
Abstract
Objectives:
To investigate the effect of kinesio taping (KT) and manual lymphatic drainage (MLD) on pain severity, breast engorgement, and milk volume in postpartum women.
Materials and Methods:
In this prospective randomized-controlled trial, we recruited 67 postpartum women who had breast engorgement and randomly assigned them to the KT, MLD, and control group. In the KT group, taping plus breast care was performed, MLD plus breast care was performed in the MLD group, and in the control group, only routine breast care was given for 10 days. Pain, breast engorgement, body temperature, and milk volume were measured. Examinations were repeated on days 1, 4, and 10.
Results:
The MLD group had significant reductions in pain and breast engorgement at all postintervention days compared with the control and KT group (p < 0.05). Milk volume increased among three groups, but the change in the MLD group was higher than in the KT and control groups (p < 0.05). There was no significant difference in the milk volume among the KT and control groups at all postintervention days (p > 0.05).
Conclusions:
MLD relieved breast pain and firmness more and increased milk volume in postpartum women compared with the KT and control groups. MLD can be recommended to postnatal mothers to better manage breast engorgement.
Introduction
Breast engorgement is characterized by interstitial edema, lymphatic and vascular congestion, sudden increase in breast volume, swelling, firmness, and shiny and painful skin. The prevalence of breast engorgement has been reported as 65%.1–3 Studies have reported that poor management of breast engorgement leads to the failure of milk production and mothers may neglect breast care during the early postpartum period. If breast engorgement does not resolve, plugged ducts may lead to mastitis, abscess, and reduced milk production.1–4
The main aim of the management of breast engorgement is to successfully establish and maintain the flow of breast milk, empty the breast milk effectively via the baby or expression, and reduce breast pain.4,5 Current approaches involve a combination of pharmacotherapy such as pain medications, anti-inflammatory drugs, and creams with progesterone and new nonpharmacologic treatments. New treatments such as ultrasound therapy, manual breast massage, use of manual milking techniques, cabbage leaf compression, cold and warm application, manual lymphatic drainage (MLD), and kinesio taping (KT) have no adverse effects, and are thus becoming increasingly popular.1,4,6,7
MLD is manually applied to the skin surface and the anatomic lymphatic pathways of the body are monitored during the process.8,9 Unlike other types of massage, it produces neither blushing nor pain and promotes lymph flow. MLD stimulates the lymphatic system by changing the direction of the accumulated fluid and helps regulate the immune system and cellular functions. Several studies have examined the effectiveness of MLD in these settings.9–12 MLD can be used in pregnancy and with postpregnancy problems such as nipple problems, occluded ducts, and engorgement because it has these properties and can relieve breast symptoms. It was indicated that MLD stimulated lymphovenous and lympholymphatic anastomoses. Also, MLD can enhance angiogenesis, and so, the number of functioning lymphatics can increase, regulate milk flow, and prevent infection development in breast engorgement. 13
KT was developed by Kenzo Kase, 14 and owing to its elastic, water-resistant, and air-permeable structure, the same band can remain on the skin for 3 days.10,11 Some theories were proposed that KT might regulate fascia and soft tissue, reduce tension, increase blood and lymphatic circulation, and relieve pain. It was indicated that KT, which is responsible for the regulation of movements in the fascia and facilitating lymphatic collectors, might relieve engorgement symptoms such as milk ducts, pain, and stiffness.10,11,14
The technique applied in KT is used to help the activation of the lymphatic system, like with MLD. It stays on the body for 3 days, ensuring that this activity is sustained. Therefore, we wanted to compare the effect of these two techniques on engorgement. To the best of our knowledge, no studies have investigated the effects of KT and MLD in postpartum women with breast engorgement. Our aim was to compare the effect of KT plus routine breast care, MLD plus routine breast care, and only routine breast care on breast engorgement among postpartum women.
Materials and Methods
Study design, ethics, and setting
This was a prospective randomized-controlled trial. The study protocol of the study was approved by the Clinical Research Ethics Committee of Karabük University School of Medicine (Decision No: 3/1). Participants were informed according to the Helsinki Declaration. All patients who met the inclusion criteria were invited to enroll in the study.
