
Abstract
Background:
Although most women start breastfeeding after delivery, difficulties often arise. One of the main reasons is nipple soreness, which contributes greatly to early cessation of breastfeeding. A soreness evaluation through validated scales, performed by health care professionals during the first few days, can contribute to improve breastfeeding and support for the mothers.
Research Aim:
Knowing the prevalence of nipple soreness during breastfeeding at 48 hours postpartum at the Infanta Cristina University Hospital (Madrid, Spain) through a cross-sectional descriptive study.
Materials and Methods:
The study took place between February and March 2019. A survey of 58 postpartum second day mothers was conducted including the Visual Analogue Scale (VAS) and Lactation Assessment Scale (LATCH) score for breastfeeding assessment. A descriptive analysis of secondary variables and subsequent bivariate inferential was performed for 95% confidence interval (CI).
Results:
The prevalence of nipple soreness observed is 97% (95% CI = 92–100%). It was found, significantly (p = 0.001), that the higher the score on LATCH, the lower the score on VAS and therefore the less pain. We found a relationship between women who were in skin-to-skin contact with their babies for 2 hours without interruption after birth and a higher pain score (p = 0.046). No other associations were found between VAS and other variables such as parity, type of birth, artificial milk supplements for the newborn, or using a pacifier.
Conclusions:
The high percentage of nipple soreness detected highlights that breastfeeding can be unpleasant in the first days after delivery. It is important to include in clinical practice the assessment of nipple soreness and the effectiveness of breastfeeding using validated scales.
Background
The specific recommendations of the World Health Organization 1 (WHO) state that exclusive breastfeeding provides the optimal food until 6 months of age and then together with complementary feeding until at least 2 years of age to achieve adequate growth, development, and level of health.
Despite the effort made by maternity hospitals to implement measures to support the initiation of breastfeeding, such as the WHO and UNICEF's “Ten Steps to Successful Breastfeeding,”2,3 there is a very marked drop in the number of adherences to breastfeeding in the following weeks. In Spain there is no official system to monitor and track breastfeeding start and continuity. Existing data come from National Health Surveys. They gather prevalence data on breastfeeding per months, disregarding WHO indicators about types of feeding. The current percentages on exclusive breastfeeding (when the child receives, from birth solely breast milk and no other food or drinks, excluding medication or vitamins) from the National Health Survey are: 68.40% at 6 weeks, 52.48% at 3 months, and 24.71% at 6 months since birth. 4 These data reflect the fact that they are far from the official recommendations.
Incorrect positioning and/or attachment during takes are considered the main cause for nipple soreness during the first days after birth.5–8
Pain, together with other factors such as feeling of insufficient production, worries about the baby's satiation and health, lack of support, and lack of knowledge about breastfeeding have an influence in the early abandonment of breastfeeding.9–16
With regard to nipple soreness, physiologically, during the first days after delivery a slight pain may be normal, taking into account that the nipples will gradually adapt to their function of breastfeeding. 17 For most mothers, the initial pain reaches its maximum degree on day 3 after giving birth and from then on they perceive a decrease toward day 7.6,18 On the one hand, some women are not prepared for this initial pain and do not know how to manage it. Other women, continue breastfeeding despite an excessive level of pain, being at higher risk of suffering from mastitis, sleep disorder, or even postpartum depression.19–21
As health professionals, the first step in helping mothers manage pain is to recognize and anticipate the problem. 22 The active management of nipple soreness, including early detection and treatment, would help mothers recover in a 2-week period. 7 Support should be established quickly and effectively during the first days after birth, because it is crucial to prevent early abandonment of breastfeeding.6,22
The incidence of nipple soreness varies according to the definition of pain in different studies and also according to the moment when the data are collected. The results of the cohort study of Buck et al. in Melbourne, Australia with 360 primiparous women found that before discharge 79% of women experienced nipple soreness. 23
In a study by Puapornpong et al., it was found that 9.6% of the 1,649 women followed after the birth suffered from nipple soreness on day 7. 7
To provide effective and early support to women suffering from nipple soreness, first, it is necessary to quantify it through a standardized assessment 24 and the Numerical Rating Scale (NRS) and the Visual Analogue Scale (VAS) are the necessary and most appropriate tools to assess pain in breastfeeding women. 25
In Spain, no data on nipple soreness in the first days postpartum have been obtained through a validated scale; for this reason this research study was carried out with the aim of knowing the prevalence of nipple soreness during breastfeeding at 48 hours postpartum at the Infanta Cristina University Hospital and quantifying it through the VAS to provide adequate support to these mothers.
