
Abstract
Objective:
To explore, in a large, nationally representative U.S. sample of children, potential independent associations between social and community factors and breastfeeding outcomes, using the Social Ecological Model as a theoretical framework.
Materials and Methods:
A secondary data analysis of the 2011–2012 National Survey of Children's Health was conducted (N = 29,829). Multivariate logistic regression was performed to estimate associations between predictor variables (parental emotional support, neighborhood social support, neighborhood safety, neighborhood amenities, and medical home) and breastfeeding outcomes (breastfeeding initiation [BFI] and exclusive breastfeeding for 6 months [EBF6m]). For predictor variables reaching statistical significance in the adjusted models, we performed subgroup analyses by race-ethnicity.
Results:
After adjusting for individual- and family-level sociodemographic and maternal-child health factors, living in a neighborhood with 4 amenities was associated with 1.54 (95% confidence interval [CI] 1.06–2.23) times the odds of BFI, compared to children living in neighborhoods with no amenities. There was a negative association (adjusted odds ratio [aOR] 0.83; 95% CI 0.70–0.99) between neighborhood social support and BFI, although living in a supportive neighborhood was associated with 1.37 (95% CI 1.11–1.69) times the odds of EBF6m. There was a negative association (aOR 0.71; 95% CI 0.54–0.93) between perceived neighborhood safety and EBF6m. The observed associations differed by race-ethnicity.
Conclusion:
Community-level structural and social support factors influence breastfeeding outcomes, independent of previously described individual level sociodemographic factors, and the observed associations differ by race-ethnicity. These findings have implications for the development of “breastfeeding-friendly” communities and public policies.
Introduction
Human milk is the gold standard of nutrition for most infants and is the physiologic norm.1,2 Feeding of human milk substitutes is associated with an increased risk of acute and chronic childhood illnesses and infant mortality compared to mother's own milk.3,4 Mothers who do not breastfeed are at increased risk of premenopausal breast cancer, ovarian cancer, type 2 diabetes, and postpartum depression.3–5 These effects are duration and dose-dependent, with the health benefits of exclusive breastfeeding being superior to partial or no breastfeeding. 4 Because of its many health benefits, the World Health Organization (WHO), the American Academy of Pediatrics (AAP), and other health authorities recommend exclusive breastfeeding of infants until 6 months of age, followed by continued breastfeeding with the introduction of complementary foods for at least 1 (AAP) to 2 (WHO) years.1,6
While breastfeeding rates have been increasing in the United States, stark disparities in rates of initiation, duration, and exclusivity persist.7,8 Sociodemographic predictors of breastfeeding outcomes have been well-documented.9–15 For example, investigators report lower rates of breastfeeding among African American and Native American women and among women who are young, less educated, single, and low income.9,14,16,17 Acculturation also plays a role in the prevalence of breastfeeding in the United States, with first-generation immigrant mothers being more likely to breastfeed than their U.S.-born peers. 14 Although individual and family-level risk factors are important to understand, they may mask community-level differences in access to health-promoting factors—such as neighborhood resources, social cohesion and safety, and access to primary care services—that could be targets for child health promotion interventions.
Infant feeding decisions are not made in a vacuum, but rather in a social and community context that includes influences from extended family, friends, coworkers, health care providers, media images, direct marketing and advertising, local and national policies, and prevailing cultural and religious norms. A useful conceptual framework for these interactions is Bronfenbrenner's Social Ecological Model (SEM; Fig. 1).18,19 As described by this model, individual health is influenced not only by personal physiology, knowledge, and attitudes but also through social interactions and the community, societal, and policy contexts in which one lives.

The social ecological model of health.