Sample size calculation
The sample size was calculated using G*Power analysis, based on the results of a previous reference study. According to the reference study results, the investigators had a medium effect size (f = 0.412). 15 For this effect size, when at least 60 persons (at least 20 for each group) were included in the study, that would result in 80% power with a 95% confidence level.
Participants and randomization
Participants who presented to the Department of Obstetrics and Gynecology of Karabük University with symptoms of breast pain and redness, in the early postpartum period (postpartum between 3 and 14 days), and who were referred to the physiotherapy and rehabilitation department of the university were included in the study. The study population comprised women aged 18 years and older; who gave birth at 38–41 weeks of gestation, received breastfeeding training, had acute breast pain, a feeling of heaviness, and engorgement after birth; and who scored themselves as at least level 4 on a six-point self-rated engorgement scale. 4 Patients with gastrointestinal, urogynecologic, autoimmune, and neurologic diseases; breast abscesses or mastitis; those using medical or herbal medication; and subjects with comprehension problems were not included in the study.
A total of 75 subjects who met the inclusion criteria were allocated into three groups using the stratified block randomization procedure with opaque and sealed envelopes containing group allocation numbers obtained from a computer-generated random number table; KT (n = 25), MLD (n = 25), and control (n = 25).
Treatment procedures
In this study, the control group received only routine breast care, whereas the MLD group received routine breast care and MLD, and the KT group received routine breast care and taping.
Routine breast care
The mothers were informed about keeping their nipples moist and instructed in terms of breastfeeding methods by a lactation advisor during rounds conducted in the hospital. The mothers were asked to breastfeed their babies regularly at home every 2 hours and report their breastfeeding data and health situations to the main researcher via the mobile phone application “WhatsApp.” The subjects in the control group were informed that they should not use any other additional strategies to manage breast engorgement until the end of the evaluation.4,15–17 We held in-person meetings with the routine care group on the 1st, 4th, and 10th day at the hospital. We received information on all other days via the phone application.
MLD treatment procedure
In this study, MLD was performed by a physiotherapist (H.D.) who was trained in MLD course by an instructor from the Földi Institute. 18 The subjects were laid in the supine position with their knees bent. MLD started with abdominal lymph drainage, after which central lymph stimulation was performed. Then, by stimulating the bilateral axillary lymph nodes, the flow of fluid over the right and left breasts was directed toward the axillary lymph nodes. While the patients were in the prone position, bilateral axillary lymph nodes were stimulated, and each MLD was performed from the dorsum to the axillary lymph node. Each treatment session lasted ∼45 minutes. After MLD, a moisturizing cream was applied to reduce skin tension. MLD was repeated at the same time of day every day for 10 days from the first day of treatment.8,9,19,20
KT treatment procedure
KT was performed by an experienced and skilled physical therapist (H.D.). Women in the KT group were applied tape, which was to be changed every 3 days from the first day to the tenth day by a physical therapist (H.D.). We applied KT on the 1st, 4th, 7th, and 10th day, and interviewed the women on these days at the hospital. On the other days, we received information by phone. To relieve the tension in the facial tissue, the breast tissue was evaluated with the manual direction test and fascia correction was performed with 25–50% tension and an oscillation movement in the direction we wanted to move the fascia (Fig. 1). In addition, when the facial tension was reduced in the individuals, lymphatic correction was used to increase lymphatic flow. The anchor portion was placed on an area close to the axillary lymph node and the strips were applied with 0–15% tension (Fig. 2).10,14

Fascia correction.

Lymphatic correction.
Evaluations
Evaluations in all groups were performed on the 1st, 4th, and 10th day in the hospital. Demographic characteristics, gynecologic and obstetric history, drug use, heat exchange, skin lesion, breast cystic structure, previous surgical status, nipple cracking, lactation status, and breastfeeding training were questioned.
Increased heat in breast tissue (on skin)
The researcher evaluated the increase in temperature of the patient's breast tissue using the dorsal part of “researcher's” hand with palpation. During palpation, the dorsum of the hands was placed in contact with the breast tissue and the researcher noted any heat and redness. We evaluated the change of temperature increase in the right and left breast separately. Evaluations were repeated on the 1st, 4th and 10th day. The researcher took note of the heat and redness felt in the breast. If there was an increase in heat during palpation, “Yes” was recorded, and “No” was recorded if there was no heat increase.
