
Abstract
Purpose:
This study was carried out to assess the effect of the odor of breast milk and formula milk on reducing the acute pain of newborn infants during the heel-prick blood sampling.
Methods:
Eighty-four newborn were randomly assigned into two groups (formula milk group and breast milk group) with 42 infant searches. The pain that the newborn felt before, during, and after heel-prick blood sampling was assessed using Neonatal Infant Pain Scale; their heart rate and blood oxygen saturation were measured with a pulse oximeter. Saliva samples were taken from newborns before and after sampling, and their salivary cortisol level was measured. During sampling, the crying duration of newborn was recorded with a chronometer.
Results:
The pain threshold and heart rates of the newborn in the breast milk group were significantly lower than those in the formula milk group (p < 0.001). Salivary cortisol in the formula milk group increased and oxygen saturation levels in these infants decreased significantly more as compared to the breast milk group (p < 0.05).
Conclusions:
The odor of breast milk may be helpful in reducing the pain of newborn during heel-prick blood sampling.
Introduction
All newborns are exposed to several painful procedures starting from their birth. Heel-prick blood sampling for diagnosis is one of the most prevalent and painful medical procedures in newborns. Although heel-prick blood sampling is considered to be a simple procedure, its recurrence might take a longer time than normal and may become painful and stressful for newborns due to the reasons like needling the heel, squeezing the heel to get the right amount of blood, changes in the quality of sample, the contamination of the sample, or insufficient amount of sample. 1
An acute pain associated with interventions leads to behavioral stress and physiological changes such as a decrease in oxygen saturation, hemodynamic instability, and an increase in intracranial pressure. These pain-related problems adversely affect the adaptation of newborns to the world outside, their growth and development, and family–infant interaction. To reduce these effects, interventions are recommended to decrease the pain of newborns. 2
Responses to the pain should be evaluated accurately to reduce the pain of newborns effectively and sufficiently. It is necessary that pain measurement tools be multidimensional and include behavioral and physiological variables to identify responses to the pain with appropriate measurement tools and to administer an effective pain medication. Behavioral pain and stress scales, as well as biochemical measurements, are used in the assessment of stress in newborns. In newborns, cortisol is the most commonly used biochemical measurement caused by stress hormones and physiological changes. Cortisol is defined as the biological sign of psychological stress. It has been found that cortisol level in saliva is detectable in the first week of newborn's life, and it is a reliable method to evaluate pain severity and stress levels of newborns. In clinical studies, it has been emphasized that there is a significant relationship between plasma and saliva cortisol levels, and saliva cortisol level indicates plasma cortisol level. Saliva intake is preferred more as it is less stressful for newborn than plasma intake.3,4
Pharmacological and nonpharmacological measurements are used for the control of pain in newborns. Since pharmacological interventions have some undesirable reactions, the use of nonpharmacological measurements has been increasing rapidly. There are studies attempting to alleviate the interventional pain of the newborns using one or more of the sensory stimuli based on newborns' sense of sight, sense of hearing, sense of touch, sense of taste, and sense of smell.5,6
In particular, the olfactory system is more susceptible than the other senses at birth. In a few short minutes after delivery, the head of a human newborn spontaneously turns to the maternal chest and makes a directional leaning toward the mother's nipple to start sucking. There is proof that the odor of newborns' mother, especially maternal milk odor, obviously and positively affects the behavior of newborns. Similar distinction between maternal and nonmaternal odors from the neck, axilla, and whole body of the mother is observed in neonates aged 1–10 days. These results show that newborns are precociously attracted by the body odor of their mother and their mother's breast milk.7,8
Within this context, the odor of breast milk that the newborn is already familiar with can be used to reduce pain and stress in the first days of the newborn's life. The calming effect of maternal odors on newborns has been investigated in several studies recently.9–13 In a study conducted by Marlier and Schaal, newborns were exposed to sniff breast milk and formula milk to evaluate their behavioral responses, breast milk was found to be more attractive by newborns than formula milk, and an increase in their behavioral responses was reported. 11 In a study carried out by Nishitani et al. during heel-prick blood sampling, newborns were exposed to sniff their mother's milk, milk of another mother, and formula milk to evaluate their behavioral responses, and it was found that their mother's milk relieved the pain newborns felt and other odors did not have a calming effect on their pain. 10 In a study by Sajjadi et al., it was reported that the olfactory stimuli in breast milk had a positive effect on reducing the neonatal pain during hepatitis B vaccination. 13 In a study by Badiee et al., preterm newborns were exposed to the odor of breast milk and formula milk during sampling, and the newborns exposed to the odor of breast milk were found to have lower increases in their cortisol levels after sampling compared to the newborns exposed to the odor of formula milk. 12
This study was carried out to assess the effect of breast milk and formula milk odors on the acute pain of newborn newborns during heel-prick blood sampling and to evaluate the effect of those odors on the heart rate, oxygen saturation, duration of crying, and cortisol level.