In recent years, there has been a growing exploration of the influence of neighborhood factors on reproductive and perinatal health.20–24 For example, Culhane and Elo proposed a conceptual model linking neighborhood physical characteristics, social environment, and service environment to birth outcomes such as preterm birth, low birth weight, and infant mortality. 23 Few investigators, however, have specifically explored associations between neighborhood context and breastfeeding in the United States, and the results of those studies have been mixed. In an analysis of the Fragile Families and Child Wellbeing Study of primarily unwed U.S. parents, living in a highly educated neighborhood was associated with 25% higher odds of breastfeeding initiation (BFI) and 13% higher odds of breastfeeding for 6 months or more, after adjusting for individual-level socioeconomic and other neighborhood contextual factors. 16 In contrast, in a study of Pregnancy Risk Assessment Monitoring System (PRAMS) data from Washington and Florida, Cubbin et al. found no significant associations between neighborhood deprivation (as measured by the Townsend Index) and breastfeeding, after adjusting for individual-level socioeconomic characteristics. 22 Ethnographic data from a sample of low-income, African American mothers in Baltimore, Maryland who were enrolled in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) revealed that mothers' concerns about personal safety impacted breastfeeding decisions. 25 In a nationally representative sample of respondents in the United Kingdom's Millennium Cohort Study, neighborhood deprivation was negatively associated with BFI, and BFI, duration, and exclusivity were each reduced by ∼20% among mothers who perceived their neighborhoods as unsafe for children. 26
Qualitative studies of mothers' infant feeding decisions have demonstrated the impact of partner, extended family, and particularly grandmother support on breastfeeding outcomes.27–29 In general, positive family and partner support appear to contribute to the initiation and continuation of breastfeeding, but the construct of “support” is complex. 27 Social support can be described as practical, informational, or emotional, and may or may not be compatible with the mother's breastfeeding goals. 27 In a recent analysis of data from the Infant Feeding Practices Survey II (2005–2007), mothers who perceived that the baby's father or the maternal grandmother preferred exclusive breastfeeding (compared to preferring another feeding method) had 7.44 and 2.45 times the odds of intending to exclusively breastfeed in the first few weeks postpartum, respectively. 30 In contrast, a study of racially diverse mothers of very-low-birth-weight infants demonstrated a negative correlation between perceived breastfeeding support from the maternal grandmother and human milk feeding at discharge from the Neonatal Intensive Care Unit (NICU). 31
Recent research demonstrates a strong dose-response relationship between the number of sources of advice encouraging breastfeeding (including baby's physician and birth hospital nurses) and maternal breastfeeding outcomes. 32 Further, health care providers' opinions regarding the importance of their breastfeeding advice are associated with duration of exclusive breastfeeding among mothers. 33 In 2017, the AAP published a clinical report outlining steps needed for providers and health system administrators to create breastfeeding-friendly pediatric outpatient practices. 34 Whether use of a medical home is associated with breastfeeding outcomes, however, is a question that has not yet been explored.
Understanding whether relationships exist between social and community-level factors and breastfeeding outcomes, independent of individual-level sociodemographic factors, has important public health and policy implications. These associations, however, have not been fully investigated at the population level. Using the SEM as a guiding framework, the objective of this study was to determine, in a large, nationally representative sample, whether parental emotional support, neighborhood context (social support, safety, and amenities), and use of a medical home were associated with BFI and 6-month exclusivity, independent of previously described individual-level sociodemographic risk factors. We hypothesized that increased parental emotional support, neighborhood social support, neighborhood safety, and neighborhood amenities, as well as the child receiving care in a medical home, would be associated with increased likelihood of BFI and 6-month exclusivity.
Materials and Methods
Data source
We used data from the 2011–2012 National Survey of Children's Health (NSCH) for this cross-sectional study, which was approved by the Institutional Review Board of the University of Minnesota. The NSCH is a random-digit-dial telephone survey of U.S. households that is sponsored by the Health Resources and Services Administration, Maternal and Child Health Bureau and conducted by the Centers for Disease Control and Prevention (CDC) and the National Center for Health Statistics (NCHS). 35 The 2011–2012 NSCH was conducted in all 50 states and the District of Columbia; results were weighted to represent the population of noninstitutionalized children aged 0–17. The survey is designed to provide national and state-level prevalence estimates for a variety of child health indicators, as well as family and demographic data.