Body temperature
Each individual's temperature was measured using a digital in-ear body thermometer by the same person three times on the 1st day before treatment, on the 4th day of treatment, and on the 10th day of treatment.
Breast engorgement
The presence and degree of breast engorgement were assessed using a six-point engorgement scale developed by Hill and Humenick in 1994. The six-point scale is a standardized scale. 21 Breast engorgement was graded from 1 to 6. Grade 1 means that the breasts are soft, and the milk flows freely; grade 2 means that the breasts have slight change; grade 3 means that breasts are firm and nontender; grade 4 means that breasts are firm and tenderness is beginning; grade 5 means that breasts are very firm and very tender; and grade 6 means that the breasts are very hard and painful and there is no milk flow. A score of 4 or more indicates the presence of engorgement and the severity is classified according to this scale. Breast engorgement was evaluated three times, on the 1st, 4th, and 10th day. 4
Pain severity score
A visual analog scale was used to evaluate the severity of breast pain. Patients were asked to rate their overall severity of pain between 0 (indicating no pain) and 10 (indicating very severe pain).15,22 Pain severity was evaluated before and after treatment on the 1st, 4th, and 10th day.
Volume of milk expression
A breast pump is routinely given to postpartum women in obstetrics clinics. If breast fullness and heaviness are present, a breast pump is recommended in mothers with engorgement, but not very often. Our reason for using this method was to both relax the mother and to learn the effects of the treatment on milk expression volume. In our study, the breasts were very full and painful, and all mothers with breast engorgement were unable to breastfeed. The total volume of milk expressed from the right and left breasts on the 1st, 4th, and 10th day before and after the treatment was calculated using an electric milking device. Evaluations were repeated on the 1st, 4th, and 10th day within about 4 hours before and after applications. 16
Statistical analyses
All statistical analyses were performed using the SPSS 25.0 software (IBM SPSS Statistics; IBM Corp., Armonk, NY). Continuous variables are expressed as mean ± standard deviation, median (minimum–maximum values), and categorical variables as number and percentage. The Shapiro–Wilk test was used for the testing of normality. If parametric test conditions were satisfied, one-way analysis of variance (ANOVA) was used for comparisons between groups. The post-hoc Tukey test was used when a significant difference was determined in ANOVA. If parametric test conditions were not satisfied, Kruskal–Wallis variance was used for comparisons between groups. The post-hoc Mann–Whitney U test with Bonferroni correction was used when a significant difference was determined in Kruskal–Wallis variance analysis. For pairwise comparisons, the paired-samples t-test and repeated-measures ANOVA were used if parametric test conditions were satisfied, and the Wilcoxon signed-rank test and Friedman test were used if parametric test conditions were not satisfied. The chi-square test was used to compare categorical variables. p < 0.05 was considered statistically significant.
Results
As a result of the power analysis conducted to determine the number of samples to be included in the study, 67 subjects (25 for MLD, 24 for KT, and 18 controls) were enrolled. For right breast stiffness results, we had a large effect size (f = 0.91) with which we reached 99% power with a 95% confidence level.
In this study, the data collected from 67 out of the 75 patients were used. Eight women were excluded from the study; six women in the control group who did not want to continue for personal reasons, one woman in the control group who developed mastitis during observation, and one woman who was sensitive to the band. Sensitivity test was applied to KT group before applying KT. Since a person was determined to be sensitive, she was excluded from the study. Sixty-seven women completed the study (KT group n = 24, MLD group n = 25, control group n = 18) (Fig. 3). All participants were at least high school graduates. The birth week of all babies was between 38 and 40 weeks. There were no significant differences in the demographic, gynecologic, and obstetric characteristics of the subjects in the KT, MLD, and control groups (p > 0.05) (Table 1).
