
Abstract
Preterm and sick term infants are commonly fed with expressed breast milk (EBM) that has been subjected to various storage and handling conditions before feeding that may cause lipase-mediated elevation of free fatty acids (FFA). This study was designed to describe the variation, between mothers' and within the same mother over time, in the concentration of FFA in EBM used in an Australian neonatal unit. A total of 256 EBM samples, 149 freshly expressed in the unit cot-side and 87 expressed at home and brought in to the unit, were collected from 32 mothers with an infant admitted to the neonatal intensive and/or special care units at the Women's and Children's Hospital, Adelaide. Among the fresh EBM samples collected cot-side, the average total fat content was 29.78 ± 9.28 mg/mL, and the FFA concentration was 1.70% of total fats (interquartile range [IQR]: 1.17–2.37%). Among the 10 mothers who provided fresh EBM at different stages of lactation, the concentration of FFA remained low overall, with some day-to-day variation (min 0.58% and max 5.0% of total fats within the same mother). The average total fat content of home collected EBM was similar to the cot-side collected samples, at 27.37 ± 8.23 mg/mL, and the FFA concentration was slightly higher at 2.49% of total fats (IQR: 1.74–3.29%). Overall, the FFA concentration of breast milk in the neonatal unit before and even after a short period of cold storage and handling is universally low.
Introduction
Human milk, from an infant's own mother or, if unavailable, milk from a donor, is the preferred food for infants. 1 Human milk is especially critical for infants born preterm (<37 weeks' gestation). A recent meta-analysis found that an exclusive human milk diet for preterm infants reduces the risk of necrotizing enterocolitis and may also be beneficial for late-onset sepsis and retinopathy of prematurity, compared with an exclusive preterm formula diet. 2 Preterm infants who are too immature to suckle and near-term to term infants who are too sick to feed from the breast must be fed expressed breast milk (EBM) using a tube. This EBM may have been subjected to various handling and storage processes, including expression, fridge and freezer storage, transport to the neonatal unit, and then thawing. These processes may alter the composition of milk, particularly the fat composition, due to the presence of endogenous lipases that are capable of breaking down milk triglycerides (TG) and releasing free fatty acids (FFA) even at low temperature. 3
Previous studies4–6 indicate that only small amounts of FFA (under 2%) are present in fresh EBM, which is similar to levels in fresh bovine milk. There is debate regarding the significance of elevated concentrations of FFA in breast milk in infants' health: whether it is beneficial by providing a predigested readily available source of energy 6 or a cause of concern as it can increase osmolality of the milk, which can cause adverse gastrointestinal symptoms. 7 These questions are particularly relevant to the sickest, most vulnerable preterm infants who start life in the neonatal unit.
The fat composition of breast milk is known to be affected by many factors including, but not limited to maternal diet, lactation stages, gestation of infants at birth, and timing of expression. 8 To better understand the role of FFA, further research that accurately measures the endogenous concentration of FFA in fresh breast milk is required, with exploration of possible variation within and between individuals and across different stages of lactation. Earlier studies have suffered from methodological issues, including small sample sizes and suboptimal handling technique that may lead to enhanced degradation of TG during the sampling and processing, 5 resulting in an inflated FFA concentration. In addition, conventional thin layer chromatography, the predominant method used in earlier studies, can be prone to contamination from TG tailing during FFA separation.
We have recently described a dried milk spot (DMS) system whereby these two major concerns were eliminated using a conventional microwave oven to denature lipases and a specific analytical column that detects FFA without interference from TG. 9 Using the DMS method, we aimed to profile naturally occurring variations in fresh EBM that was sampled immediately after expression of milk at the cot-side. We also aimed to measure the effect of stage of lactation on the concentration of FFA in fresh EBM within the same mother and to measure the variations in FFA concentration of breast milk that was expressed at home and brought into the neonatal unit.
Materials and Methods
Participants
Eligible women included all mothers with an infant or infants admitted to the neonatal unit (intensive and special care units) at the Women's and Children's Hospital, North Adelaide, who were supplying EBM and had a surplus of milk beyond what their infant or infants' required for growth.