For each household, one child was randomly selected as the subject of the interview; the respondent was a parent or guardian familiar with the child's health (68.7% of respondents were the child's mother, 24.1% were the child's father, and 7.1% other). Informed consent was obtained from all respondents. In total, 95,677 interviews were completed between February 2011 and June 2012. BFI data were collected only for children aged 0 to 5 years at the time of the interview; our analyses were limited to these children (N = 29,829). Among those children included in the initiation sample, 21,533 respondents had data available regarding exclusive breastfeeding for 6 months (EBF6m); this comprised our sample for 6-month exclusivity analysis. The selection of the study population is shown in Figure 2.
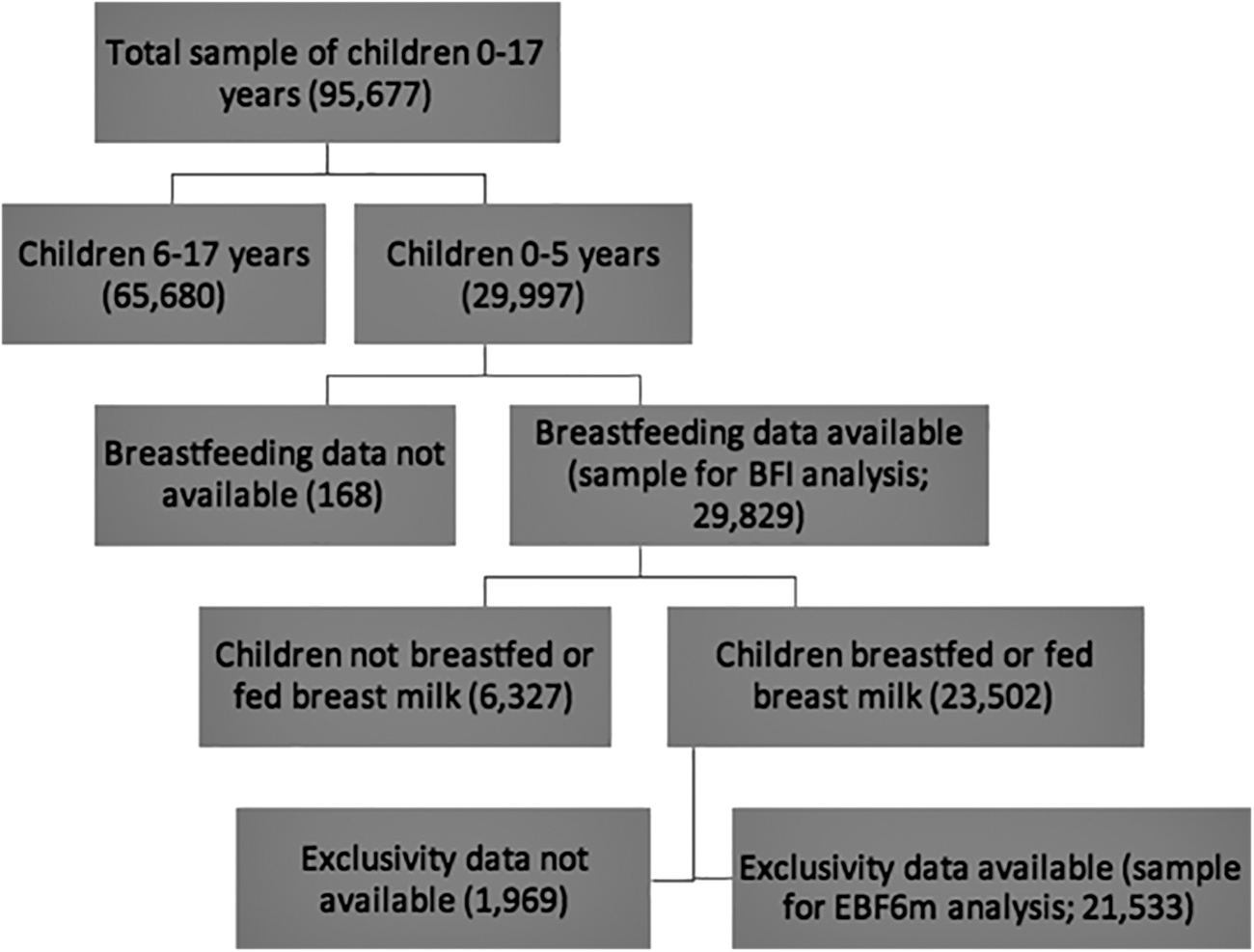
Flow diagram of the study initial population and sample used for analysis of BFI and. BFI, breastfeeding initiation; EBF6m, exclusive breastfeeding for 6 months.