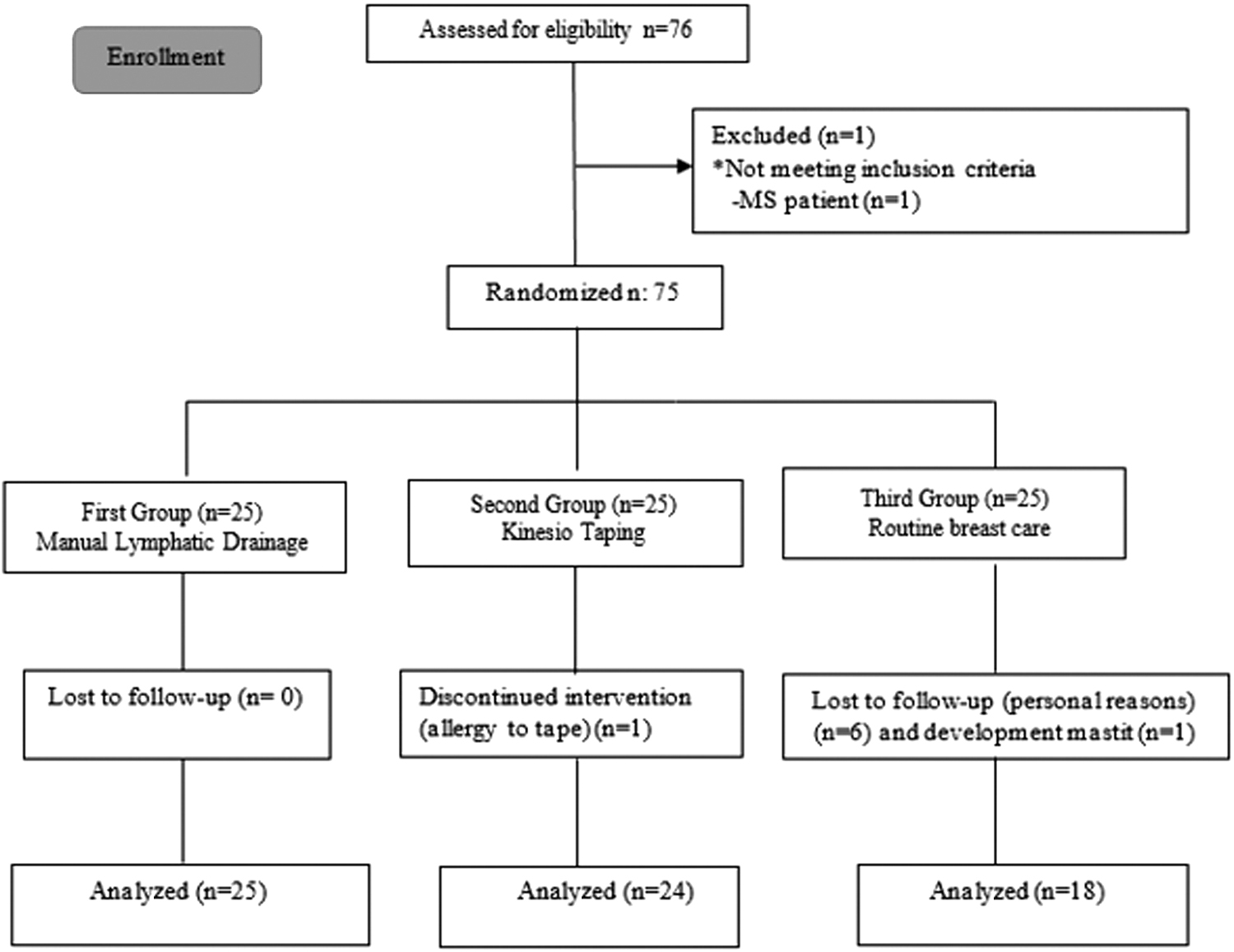
CONSORT flow diagram.
Baseline Characteristics of Participants Who Completed the Study
p < 0.05: statistically significant difference.
BMI, body mass index; KT, kinesio taping; MLD, manual lymphatic drainage; kwh, Kruskal–Wallis variance analysis; mean ± SD, arithmetic mean ± standard deviation; med (min–max), median (minimum–maximum).
Increased heat in breast tissue
There were no differences between the three groups on the first day (before treatment) (p > 0.05). In the MLD group, the temperature increase in both breasts was significantly lower after treatment compared with the KT and control groups. In patients in the KT group, the temperature increase in both breasts was significantly lower after the treatment than in the control group (p < 0.05) (Table 2).
Comparison of Outcome Variables at Baseline Between Manual Lymphatic Drainage, Kinesio Taping, and Control Groups
p < 0.05: statistically significant difference.