Materials and Methods
Design
We designed a cross-sectional descriptive study. The purpose was to know the prevalence of nipple soreness during breastfeeding at 48 hours postpartum at Infanta Cristina University Hospital (Madrid, Spain) and, secondary, to identify the variables related with it.
The study was evaluated by the Research Ethics Committee with reference medicinal products of the study hospital (Act no. 02.19) on February 4, 2019 and by the Research Commission of the Faculty of Nursing, Physotherapy and Podiatry of the Complutense University of Madrid, being favorable in both cases.
All measures set out in the Regulation (EU) no. 2016/679 of the European Parliament and of the Council of April 27, 2016 on the protection of natural persons with regard to the processing of personal data and on the free movement of such data, were taken into account and voluntary informed consent was obtained from each mother to participate.
Setting
The hospital where we recruited is publicly funded. In Spain people are assigned a nearby public hospital based on geographical and demographic factors. Of the total population assigned to this hospital (175,000 people), 77,000 are women of childbearing age (between 15 and 49 years old). 26 The average annual number of births in the past 5 years is 1,500.
In this hospital, early skin-to-skin contact is systematically carried out at all births (regardless of the type of delivery), as well as the early start of breastfeeding.
In Spain, to be accredited as Baby Friendly, a hospital must pass four stages. Infanta Cristina University Hospital is currently on Stage 2, so it still is not certified. Efforts are being made to clear Stage 3 soon, by means of a very active breastfeeding support policy and a training program for all health personnel.
Because of this, breastfeeding initiation rate was high (92% of women who give birth initiate breastfeeding).
Data collection took place between 15 February and March 21, 2019.
Sample
Our sample included women who had given birth to a healthy child between 37 and 42 weeks of pregnancy, who initiated breastfeeding within the first 2 hours of the immediate puerperium, and who at the time of discharge has breast milk as its main nourishment even if they had received any infant formula supplements during admission. Mothers with multiple gestations, whose infants weighed <2,500 kg, and those who were diagnosed with ankyloglossia at any time before discharge were excluded. Cases of severe illness of the mother or the newborn that implied a situation of hemodynamic instability for either of the two were also excluded.
A consecutive probability sampling was carried out in such a way that all women who gave birth in the study hospital and met the selection criteria up to the estimated sample size were recruited. The sample size was calculated according to the proportion of nipple soreness in the first postpartum days, because there are no data of this value in Spain and the consulted bibliography showed very dispersed data.6,7,9,12,23,27 To estimate the prevalence of pain, a pilot sample of seven women was taken, with the result that 85% of them experienced pain (in the range of the consulted bibliography). The population was estimated based on births in 2018, which is a total of 1,436, of whom 92% of the women initiated breastfeeding within 2 hours after delivery while making skin-to-skin contact, which means a total of 1,321 postpartum women. A safety level of 95%, an accuracy of 10%, an expected proportion of 85%, and an expected percentage of missing data of 10% were set, resulting in a sample of 53 postpartum women. The sample size was calculated with the GRANMO software. 28
During the collection period there were 127 deliveries, of which 18 possible cases did not meet the selection criteria (1 delivery was preterm before 37 weeks gestation, 4 were twin deliveries, 3 neonates had severe pathology, 1 newborn was diagnosed with ankyloglossia, and 9 women opted for formula feeding), 3 did not want to participate in the study and 48 women could not be interviewed by the team because of various circumstances (discharge early or owing to circumstances arising from care activity). A total of 58 mothers were included in the study on their second postpartum day, 5 more than the calculated sample size.
Measurement
The main variable was the presence of nipple soreness or pain as a dichotomous categorical variable.
Regarding the secondary variables, they were collected in the following way:
The intensity of soreness or pain was measured through the VAS. 29 Using this scale, subjects made a mark on a 10 cm line numbered from 0 to 10, where the left end is absence of pain and the right end is maximum bearable pain. The researcher measured the centimeters up to the mark made by the study subjects. The moment with the highest pain level (start, middle, or end of the take) was also recorded.
Effectiveness was measured using the Lactation Assessment Scale (LATCH),30,31 validated in Spanish 32 and widely used in research. This scale values 5 items with a score of 0–2 each. The maximum score is 10 points and it would indicate adequate breastfeeding and, as the total score decreases, the breastfeeding skills worsens.
In addition, the following information was recorded for each participant: sociodemographic data, personal and obstetric background, personal history deemed, according to bibliography, to possibly be related to nipple soreness such as skin pigmentation, chronic pain, anxiety, breast surgery, and nipple sensitivity during pregnancy, knowledge and expectations that women had during pregnancy about breastfeeding, data about breastfeeding of previous children, if any, and information about breastfeeding of the current newborn. To agree on the questions on these secondary variables, a panel of experts was made up of five professionals with clinical experience and training in the subject.