Analytic variables
The outcomes chosen for this study were BFI and EBF6m, consistent with the recommendations of the WHO and the AAP. BFI was considered to have occurred if the parent answered affirmatively to the question, “Was [child's name] ever breastfed or fed breast milk?” EBF6m was determined based on whether the child (1) was at least 6 months old, (2) did not stop breastfeeding before 6 months of age, and (3) was not introduced to formula or anything other than breast milk (including juice, cow's milk, water, sugar water, baby food, or anything else).
Predictor variables were chosen to represent the relationship and community levels of the SEM (Fig. 1). These included the respondent's perceived emotional support, neighborhood social support, neighborhood safety, neighborhood physical amenities (parks/playgrounds, sidewalks/walking paths, community/recreation centers, libraries/bookmobiles), and whether the child was receiving care within a medical home (Appendix Table A1).
In our analyses, we controlled for individual- and family-level sociodemographic and health variables, including maternal age, maternal education level, self-rated maternal physical and mental health, the child's race/ethnicity (Hispanic, non-Hispanic white, non-Hispanic black, non-Hispanic other/Multiracial), preterm birth, low birth weight, whether the respondent was U.S.- or foreign-born, household poverty, and family structure of the child (two parent—biological or adopted; two parent—step family; single mother—no father present; or other family type). Poverty level was derived with single imputation for households lacking income data (9.7% of the sample) and was based on Department of Health and Human Services (DHHS) guidelines.
Statistical analysis
All analyses were performed on weighted data to produce nationally representative estimates. Maternal age was transformed from a continuous to a categorical variable, and the maternal physical and emotional health variables were restructured from five to three categories. The neighborhood safety variable was dichotomized. Neighborhood social support was a composite variable derived from responses to four statements (Appendix Table A1). The medical home variable was a composite based on all positive responses to five component variables (has a personal doctor or nurse, has a usual source of sick and well care, receives family-centered care, has had no problems getting needed referrals, and has received effective care coordination when needed; Appendix Table A1).
We first determined frequency distributions for the individual- and family-level sociodemographic and health variables, breastfeeding outcome variables, and the social and community-level predictor variables of interest. Then, we used Pearson's chi-square test to determine bivariate associations between the predictor and breastfeeding outcome variables. We conducted multivariate logistic regression to determine if social support, neighborhood context, and having a medical home were significantly associated with the odds of BFI and EBF6m after adjustment for individual- and family-level sociodemographic and maternal and child health characteristics. For predictor variables reaching statistical significance in the adjusted models, we performed subgroup analyses by race-ethnicity. Statistical significance was set at p < 0.05. Analyses were performed using Stata 12 SE (StataCorp, College Station, TX).
Results
Sociodemographic characteristics of sample
Sociodemographic, health, social support, and community characteristics of the study population are presented in Table 1. In this sample, mothers were predominantly 30 years or older, U.S.-born, and had postsecondary education. Most (62.3%) identified their children as non-Hispanic white. Approximately one in five respondents (19.3%) was living in a household below the federal poverty level (FPL), whereas 32.9% of respondents reported household incomes at or greater than 400% of the FPL. More than three-quarters of respondents (76.7%) reported that the index child was living in a two parent (biological or adoptive) family. Nearly 12% of the children in the sample were born prematurely (<37 weeks' gestation), and 9.4% were low birth weight (<2,500 g). Most respondents reported the child's mother as having “excellent” or “very good” physical and emotional health (73% and 77.4%, respectively).
Descriptive Characteristics of the Sample (N = 29,829)
The sample size for some variables does not equal 29,829 due to the exclusion of missing data.
FPL; household poverty level imputed by NSCH 2011–12.
BFI, breastfeeding initiation; EBF6m, exclusive breastfeeding for 6 months; FPL, federal poverty level.