Breast milk sample collection
Two types of EBM were collected in this study: (1) fresh EBM that was expressed at the cot-side during a visit in the neonatal unit and (2) home collected EBM that was subsequently transported to the unit. Participating mothers EBM primarily using hospital grade electric pumps, and hand expression might be used to assist the expression to maximize the quantity of milk obtained. At the end of a single episode of expression, EBM from both breasts were pooled together into a sterile container. Fresh EBM was sampled immediately after completion of expression at the cot-side, and home collected EBM was sampled immediately upon arrival in the unit. All home collected EBM in the study was stored in the home fridge before delivery to the hospital. All mothers followed the hospital guidelines and transported EBM in an insulated bag or a hard-walled cool box with ice bricks or equivalent.
As the goal of the study was to examine the FFA concentration overall and then investigate the effect of stage of lactation, we aimed to collect EBM from each participant twice a week, during the first week postpartum, second week postpartum, and third week postpartum and beyond until hospital discharge. However, in the context of a busy neonatal unit and to minimize impost on families, we took a pragmatic and opportunistic approach to sampling, which meant that not all women provided samples at each of these time points, and women could provide either fresh EBM samples or home collected EBM (or both). Furthermore, as we did not collect samples postdischarge, mothers of longer stay infants tended to contribute the most samples.
Ethical approval for the study was granted by the Women's and Children's Health Network Human Research Ethics Committee (Approval number HREC/19/WCHN/19).
Laboratory analysis
For each collection, 20 μL of EBM was collected on each of two filter paper discs in a premanufactured card and allowed to dry. The DMS card was then microwaved (NN-S235WF, 5.4A, 50Hz, 800W; Panasonic Home Appliance Co., Ltd) at high power for 3 minutes as described in a previous report. 9
The total fatty acids (equivalent to total fats) and FFA analyses were conducted using methods detailed previously. 9 Briefly, each DMS spot was excised with cleaned scissors and tweezers and then transferred into 6 mL vials. Twenty microliters of internal standard (triheptanoic acid C13:0) were added on the spots. For FFA analysis, the elution of milk fats from one of the spots was achieved with two washes of acetone (1 mL each), and the resulting acetone was dried under nitrogen and then reconstituted in 100 μL heptane. The other DMS spot was used for total fatty acid analysis, which was achieved by transmethylating into fatty acid methyl esters (FAME) in 2 mL 1% sulfuric acid in methanol at 70°C for 3 hours. The FAME was then extracted with heptane.
The nonesterified FFA and FAME were then analyzed by gas chromatography equipped with flame ionized detector (GC-FID) as described previously. 9 For FFA separation we used a GC-FID (Agilent Technology 7890B, Santa Clara, CA) equipped with a BP21 column (free fatty acid phase, 10 m × 0.25 mm, film thickness of 0.25 μm; Trajan Scientific Australia Pty Ltd); the temperature ramp was set between 180°C and 240°C with a helium flow of 3 mL/min. For FAME separation, GC-FID (Hewlett-Packard 6890, Palo Alto, CA) equipped with a BPX70 column (30 m × 0.25 mm, film thickness of 0.25 μm, Trajan Scientific Australia Pty Ltd) was used, with a temperature ramp set between 140°C and 240°C and helium flow of 2 mL/min.
Statistical analysis
Breast milk total fat content was expressed as mg/mL, and FFA concentration was reported as percentage of total fats. Results were presented as either a mean and standard deviation or median and interquartile range (IQR; based on the distribution of data). Data were analyzed using SPSS (Version 24; IBM Crop, Armonk, NY) and plotted using GraphPad Prism 8 (GraphPad Software, LA Jolla, CA). The possible association between storage time and the fat composition of home collected EBM was examined by calculating the Pearson's correlation coefficient. No further statistical analysis was performed, as this exploratory observational study was designed to explore the possible variations occurring in EBM samples, but was not powered to define the levels of FFA in EBM.
Results
Thirty-four mothers were enrolled in the study: one withdrew due to low milk supply after an episode of mastitis and another withdrew as she returned to work. EBM samples were collected from the remaining 32 mothers, who are described in Table 1. The majority (28/32) gave birth to preterm infants, including 21 who gave birth to an infant or infants' born <34 week's gestation, considered early preterm.