BT, before treatment; χ 2 , chi-square test.
Body temperature
When the difference between the body temperature scores of the individuals in all groups was compared, the decrease in body temperature in the MLD group was greater than in the KT and control groups on the 4th and 10th day (p < 0.05). There was no significant difference in the body temperature measurements between the KT and control groups (p > 0.05). Body temperatures of all women in all groups were at normal levels. In addition, the degrees of body temperature after treatment were low in the KT and MLD groups (p < 0.05) (Table 3).
Comparison of Changes in Body Temperature, Breast Stiffness Between Baseline and After Treatment in Manual Lymphatic Drainage, Kinesio Taping, and Control Groups
p < 0.05: statistically significant difference.
Fr, Friedman test.
Breast engorgement
The pretreatment scores on the first day were not significantly different between the three groups (left and right breast) (p > 0.05). In left and right breast examinations on the 4th and 10th day, the degree of engorgement in the MLD group was lower than in the KT and control groups (p < 0.05). The post-treatment left and right breast firmness on fourth day in the KT group was less than in the control group (p < 0.05). In addition, the analysis of breast engorgement for the MLD group, which was measured three times, showed a significant difference over time. In intragroup analysis, the degree of engorgement decreased on the 4th and 10th day in MLD and KT groups (p < 0.05) and the degree of engorgement decreased on the 10th day in the control group (p < 0.05) (Table 3).
Pain severity score
The pretreatment scores on the first day were not significantly different between the three groups (p > 0.05). The decrease in pain intensity after treatment was greater in the MLD group on the 1st, 4th, and 10th day compared with the KT and control groups (p < 0.05). The decrease in pain intensity on the fourth day in the KT group was greater than in the control group (p < 0.05). When the differences in pain intensity changes between the days were compared between the first and fourth days, the difference was greater in the MLD group than in the KT and control groups (p < 0.05). The analysis of breast pain scores showed a significant difference over time for all groups. Breast pain levels in each group were significantly decreased over the study period (p < 0.05) (Tables 4 and 5).
Comparison of Changes in Pain Intensity and Amount of Milk Before and After Treatment in Manual Lymphatic Drainage, Kinesio Taping, and Control Groups
p < 0.05: statistically significant difference.
t, paired-samples t test; z, Wilcoxon signed-rank test; AT, after treatment.
Comparison of Changes in Pain Intensity Score, Breast Milk Between Baseline and After Treatment in Manual Lymphatic Drainage and Kinesio Taping Groups
p < 0.05: statistically significant difference.
(1–2), difference between the 1st and 2nd group; (1–3), difference between the 1st and 3rd group.
Volume of milk expressed
The difference in the volume of milk before and after treatment was greater in the MLD group on the 1st, 4th, and 10th day than in the KT and control groups (p < 0.05). In terms of changes in milk volumes between the days, when the difference in values between the 1st and 4th day, the 4th and 10th day, and the 1st and 10th day was compared, the increase in the volume of milk expressed in the MLD group was greater than in the KT and control groups (p < 0.05). The analysis of the milk volume showed a significant difference over time; the volume of milk expressed in each group was significantly increased (p < 0.05) (Tables 4 and 5).
Adverse events
No adverse effects were reported.
Discussion
This is the first study to investigate the effectiveness of MLD and KT among postpartum mothers with breast engorgement by comparing the effects of MLD plus routine breast care, KT plus routine breast care, and routine breast care only on breast pain, breast engorgement, body temperature, breast skin heat, and breast milk volume. The results showed that MLD plus breast care significantly reduced breast pain, breast engorgement, body temperature, and breast skin heat, and increased breast milk volume more than KT plus routine breast care and routine breast care alone.
Heberle et al. 23 used thermotherapy to investigate heat exchange in women who had engorgement in the postpartum period. They found that breast tissue with engorgement was warmer than in normal women. 23 In our study, our criteria in palpation were redness and increased tactile heat in the breast tissue as felt by the examiners. We found that the redness and sense of heat in the breast tissues were decreased in the MLD group. This may indicate that MLD in particular can remove inflammatory markers faster than taping and breast care alone. In our study, there were differences between the changes in body temperature in the three groups after treatment, with MLD showing the lowest heat level. The normal body temperature of the subjects indicated that they did not have mastitis and that they did not need medical treatment. After the treatment, when the breast was sufficiently emptied after breastfeeding, we measured body temperature and we found that the temperature was decreased on the 1st, 4th, and 10th day. When these results are evaluated, we think that the decrease in body temperature was due to the emptying of the breasts or the effectiveness of the treatment.