Most respondents (92.3%) reported that they had a person in their lives who provided day-to-day emotional support with parenting. Most (82.3%) reported that the child lived in a supportive neighborhood, and 89.5% reported that the child was “usually/always” safe in their neighborhood. Slightly more than half of parents (55.1%) reported having all four categories of physical amenities in their neighborhood. Nearly two-thirds (64.4%) of children received care within a medical home.
Associations between social and community characteristics and breastfeeding outcomes
Among children aged 0–5 years at the time of the survey, 78.8% had ever been breastfed, and of these, 20.6% were breastfed exclusively for 6 months of age (EBF6m; 16.2% of the total sample; Table 1).
Bivariate associations between the social and community-level predictor variables, BFI and EBF6m are shown in Table 2. The rates of BFI were significantly higher for children whose parent has an emotional support person, who live in a supportive neighborhood, whose parents feel the child is “always” or “usually” safe in their neighborhood, who live in neighborhoods with more amenities, and who received care within a medical home. The rates of EBF6m were significantly higher for children living in supportive and safe neighborhoods, for those living in neighborhoods with four amenities, and for those receiving care within a medical home.
Bivariate Associations Among Predictor Variables, Breastfeeding Initiation, and Exclusive Breastfeeding for 6 Months
BFI, breastfeeding initiation; EBF6m, exclusive breastfeeding for 6 months.
In the unadjusted regression analysis, BFI was significantly associated with the parent having an emotional support person, parent perception of neighborhood safety, living in a neighborhood with two or more amenities (parks/playgrounds, sidewalks/walking paths, community/recreation centers, libraries/bookmobiles), and the child receiving care within a medical home (Table 3). After adjusting for individual- and family-level socioeconomic and health variables, children living in neighborhoods with four amenities had significantly increased odds (adjusted odds ratio [aOR] 1.54; 95% confidence interval [CI] 1.06–2.23) of BFI, compared to those living in neighborhoods with no amenities. Subgroup analysis by race-ethnicity demonstrated that this finding held true only for those who identified their child's race-ethnicity as Hispanic (aOR 2.89; 95% CI 1.23–6.79) or non-Hispanic white (aOR 1.49; 95% CI 1.04–2.13; data not shown). There was no independent association between neighborhood amenities and BFI for those identifying their children as non-Hispanic black or other/multiracial. In the fully adjusted model, neighborhood social support exhibited a weak negative association with BFI (aOR 0.83; 95% CI 0.70–0.99). This finding, however, was present only for non-Hispanic black children (aOR 0.65; 95% CI 0.45–0.93); neighborhood social support was not associated with BFI for any other race-ethnic subgroup (data not shown).
Unadjusted and Adjusted Odds of Breastfeeding Initiation and Exclusive Breastfeeding for 6 Months, NSCH 2011–12
Adjusted for maternal age, maternal education level, child's race/ethnicity, maternal nativity status, maternal physical health, maternal mental health, prematurity, low birth weight, household income, family structure, and all other variables in this table.
p < 0.05; **p < 0.01; ***p < 0.001.
aOR, adjusted odds ratio; NSCH, National Survey of Children's Health; OR, odds ratio.
EBF6m was significantly associated with perception of neighborhood social support in both unadjusted and adjusted models (Table 3). After adjusting for individual- and family-level variables, children whose parents reported living in a supportive neighborhood had 1.37 (95% CI 1.11–1.69) times higher odds of exclusively breastfeeding to 6 months of age, compared to those whose parents who did not describe their neighborhood as supportive. In race-ethnic subgroup analysis, however, this finding was significant only for Hispanic children (aOR 2.17; 95% CI 1.35–3.48; data not shown). Living in a “usually” or “always” safe neighborhood was associated with 0.71 (95% CI 0.54–0.93) times the adjusted odds of EBF6m, but only among non-Hispanic black children (aOR 0.54; 95% CI 0.32–0.92; data not shown); for the remaining race-ethnic groups, neighborhood safety was not significantly associated with EBF6m. There was a trend toward increased odds of EBF6m for those children meeting criteria for having a medical home, but the relationship did not reach statistical significance. There were no significant associations between parental social support or neighborhood amenities and EBF6m.