Demographic Characteristics of Mothers (n = 32)
Data are either presented as mean ± SD or n (%).
Superscript refers to number of days of a complete week.
A total of 256 EBM samples were collected, including 149 freshly expressed in the unit and 87 expressed at home and brought into the unit. The total fat data of all were normally distributed, while the FFA concentration data were negatively skewed.
Fresh EBM
Overall, the total fat content in the fresh EBM samples was 29.78 ± 9.28 mg/mL, with FFA accounting for 1.70% (IQR: 1.17–2.37%) of the total fats. The concentration of FFA and total fats of fresh EBM based on different stages of lactation (first, second, and third week postpartum and beyond) and by gestation are presented in Table 2. There was a trend toward increased total fat concentration as lactation progressed from ∼21 mg/mL in the first week postpartum to 31 mg/mL in the third week postpartum and beyond, but the concentration of FFA remained relatively stable, accounting for ∼2% of total fats across each stage. There was a possible trend that the FFA concentration of fresh EBM from mothers of late preterm infants tended to increase over time, whereas the EBM from mothers of early preterm infants declined slightly (Table 2).
The Total Fat Content (mg/mL) and Concentration of Free Fatty Acids (% of Total Fats) of All Freshly Expressed Breast Milk at the Cot-Side According to Gestation at Birth and Stages of Lactation (n = 256)
Data are either presented as median (interquartile range) or mean ± SD.
FFA, free fatty acids.
Ten mothers were able to provide EBM samples at each stage of lactation, and the FFA concentration of the EBM at each collection point is shown in Figure 1. For most mothers, the FFA concentration in EBM was below 5% of total fats across all stages, and there was no clear trend. There was some variation within the same mother across different lactation stages (e.g., minimum of 0.58% and maximum of 5.08%, Fig. 1).