Different treatment options need to be developed only if regular breastfeeding and breast emptying are not sufficient to cope with engorgement symptoms.4,6 In this study, in the post-treatment analysis on the 4th and 10th day postpartum, the MLD groups showed the lowest pain level. This indicated that the MLD had been effective in relieving breast firmness. MLD had a calming effect on the patients due to the soothing effect of hands-on therapy and the social interaction with a therapist for 45 minutes on a daily basis. It can be thought that MLD is performed more softly by hand, has a sedative effect, and has a calming effect on patients for 45 minutes daily. In addition, this result showed that with the administration of MLD for ∼45 minutes, the symptoms of women with engorgement will be significantly reduced. By contrast, KT application sessions last only 5 minutes as described in the “Materials and Methods” section, but KT stays in the body for 3 days. As long as KT remains in place, it actively stimulates the tissue. MLD acutely drains fluid in the lymphatic system, and KT helps with drainage, similar to MLD. The positive effects of MLD were greater than KT, both through the calming effect of MLD and with the mechanical removal of inflammatory cells from the body, that is, by the easier flow of milk channels. Our objective findings (such as a decrease in body temperature, a decrease in the degree of the engorgement, and an increase in the volume of milk) in the patients showed that MLD provided lymphatic activation for the engorgement.
Breast pain usually increases on the 3rd–5th postpartum days and continues until the 14th day due to the development of the mammary glands in the breast.2,3,15 With adequate and proper breastfeeding, milk flow is provided and pain decreases. Lim et al. 15 found that the average VAS before cabbage leaf treatment was 0.85 ± 2.03, 1.65 ± 2.87, and 1.35 ± 2.08, respectively. However, in our study, the pretreatment pain severity averages were 8.06 ± 1.06, 8.38 ± 0.68, and 8.41 ± 0.71, respectively. Our pretreatment pain score was higher compared with Lim et al.'s study. 15 Lim et al. 15 included women on the postpartum 2nd day, whereas our study included women on the postpartum 3rd and 14th day. Because our first pain score was higher, the decrease in post-treatment pain scores was more remarkable compared with Lim et al.'s 15 study. However, in future studies, new results can be obtained by selecting patient groups simultaneously.
The greater decrease in pain intensity may indicate that MLD could reduce pain more than applying chilled cabbage leaves. A study directly comparing the effect of these two treatment methods on engorgement pain may yield better results in future studies. Also, Witt et al. 7 used the principles of light massage to activate the lymphatics. They saw a significant decrease in maternal pain and engorgement severity with a one time in-office treatment. Both MLD and superficial classical massage are massage techniques based on touch method. Both techniques reduce pain. However, the pain reduction mechanism of classical massage is based on the postsynaptic inhibition theory in gate control theory. It inhibits pain by creating inflammation and opposite irritation in the painful area. However, MLD reduces the lymph load by clearing the inflammatory markers in the lymph nodes. MLD and KT are methods that can be used in acute cases and reduce inflammation. Both are methods that provide lymphatic drainage and are used. However, classical massage is mostly used in subacute and chronic periods. In MLD application, appropriate paths are followed in the lymph system and they are applications with pressure that will not damage the lymph vessels. The main aim in our study was to remove the inflammation in a short time by decreasing the lymph load in case of acute pain.9,12,18 These two techniques can be compared in future studies to see these differences.
Our results indicated that MLD plus routine breast care, which was applied after the development of breast engorgement, reduced breast pain. KT is thought to be an effective method for relieving breast pain if women cannot come to the hospital every day because it can reduce muscle spasm, connective tissue tenderness, and help lymphatic flow. Routine breast care relieved pain in that it included regular breastfeeding, nipple care by keeping the nipples moist, and several times to milk the breast with a pump. MLD and KT accelerated this process and reduced pain more. The breast pain of women in the MLD group decreased more than in the other groups. Also, analgesic administration was not controlled due to ethical reasons. However, none of the subjects in our study used analgesics, reporting that the painkiller might mix with breast milk and that these nonpharmacologic treatments reduced their pain. This result showed that KT, breast care, and especially MLD treatments reduced breast pain and drug use, and so, alternative treatments could be used in the treatment of breast engorgement before turning to pharmacologic therapies.