Data collection
The survey and the two scales were carried out 48 hours after childbirth on mothers admitted to the maternity ward. The women were interviewed in their room. Their informed consent was obtained after explaining the objectives and methodology of the study.
The participants quantified the level of soreness or pain using the VAS and the researchers assessed the LATCH items with the newborn on their mother's breast. The LATCH has high reliability. 32
All participants were identified by a code (ID) that was included as questionnaire identification rather than name.
Data analysis
The survey data were transcribed into a database in the SPSS Statistics 22.0 program. The study ID of each participant was included in this database.
The descriptive analysis was carried out using proportions and number of events for the categorical variables and for the quantitative mean and standard deviation.
A bivariate analysis of the pain VAS score with the secondary variables was performed to detect possible relationships by means of linear regression and one-way analysis of variance test of one pathway, setting a significance level of 5%.
The Stats program used for the analysis was SPSS Statistics 22.0.
Limitations
Because of the design of the study, external validity is compromised by the impossibility of generalizing results and also the impossibility of controlling confounding variables. To minimize confounding bias, all the variables that have been described in previous research that may affect nipple soreness during the first days of breastfeeding were collected.
To avoid interviewer bias, it was verified during team meetings that all research officers had understood the survey and were sufficiently familiar with the questions in the survey. The interviewers were nursing staff from the maternity ward, with ample clinical experience and credited training in breastfeeding.
To minimize attention bias or the Hawthorne effect, the research officers assessed the breastfeeding technique using the LATCH, with the newborn at the mother's breast, without explicitly telling the woman the parameters that were being assessed, so as not to alter the way in which the feeding was carried out.
To reduce procedural bias, the research officers were instructed not to forget to collect all data as well from women who do not present the main variable of the study.
Finally, this same study should be carried out with more participants and in different hospitals to verify that the results obtained in our study can be valid in any center.
Results
Fifty-eight women in their second day of puerperium were recruited in the study. The age of the women were between 19 and 45 years, obtaining an average of 32.7 years (SD = 6.5 years). Sixty-nine percent of women had secondary studies or university studies, and 5.9% had no education; 53.4% of women were Spanish and the rest of them were from 16 different countries.
Personal background is given in Table 1.
Personal Background (N = 58)
Diagnosed with these pathologies before this child's delivery.
Regarding obstetric history, it could be verified that 58.6% (n = 34) of women were multiparous. Average gestational age was 39 weeks and 5 days (SD = 1 week). About 77.6% (n = 459) of births were eutocic births and the rest of them cesarean sections and instrumental vaginal births; In 81% of births, women called for epidural anesthesia; 96.6% (n = 56) of women had skin-to-skin contact with their baby for at least 2 hours. During that time, the skin-to-skin contact was interrupted in the 22% of cases (n = 13).
Regarding the previous knowledge and expectations about breastfeeding before the birth, 51.7% of women said they have received information about breastfeeding through other sources (books, magazines, internet, family, or friends).
They attended antenatal classes during pregnancy, which the national health system offers in a standardized and universal way, to prepare women and their partners for maternity, 44.85% (n = 26) of the sample.
Nine of 10 multiparous women breastfed their previous babies and all of them had difficulty breastfeeding. The most common problem was pain in 43.9% (n = 29), followed by cracked nipples in 36.4% (n = 24), mastitis 13.6% (n = 9), and others 6.1% (n = 4).
About 96.6% (n = 56) of participants stated that, during pregnancy, they intended to breastfeed their future child. Most of the women thought there may be a problem during breastfeeding but it would be easy to solve it, or it would be an appropriate breastfeeding.
The collected data on breastfeeding during the hospital stay are given in Table 2.
Data on Breastfeeding During the Hospital Stay (N = 58)
The prevalence of nipple soreness observed in the sample is 97% (95% CI = 92–100%), being at the start of feeding the moment in which they indicate having more severe pain or soreness by 85.7% (95% CI = 76.5–94.9%).
To assess pain intensity, the VAS was used. It includes values between 0 and 10, with 0 being absence of pain and 10 being maximum pain. Fifty percent of the participants scored the pain between 4 and 6.5 on VAS (mean = 5.1, SD = 2.1).
To objectify the efficacy of breastfeeding, LATCH was used, which presents 5 items with a score of 0–2. The maximum score on the scale is 10 points, which indicates a correction established at lactation. Lower score indicates worse assessment of the lactation technique and possible difficulties. The average score on this scale was 8.2 points (SD = 1.7 points).