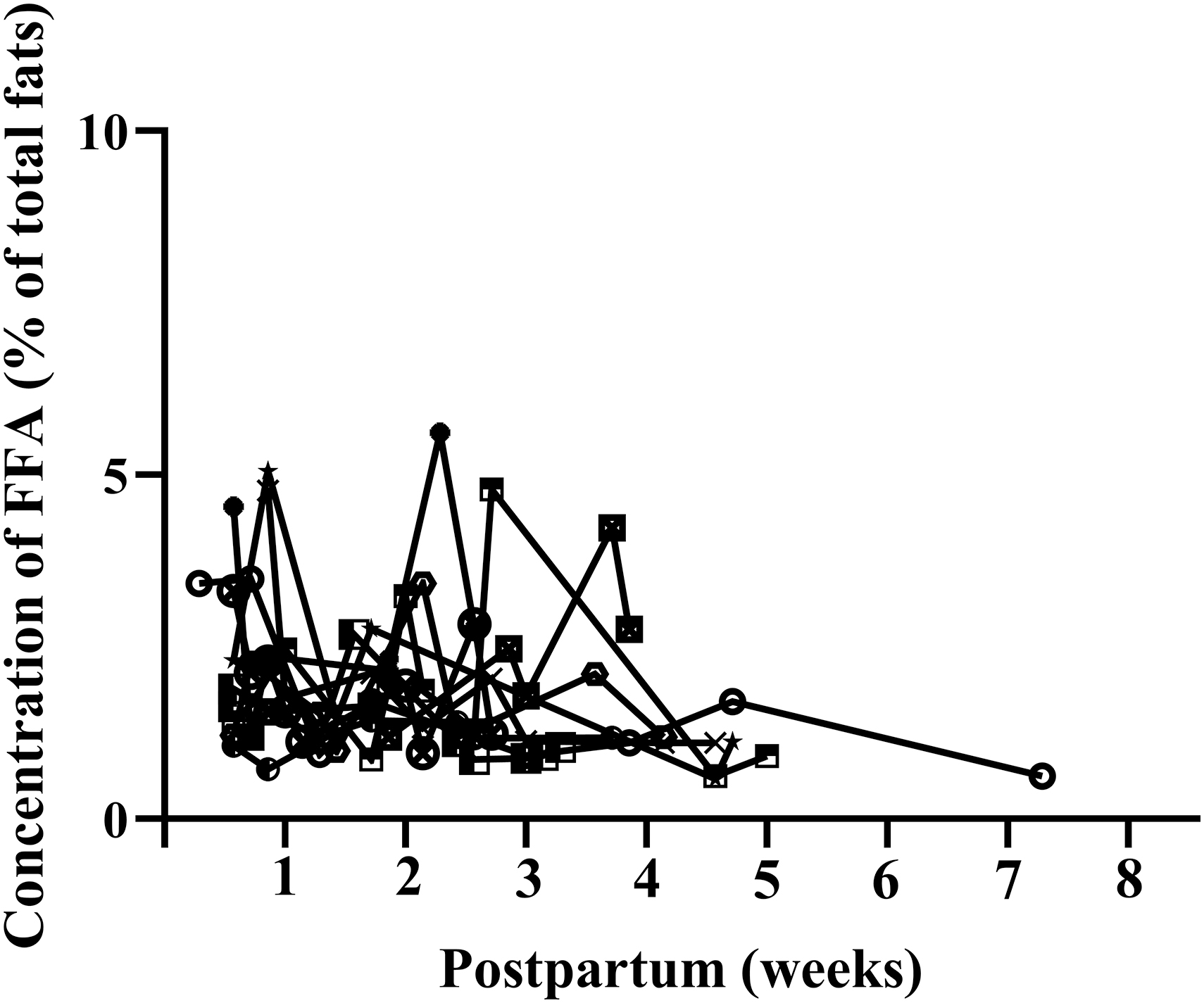
FFA concentration (as % of total fats) of fresh breast milk from 10 mothers who provided samples at each stage of lactation. FFA, free fatty acids.
Home collected EBM
In comparison, the total fat content of home collected EBM was 27.37 ± 8.23 mg/mL, with FFA accounting for 2.49% (IQR: 1.74–3.29%) of the total fats. Similar to fresh EBM collected at the cot-side, there was also a trend toward gradual increase in total fat content as lactation progressed (Table 3). However, the FFA concentration of EBM brought from home was slightly but constantly higher compared with EBM freshly collected at the cot-side, across all different stages of lactation (Table 3).
The Total Fat Content (mg/mL) and Concentration of Free Fatty Acids (% of Total Fats) of Home Expressed Breast Milk According to Gestation at Birth and Stages of Lactation (N = 87)
Data are either presented as median (interquartile range) or mean ± SD.
FFA, free fatty acids.
For home collected EBM, the fat composition was plotted against the time from expression at home to collection at arrival of the unit (Fig. 2). There was a significant correlation between this time and the concentration of FFA (r = 0.6043, p < 0.0001, Fig. 2a). There were two apparent outliers with elevated FFA concentration observed in EBM that was collected 27 and 58 hours postexpression with a FFA concentration of 7.9% and 9.7% of total fats, respectively (Fig. 2a). The FFA concentration of home collected EBM was mostly less than 5% of total fats when sampled within 20 hours postexpression (Fig. 2a). In contrast, the total fat content of home collected EBM was independent of the time from collection to arrival in the unit (r = −0.1402, p = 0.1951, Fig. 2b).