Discussion
In this large, nationally representative sample from the 2011–2012 National Survey of Children's Health, BFI was positively associated with the presence of an emotional support person in the parent's life, neighborhood safety, increased number of neighborhood amenities, and having a medical home. After adjusting for a broad range of individual- and family-level factors (sociodemographic measures, maternal physical and emotional health, prematurity, and low birth weight), living in a neighborhood with four amenities (parks/playgrounds, sidewalks/walking paths, community/recreation centers, and libraries/bookmobiles) remained independently associated with increased odds of BFI, compared to living in a neighborhood with none of these amenities. In race-ethnic subpopulation analysis, however, this association was seen only among Hispanic and non-Hispanic white children.
These results support the findings of Peregrino et al. who found that after adjustment for individual- and family-level sociodemographic variables, BFI was 40% less likely in those living in the most deprived neighborhoods in the United Kingdom, compared to those living in the least deprived. 26 Yourkavitch et al. similarly found that among children liveborn in New Jersey in 2006, the associations of neighborhood disadvantage and affluence with breastfeeding practices differed by race-ethnicity; the odds of any breastfeeding decreased with increasing neighborhood disadvantage only for Hispanic women. 36 In the U.S. context, the independent association between high-amenity neighborhoods and BFI may reflect a concept described as “first food deserts”—concentrated geographic areas lacking community resources for breastfeeding support, such as Baby Friendly Hospital Initiative (BFHI)-accredited birthing facilities, which have been associated with increased BFI.37,38 The association we observed may also reflect the fact that amenities like libraries, community centers, and parks provide spaces for parents to connect with educational resources and other breastfeeding support. Access to these types of community resources may only impact breastfeeding decisions for certain subpopulations, however.
Interestingly, there was a weak negative association between perceived neighborhood social support and BFI while a positive association was noted for EBF6m. Subgroup analysis, however, revealed that the former association was only present for non-Hispanic black children, while the latter was only true for Hispanic children. This finding may reflect neighborhood-based social norms that influence infant feeding choices in different ways. Qualitative research on social support and breastfeeding decisions has indicated that the construct of “support” is complex, and may or may not be compatible with the mother's breastfeeding goals. 27 Further, Bentley et al. found that among a group of low-income, African American mothers, decisions regarding breastfeeding were shaped by beliefs around power and a desire to raise children not dependent upon their mothers for survival; these cultural norms may be rooted in generational historical trauma. 25
Parental report of living in a supportive neighborhood was associated with increased odds of EBF6m in both our crude and adjusted models. This is not surprising, given that infant feeding commonly occurs in the community setting and that social norms impact feeding decisions—for example, breastfeeding in public. This finding is in contrast to that of Peregrino et al., who did not observe an association between maternal perception of the level of “friendliness” of neighbors and exclusive breastfeeding to 3 months. 26 Subgroup analysis of our data, however, suggested that the positive association of neighborhood support and EBF6m was only present for Hispanic children; no significant association was noted for other race-ethnic groups. The contrast between this positive association with EBF6m for mothers of Hispanic children, and the negative association with BFI for mothers of non-Hispanic black children, implies that neighborhood social support may impact breastfeeding decisions differently for different racial-ethnic communities, depending on prevailing social norms.
After adjustment for individual- and family-level variables, living in a safe neighborhood was associated with decreased odds of EBF6m, in contrast to our hypothesis. This association was seen only among mothers of non-Hispanic black children, however; no association between perceived neighborhood safety and EBF6m was noted for other race-ethnic groups. Our finding stands in contrast to the observations of Bentley et al. 25 and Peregrino et al., 26 who found that breastfeeding was more likely when neighborhood were perceived as safe.
Although there was a trend toward a positive association between having a medical home and EBF6m, the result did not reach statistical significance in either model. Guidelines for establishment of a breastfeeding-friendly medical office have been published, and implementation of the recommended practices has resulted in increased exclusive breastfeeding rates in one study.34,39,40 To our knowledge, however, no prior studies have evaluated the potential relationship between access to and use of a medical home and breastfeeding outcomes, specifically.