Materials and Methods
Design
This study was a randomized controlled study conducted on newborns who were hospitalized at the nursery of a pediatric department in a public hospital from March to December 2017.
Sample
The inclusion criteria of the study were: being of a gestational age of 38–42 weeks, having a birth weight of 2,500–4,000 g, an Apgar score higher than 8 at Minute 1 and Minute 5, having no congenital anomaly, having undergone no surgery, not having been administered a sedative or analgesic, not being in condition such as sepsis or requiring mechanical ventilation, not having been treated at the Neonatal Intensive Care Unit, being in stable condition, not having been treated pharmacologically or nonpharmacologically for pain, having been in contact with the mother for breastfeeding at least twice, having been alive for 20 hours, and written consent of family for blood sampling for routine metabolic (phenylketonuria and hypothyroid) screening.
The calculation of the sample size was performed by G-power 3.1.9.2 package program. According to the power analysis, the minimum required sample size was determined to be 80 newborns with the 95% confidence level (the first type of error with the index equal to 0.05) and the 90% study power (the second type of error with the index equal to 0.10). Considering that there could be case losses and cases that could disrupt the homogeneity of the groups in terms of variables affecting pain, 88 newborns were included in the sample.
Initially, 244 newborns were included in the study. However, a sample size of 88 newborns who met the inclusion criteria was required as a result of the calculations. These newborns were randomly divided into two groups (breast milk group and formula milk group) each of which consisted of 44 infants. Numbers from 1 to 88 were assigned into two groups using a program in computer without recurrence of the numbers at randomization. Two newborns from the formula milk group and two from breast milk group were excluded. The final number of newborns in each group became 42, and thus, 84 newborns in total were included in the analysis. The CONSORT flow diagram for the study procedure is shown in Figure 1. 14

CONSORT diagram of this study.
The design of the study is not appropriate for the double blind study since the intervention and assessment were performed by the same researcher. The nurse who assessed neonatal infant pain scale (NIPS) did not know which participant was in which group.
Instruments
Parent-newborn assessment form
Based on the review of literature, the researcher formed 16 descriptive, open-ended multiple-choice questions consisting of the newborn's characteristics of gender, date of birth, mode of delivery, birth weight and length, head circumference, and diet (breast milk or formula milk).15–17
Neonatal infant pain scale
Developed by Lawrence et al. in 1993, the NIPS questionnaire is a reliable, valid, applicable, and comprehensive measurement tool used to assess the degree of a newborn's pain. It consists of the responses to six behavioral indicators such as facial expression, crying, respiration, arm and leg movements, and state of wakefulness (Table 1). 18
Neonatal Infant Pain Scale
Pain level: 0–2 points = No pain, 3–4 points = Moderate pain, >4 points = Severe pain.
Akdovan and Yıldırım adapted the Neonatal Infant Pain Scale to Turkish and tested its validity and reliability.19,20 To detect the inter-rater reliability of NIPS, two independent observers calculated the intraclass correlation coefficient (ICC) indicating the correlation between the NIPS scores obtained during and after the heel-prick blood sampling, under the same circumstances. The ICC was found to be 0.96 before sampling, 1.00 during sampling, and 0.99 after sampling. The ICC score indicating an agreement of 0.75 is considered to be an acceptable level of agreement between the raters more than one. 21
Saliva sampling with SalivaBio Infant's Swabs
SalivaBio Infant's Swabs (SIS) are designed to collect saliva samples from infants younger than 6 months. 22 With the aim of understanding the stress the infants experienced during a painful procedure, saliva samples of all the newborns included in the study were collected 4 minutes before sampling and 20 minutes after sampling.23,24 Cortisol levels were assessed with the saliva samples that had been collected. The samples were collected using SIS. They were collected at least 60 minutes after the infants were fed and before the start of next feeding. The infant's mouth was cleaned first with a sterile sponge (moistened with distilled water) before sampling, which started after a break of 10 minutes.
ELISA reader
The ELISA reader is a device to detect enzymatic events in samples placed on enzymatic and culture plates when enzyme tests are carried out in hospitals or other institutions. 25 The device was used for the measurement of the cortisol level in the saliva samples collected with SIS.
Isolab filter paper
Isolab Filter Paper is a type of filter paper made of high quality cellulose that is resistant to dampness and highly absorbent. It is widely used in general laboratory filtration procedures and for preparing simple samples. 26 In this study, the filter paper was moistened with about 2 mL of breast milk or formula, and 3 minutes before the start of the heel-prick blood sampling, the filter was held to the newborn's nose from a distance of 10 cm so that the newborn could sense the odor. Nine minutes after sampling, the filter paper was removed away from the newborn.
