on macronutrients concentration still has limited data. The latest studies in recent 10 years (2009–2019) concerning about the frozen storage effect on macronutrients (fat, protein, and lactose/carbohydrate) of breast milk were also searched in PubMed and reviewed as Table 3.
The Effect of Frozen Storage on Macronutrients Concentration of Breast Milk
SD, standard deviation.
Although the duration of storage varied from 24 hours to 12 months, most studies showed significantly decrease of fat components (2.4–11.3%) after frozen at −20°C or −80°C. The long-term duration effect on fat concentration was also noted in a 2012 and a 2013 study by Gracia-Lara et al.,17,25 and there were similar results, no matter stored at −20°C or −80°C, in the 2019 study by Orbach et al. 26 The longer the breast milk is stored, the more the loss of fat components. The change was not reported in the study of de Waard et al. 27 The freezing and thawing processes had been demonstrated to alter the fat globule membrane and enable the action of lipase on triglycerides, thus increasing the concentration of free fatty acids. The oxidized fatty acids cannot be quantified with the human milk analyzer, which may explain the decreased fat concentration.28,29
In contrast to findings of fat, the protein content stayed stable during periods of frozen storage in most studies.17,25,26,30 In the 2011 study by Vieira et al., there was a small but significant decrease in the protein content (2%). 17 In 2018, de Waard et al. reported a significant increase in protein content (13.4% relative increase, p = 0.037), and the cause of relatively lower baseline protein content compared to all other time points is unclear. 27
In 2011, Vieira et al. reported no significant changes in lactose concentrations (p = 0.427) after 24 hours of frozen storage. 17 In a 2018 study of de Waard et al., there was also no significant change in carbohydrate concentrations over 12 months of frozen storage. Similar results were revealed in 2019 study by Orbach et al., with frozen storage up to 24 weeks, no matter at −20°C or −80°C (p = 0.723). 26 However, in the 2013 study by Gracía-Lara et al., there was a small but significant decrease in the carbohydrate content (loss 1.7%, p = 0.006) after frozen for 180 days. 18 Our study also reported a significant change from 7.40 g/dL to 7.17 g/dL (loss 3.1%, p = 0.001) after frozen for 3 months. In their 2014 study about preterm human milk frozen at −80°C, Lev et al. found that the amplitude of the decline in carbohydrate content was much higher (30.2%,) and the decline correlated significantly with the freezing duration. The effect of adhesion of macronutrients to container walls is speculated. 30
These studies suggest that the fat components decrease after frozen storage at −20°C or −80°C for any duration. The protein level was stable. The carbohydrate/lactose concentration may decrease a little or stay without change, unless stored at −80°C. Overall, these decreases correspond to reduction in energy content from 2.2% to 12.7% significantly after frozen storage.
Since there is concern about the prolonged frozen storage, the processed pooled donor milk was stored at room temperature for 5 to 7 months in Ding's study. The nutritional composition of the donor milk is not affected and is ready for use when needed. 19 The effect on nutrients and the microbial safety of the bank milk by repeated freezing/thawing and the temperature/duration of storage needed more evidence.
Conclusion
Data from our study revealed that the processing of bank milk (including Holder Pasteurization and frozen storage) decreased fat and energy content of human milk significantly. This might not be enough to meet the specific needs of preterm infants. Further studies are needed to evaluate such great loss of nutrients.
Footnotes
Acknowledgments
The authors thank all the human milk donors for their participation in this study.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.