It is possible that, similar to the findings of Cubbin et al., the apparent associations of parental emotional support, neighborhood safety, lower numbers of neighborhood amenities, and receiving care within a medical home with BFI in our crude analysis were confounded by individual- and/or family-level factors and were attenuated after adjustment for these factors. 22 Further, some factors that may be associated with BFI and duration, such as body mass index, mode of delivery, parity, prior breastfeeding experience, and paid maternity leave, were not controlled for in this analysis.41,42
Limitations of this study include its cross-sectional design and its reliance on parent or guardian recall of up to 5 years duration, which makes the data subject to potential recall bias. Further, it is possible that the social, neighborhood, and medical home context at the time of the respondent's report was not the same as during the period of infant feeding (e.g., due to a change in residence, which may be more frequent among low-income respondents). Finally, the construct of “support” contains complexity beyond the scope of the NSCH; the interpretation of our findings is limited by the definitions included in the survey.
Nonetheless, to our knowledge, this analysis is the first to explore the relationships of community-level factors such as neighborhood context and medical home with breastfeeding outcomes in a large, nationally representative sample of U.S. children. Our findings suggest that neighborhood amenities, social support, and safety are independently associated with initiation and 6-month exclusivity of breastfeeding, respectively, and that these associations differ by race-ethnicity. These data reflect the nuanced interplay between neighborhood context, social norms, and infant feeding practices, and indicate a need for different types of breastfeeding support for different communities.
Conclusions
These observations suggest a role for public health experts, policymakers, and urban planners in the development of “breastfeeding-friendly” communities. This study contributes to the evidence that the social and structural health of a neighborhood directly impacts the health of its residents. It strengthens the body of evidence for associations between neighborhood context and perinatal health outcomes, and demonstrates that these associations differ by race-ethnicity. Further research is needed to better understand the community-level factors that impact breastfeeding outcomes and inform potential neighborhood-based public health interventions. Future studies should also investigate the impact of medical home utilization on breastfeeding outcomes.
Footnotes
Disclaimer
This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by Health Resources and Services Administration (HRSA), U.S. Department of Health and Human Services (DHHS) or the U.S. Government.
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (DHHS) under National Research Service Award in Primary Medical Care grant number T32HP22239 (PI: I.B.), Bureau of Health Workforce.
Appendix
Questions and Response Options Used in the 2011–2012 National Survey of Children's Health for Predictor Variables by Social Ecological Model level
| Question | Response options |
|---|---|
| Relationship level: Social support | |
| Is there someone that you can turn to for day-to-day emotional help with [parenthood/raising children]? | Yes; no; don't know/refused |
| Community Level: Neighborhood and Medical Home | |
| Does [child] live in a supportive neighborhood? | Yes; no |
| Derived from responses to four statements: | For questions 1–4, response options were: Strongly disagree; somewhat disagree; somewhat agree; strongly agree. Responses were assigned a value from 1 (strongly disagree) to 4 (strongly agree) and an average was calculated for cases with response to at least three of the four questions. |
| 1. People in my neighborhood help each other out | |
| 2. We watch out for each other's children in this neighborhood | |
| 3. There are people I can count on in this neighborhood | |
| 4. If my child were outside playing and got hurt or scared, there are adults nearby who I trust to help my child | Child considered to live in a supportive neighborhood of the mean response score was 2.25 or higher, indicating no more than one “disagree” response. |
| How often do you feel [child] is safe in your community or neighborhood? | Dichotomized to usually/always safe; never/sometimes safe |
| Presence of neighborhood amenities: | Count of “yes” responses (range 0–4) |
| 1. Do sidewalks or walking paths exist in your neighborhood? | |
| 2. Does a park or playground area exist in your neighborhood? | |
| 3. Does a recreation center, community center, or boys' or girls' club exist in your community? | |
| 4. Does a library or bookmobile exist in your community? | |
| Does [child] receive care within a medical home? | Yes; no |
| Composite measure based on 5 component variables constructed from 19 survey items: | To qualify as “yes,” child must meet criteria for adequate care on the first three components. Any children who needed referrals or care coordination must also have met criteria for those components to qualify as having a medical home |
| 1. Personal doctor or nurse | |
| 2. Usual source of sick and well care | |
| 3. Family-centered care | |
| 4. Problems getting needed referrals | |
| 5. Effective care coordination when needed | |