We believe that in cases where frequent feeding of the baby does not alleviate the severity of engorgement, methods such as MLD and KT should be used to reduce the patient's need for analgesia and other medications and prevent the use of lactation-suppressant drugs. Our results showed that the increase in the volume of milk expression in the MLD group was greater than in the KT and control groups. This result indicated that MLD plus breast care might increase the release of prolactin faster than the other methods or increase the milk flow in the canals by increasing lymphangion motor activity. By increasing lymphatic activation, MLD accelerated the passage of proteins and reduced the feeling of heaviness caused by milk pressure in the breast.
The greater effectiveness of MLD plus breast care could be attributed to accelerated blood circulation and facilitated faster elimination of metabolic wastes from the body, and transport of oxygen to the muscles. In the literature, it was mentioned that metabolites and inflammatory cytokines rapidly disappeared in blood values even with the acute effects of MLD, which can carry more antigens to the lymph nodes and activate the immune system. Wilson-Clay found that the volume of milk increased, and the feeling of discomfort decreased with MLD in three women who had serious engorgement.8,19,24 In their study, although the number of patients was less than in our study, the effectiveness of MLD was seen. Its physiologic effects include increased contraction of lymphangions, improved collateral lymphatic drainage between the lymphatic regions of the skin, and enhanced angiogenesis.13,20 In this way, the symptoms of breast engorgement decreased faster and the milk flow became easier.
This study had several limitations, including the small sample size, lack of some evaluation methods such as areola diameters of the individuals, edema amounts, breastfeeding periods, supplementation of nutrient quantities, and baby weight. A double-blind, randomized-controlled version of this research was not possible due to the nature of the study. The investigators who implemented the interventions and data collection for pre- and post-treatment readings of breast pain, engorgement, palpation, and body temperature, as well as the patients, were not blinded. The women with breast engorgement in all groups were aware of the treatments they received, and thus, the other limitation of our study was the lack of blinding. Also, the KT plus routine breast care and routine breast care groups did not have daily in-person appointments, but the MLD group had a daily in-person appointment. It is known that touch can have a relaxing effect. There could have been a placebo group to look at the relaxing effect of touch. So, our other limitation is that there was no placebo group to exclude the effect of touch. Our last limitation is that we did not have objective devices such as a durometer, which evaluates the degree of firmness in the breast, and thermography, which evaluates thermal change.
Our data contribute to the literature on the use of new and effective methods for the treatment of engorgement. Wong et al. 4 recommended paying attention to hygiene when preparing cabbage leaves for use. One of their limitations was that some participants might not have fully adhered to the study regimens and also might not have measured the outcomes carefully. Neither MLD nor KT requires active participation. MLD and KT were performed by a trained physiotherapist for 10 days. Postpartum women have to take care of their babies and have pain due to engorgement. Considering this, MLD and KT are attractive for patients and patient feedback indicates that they feel quite comfortable. Future studies should involve standardized daily attention and calming for 45 minutes and evaluate routine breast care with maternal gentle massage of breast toward the armpit. For future comparison, gentle self breast massage or by a family member at home could provide the calming 45-minute effect to help control for the benefit of MLD. In future studies, a comparison can be made for MLD, such as the control and KT groups, once a day or every 3 days. In addition, MLD and self lymph drainage can be compared in women with engorgement in future studies. Also, self drainage and KT or MLD and classic massage can be compared.
Footnotes
Conclusions
In this study, it was observed that there was a decrease in breast stiffness, pain severity, and body temperature, and an increase in the amount of milk in postpartum breast engorgement after MLD, KT, and breast care treatment. MLD relieved breast pain and firmness more and increased milk volume in postpartum women compared with the KT and control groups. KT, MLD, and breast care could improve the quality and efficiency of postnatal health care.
Acknowledgments
We thank the postpartum women who took the time to participate in this study. We took permission for women's photographs.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research did not receive any specific grant from funding agencies in the public, commercial, or private sectors.