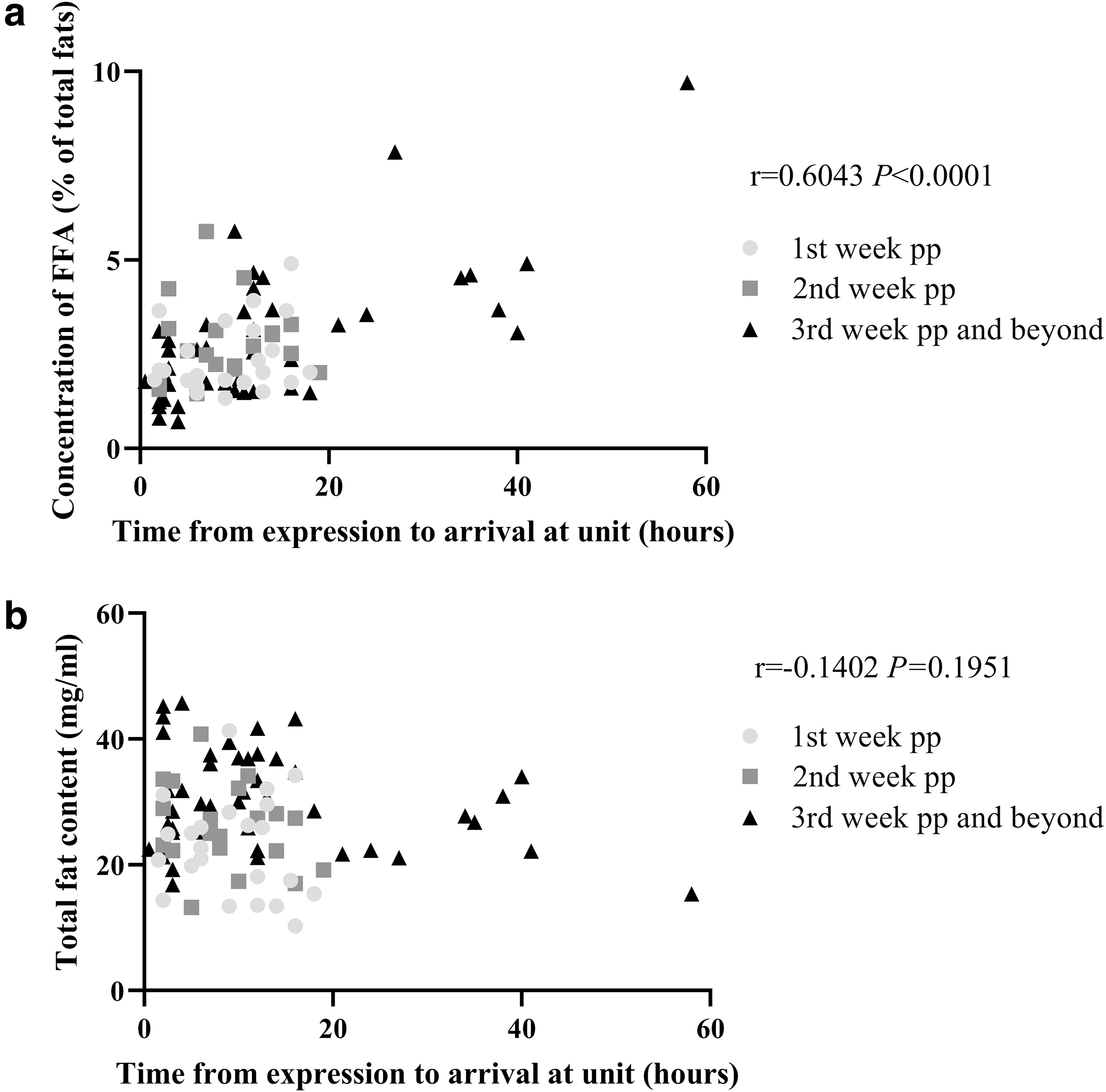
The concentration of FFA (% of total fats,
Discussion
This is the first study that has used a DMS method specifically developed to measure the concentration of FFA in breast milk by eliminating the potential errors that may occur during sample processing as a result of lipolysis or from TG contamination. With this methodology, we report the average concentration of FFA in breast milk from a sample of Australian mothers who had mostly given birth to premature infants. It was found that FFA accounted for only a small percentage of fats in breast milk, regardless of the stage of lactation, or gestation at birth of the infant, although it tended to increase modestly over time with storage. Despite some variation within and between individuals, the concentration of FFA in fresh EBM was mostly below 5%, with a median of 1.7% of total fats.