It was found that there is a meaningful relationship between LATCH and VAS scores. The higher the LATCH score the lower the VAS score (p = 0.001), as given in Figure 1.
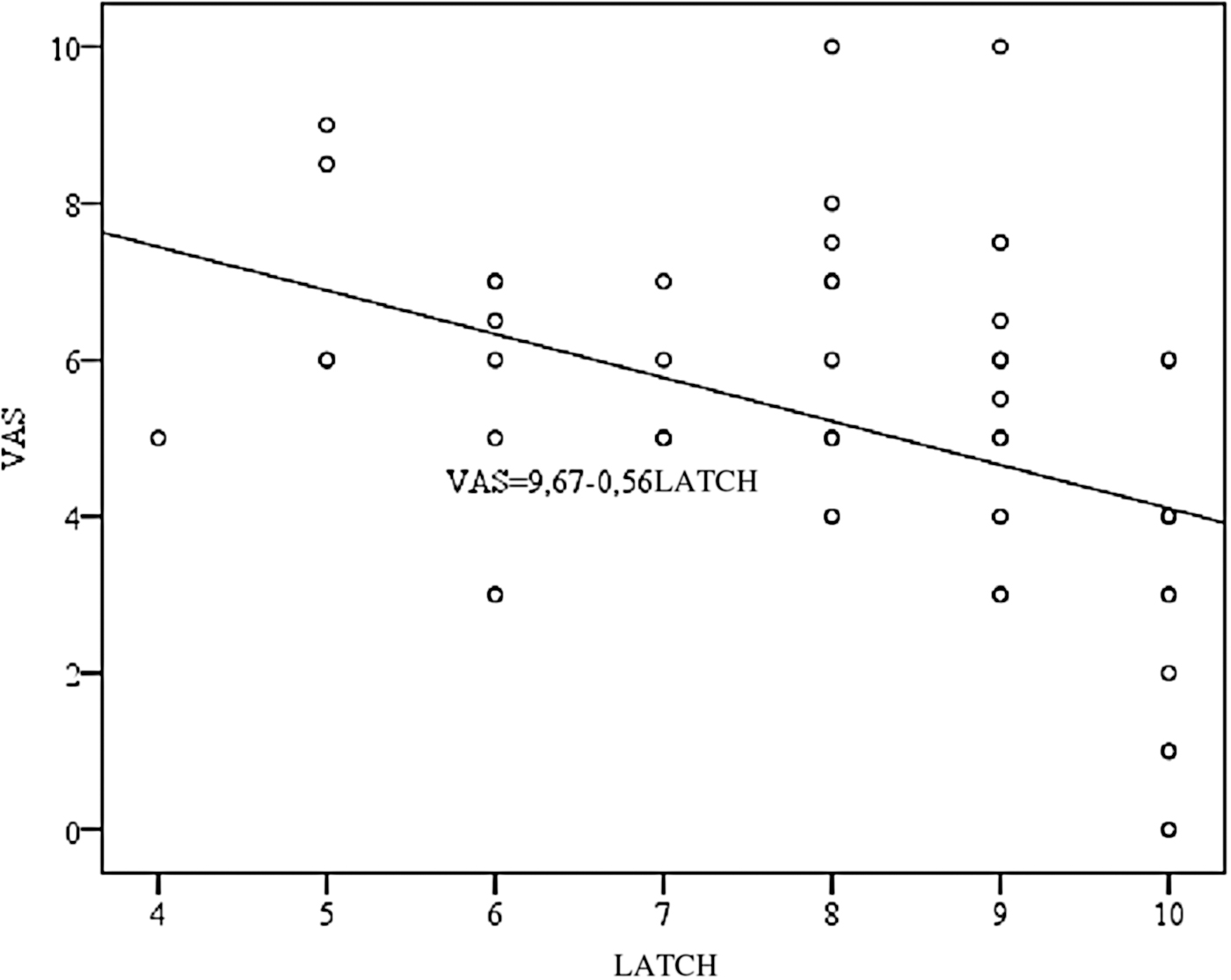
Lineal relationship between the scores of the VAS scale and the LATCH scale. VAS, visual analogue scale; LATCH, lactation assessment scale.
Through a bivariate analysis (Student's t-test), the possible relationships of each of the clinically relevant secondary variables and the pain VAS score was studied. No significant relationship was detected between the parity variable (p = 0.725) and the delivery type variable with pain score (p = 0.292). The results are given in Table 3.
Relationship Between Secondary Variables and Visual Analogue Scale Score (N = 58)
Skin pigmentation (yellow, white, and dark) was recoded into a dichotomous variable (white and yellow or dark).