Due to the technological difficulties associated with the need to eliminate the impact of lipases and preserve the endogenous FFA concentration, few studies have been able to measure the endogenous concentration of FFA in EBM.5,6 Previous research has done this by immediately adding lipase inhibitor 6 or organic solvent 5 following milk collection to prevent the simultaneous breakdown of TG and the release of FFA, but both methods are less practical in a clinical setting and require greater volumes of milk. In addition, potential errors could also be generated when separating FFA from TG. Nevertheless, our findings are broadly consistent with previous studies. For example, Chappell et al. 6 reported that the average concentration of FFA in EBM from mothers delivered term and preterm was 1.9% and 1.5% of total fats, respectively, based on EBM donated by 15 mothers using a TLC separation method. 6 The same authors also claimed that there was a significant increase in the concentration of FFA in EBM with lactation stages from 0.5% to 1.5% of total fats of colostrum and EBM collected on day 7 postpartum, respectively. 6 This trend was observed in both mothers who delivered early preterm infants and term infants. 6 Although not directly comparable, due to differences in the study population and collection and analytical method, in the present study there appeared to be an increase in the FFA concentration of EBM of mothers who delivered late preterm and term infants, from first week postpartum until 3–4 weeks after birth. In contrast, the FFA concentration in the breast milk of mothers who delivered early preterm appeared to decline over time. The reasons for this are unclear and require confirmation in further studies that are appropriately powered to examine the effects of gestation at birth. In addition, further research is required to determine whether these small differences have implications for infant developmental outcomes.
We did not find any other changes in FFA concentration by stage of lactation. Among the subset of 10 mothers who provided repeat samples at each stage, all of whom delivered preterm, there was some day-to-day variation within individuals, where the FFA concentration of fresh EBM from the same person could be as low as 0.5% but as high as just over 5% of total fats. However, overall, the FFA concentration remained universally low at each stage.
In this study, all home collected EBM was refrigerated before delivery to the unit. As the majority of the mothers visited their infants in the unit on a daily basis, the EBM was only temporarily stored in a fridge before transportation to the hospital and collection was completed mostly within 20 hours postexpression. However, as lactation progresses some mothers may accumulate surplus milk and bring the “oldest” EBM for feeding, exposed to the longest storage time. Many in vitro studies have reported an almost linear increase in the concentration of FFA in EBM when the milk is stored at fridge temperatures for prolonged periods, 10 and some claimed a three-fold increase in the FFA concentration from ∼1% to 4%11,12 of total fats (based on a content of milk fats of 30mg/L). Our study observed a small but significant correlation between the storage/transportation time and the concentration of FFA measured in EBM; however, most of the values observed were still less than 5% of total fats and fell within the range of daily variations seen in the fresh EBM samples. These results highlight the stability of EBM under these conditions and therefore, may provide some reassurance to mothers who need to express milk to feed, as well as reinforcing current practices in the neonatal units to promote human milk feeding. Our findings also emphasize the need for caution when interpreting any research related to the concentration of FFA in breast milk as any changes observed may still fall within the variation displayed between individuals, and also the daily variation within the same individual.
A major strength of this study is that we used a DMS method that provides an accurate measurement of FFA concentration, even at very low levels, which eliminated potential errors of detection. The limitations of the study are that the sampling schedule (time of the day) was not prespecified, and not all women contributed EBM samples at each lactation stage. This occurred as we took a pragmatic approach to minimize impost on families in the neonatal unit and timed collection of EBM with their planned visits to the unit. In addition, we had only small numbers of women in some subgroups based on gestational age. However, the purpose of this study was to explore the variation that naturally occurred between mothers; it was not designed to define the FFA concentration of EBM in mothers of preterm and term infants.
Conclusion
The present study reports the median concentration of FFA in fresh and stored EBM collected from Australian mothers of mostly premature infants. We found that the FFA concentration of EBM is universally low, irrespective of gestation at birth and lactation stage, and remain relatively low even after a short period of cold storage postexpression. Future studies are warranted to confirm these findings and to explore the factors that might influence the FFA concentration of EBM.
Footnotes
Acknowledgments
The authors are grateful to all mothers who participated by donating their breast milk to this research and all the nurses, midwives, and dietitians in the neonatal nursery for their assistance.
Disclosure Statement
C.G. receives an Adelaide Graduate Research Scholarship for her PhD candidature at the University of Adelaide. Other authors declare none.
Funding Information
This work is supported by the Nutrition for Mother and Child, Centre of Research Excellence, National Health and Medical Research Centre (APP 1135155).