CI, confidence interval.
Discussion
The prevalence of nipple soreness observed is very high in line with most studies.19,23,27 In contrast, other authors have found lower percentages.6,7,12 This difference could be influenced by the characteristics of health centers where they have taken place, the different definitions of pain that have been used and, finally, the time of postpartum when the measurement is made.
The pain scores obtained using the VAS show a median of 5 points, similar to those obtained by Coca et al. 25 in 2019, in whose systematic review they conclude that the NRS and the VAS can be useful pain scales to use with breastfeeding mothers.
With regard to the assessment of the breastfeeding on the LATCH, it was found in our sample that there is an inverse relationship between the score obtained with this scale and the score on VAS (p = 0.001). This result is in accordance with the literature published to date that indicates that the most common cause of nipple soreness during breastfeeding is inadequate newborn's positioning and latching on to the breast.5–8,33
Although this association between poor breastfeeding technique and nipple soreness has been described, there are other important pain determinants that have not been considered in this study, such as anomaly of palate, insufficient quantity of milk, suspected infection, unusually strong vacuum, or personal history of Raynaud's phenomenon. 6
The emotional state evaluation proposed by Amir et al.'s 2015 Breastfeeding Pain Reasoning Model 34 has not been used in this study. For the evaluation of nipple soreness, this researcher incorporates the assessment of emotional factors that can increase the mother's sensitivity to nipple soreness such as fatigue, lack of social support, social distress associated with loneliness, feeling of rejection, feeling of failure, risk of harm beliefs, anxiety, moodiness, and sleep deprivation.
We have not found any association between attending maternal education classes and pain scores. This could be because of the small sample size. Other researchers have found that earlier problems with breastfeeding were found more often in those women who had not received breastfeeding counseling during the gestation period.8,12,35
In the systematic review on early skin-to-skin contact by Moore et al., 36 the researchers conclude that skin-to-skin contact has numerous benefits for the mother and baby in terms of neonatal mortality reduction, interaction between them, thermoregulation of the newborn, less crying, more likely to be breastfed, and to breastfeed for longer. However, its relationship to nipple soreness is controversial. In our study we found a relationship between women who made skin-to-skin contact with their babies for 2 hours without interruption after birth and a higher pain score (p = 0.046). Similar results have been found by other researchers.8,37 These authors suggest as an explanation that nipple injuries were not associated with breastfeeding in the first hour of life, but rather with poor positioning and latching of the baby in this period.
Even if this study did not record the duration of the first take, investigators suggest that, because the newborns were permanently in skin-to-skin contact with their mothers, they could have made longer first takes, leaving the nipples more sensitive afterward. Those mothers who were separated from their babies could have less or shorter takes, which would put the nipple under pressure for a shorter time and therefore result in less pain. More studies are needed in this regard to be able to draw conclusions.
The lack of association in our study between pacifier use and pain levels is an interesting point because, traditionally, the early use of pacifiers in breastfeeding babies has been discouraged. Current evidence does not support this recommendation and thus WHO/UNICEF has changed step 9 from their 10 Steps for Successful Breastfeeding and no longer explicitly forbid the use of pacifier. 2 The American Academy of Pediatrics recommends using a pacifier during healthy newborn's naps or sleeping periods to decrease the incidence of sudden infant death syndrome. 38
Besides, there seems to persist a general perception among mothers of the benefits of pacifiers. 39 All in all, there should be more studies about early use of pacifiers and its short- and long-term consequences on breastfeeding.
Finally, it has been observed in our sample that women seem to have quite positive expectations regarding breastfeeding. The preconceived idea of smooth breastfeeding meets a different reality when women after delivery encounter painful breastfeeding. This may contribute to an increased risk of postpartum depression. 40 This author proposes specific support for mothers who experience soreness, not only from the perspective of continuing and prolonging breastfeeding but also in supporting maternal well-being. Because the prevalence of soreness is so high, women should receive guidance about it before and after delivery, with better continued support.
Conclusions
The high percentage of nipple soreness detected highlights that breastfeeding can be unpleasant in the first days after delivery. It is important to include in clinical practice the assessment of nipple soreness and the effectiveness of breastfeeding using validated scales to provide adequate support around discharge from hospital. This would prevent possible difficulties, in addition to the early cessation of breastfeeding.
Footnotes
Acknowledgments
The authors thank the maternity department for their support and collaboration in data collection. All the authors acknowledge the mothers and their children for their voluntary participation. The authors thank Jose Enrique de la Iglesia Bautista and Inés Cabañas Engenios for translation support of this article.
Disclosure Statement
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding Information
No funding was received.