Masimo Rad 5 pulse oximeter
This pulse oximeter is a device that works with Masimo SET technology and is used for making accurate measurements in low perfusion and mobile patients. With its Fast Sat feature, the device is able to track rapid changes in arterial O2 and to make SpO2, pulse rate, and perfusion index readings. The pulse oximeter was placed on the newborn's right ankle before the start of the heel-prick blood sampling. 27
Delta chronometer: SW 305
The Delta Chronometer—SW 305 is a device with wide-scale time and date indicators that provide information in a 12/24 format; it is easy and practical to use and works with a 1.5 V battery. The chronometer was activated at the start of sampling, and the steps of the process were taken one by one. The chronometer was used to set the duration of sampling and the crying duration of the newborn afterward. 28
Implementation of the study
Before the heel-prick blood sampling procedure
The parents agreeing to participate in the study were asked to fill out the Parent-Newborn Assessment Form. On the second day after childbirth, the mother's breasts were milked by hands for 2 hours after breakfast to obtain 2 mL of milk to be sniffed by the first group of newborns. A measuring spoon of powder formula was dissolved in 30 mL warm water to be sniffed by the second group. Two milliliters of this formula milk was drawn with an injector.
Taking the heel-prick sample
On the second day, blood samples were taken from the capillaries of the newborns' heels for a metabolic screening. The heel blood sampling was performed between the hours of 8:00 a.m. and 10:00 a.m. on all the newborns by the researcher. The newborn newborns were fed at least an hour before sampling. To perform sampling, each newborn was taken into a quiet room, kept warm with a radiant heater, and kept away from the crying sounds of the other newborns. Room temperature was set to 23–26°C.
After being brought into the heated space, a pulse oximeter was placed on the newborn's right ankle, and the newborn's heart rate and SpO2 level were recorded before sampling. The device was kept on the newborn's ankle throughout sampling. Afterward, the researcher and a neonatal nurse separately took a NIPS pain measurement. Then the newborn's mouth was cleaned with a sponge and salivary sample was taken using SIS. A minute after the salivary specimen was taken, the filter paper that had absorbed the substance that the baby was to smell was held close to the newborn's nose so that the newborn could sniff it. Three minutes after the filter paper had been held to the newborn's nose, the heel-prick blood sampling procedure was initiated and a chronometer was set to find how long the newborn would cry. Before sampling, the researcher massaged the newborn's heel with her hands and then cleaned the skin of the heel with alcohol. A No. 22G needle point was used to draw blood from all of the newborns. During sampling, heart rates and SpO2 levels were recorded, and the level of pain was assessed using NIPS. The filter paper which was placed near the newborn's nose was removed 9 minutes after sampling. Two minutes after sampling, heart rates and SpO2 levels were recorded, and the level of pain was assessed using NIPS. Another salivary sample was taken 20 minutes after the heel-prick blood sampling procedure. The saliva sampling was performed on all the newborns by the researcher. The sampling procedure took an average of 2 minutes with every one of the newborns.
Calculating the level of salivary cortisol
Salivary cortisol levels were measured using Salimetrics brand (Salimetrics LLC, CA) ELISA Kits. Measurements were taken with these kits using the competitive method. The 96-well ELISA plate is covered with a monoclonal anticortisol antibody. Kit standards are at the concentrations of 3, 1, 0.33, 0.111, 0.037, 0.012, and 0 μg/dL. In addition to the calibrators, there are two level controls at high (0.988 ± 0.247 μg/dL) and low (0.102 ± 0.026 μg/dL). Before the procedure, the saliva specimens stored at −80°C were dissolved at room temperature. Then the vortexed saliva specimens were used without diluting.
The analytical sensitivity of cortisol is 00.007 μg/dL. Its assay range is 00.012–3 μg/dL. While the daily coefficient of variation (CV%) is <7%, the CV% between days is <11%. The reference interval determined for the newborns using the ELISA Kit was <3.417 μg/dL.
Ethics of research
The Ethics Committee of Zonguldak Bulent Ecevit University of Medical Sciences (2017-22-08/02) confirmed the study, and parents' written consent was obtained from all the participants.
Data analysis
SPSS 190.0 program was used for statistical analysis. Mean ± standard deviation (minimum–maximum), number, percentage values, Shapiro–Wilk test, chi-square, Student's t test, Mann–Whitney U test, Repeat Measure Test, Friedman Test, Paired-Samples T test, Kruskal–Wallis test, and Wilcoxon test with Bonferroni correction test were used for the assessment of the data. Results were evaluated in the confidence interval of 95%, and p < 0.05 was considered as statistically significant.
Results
It was found in the study that the parents of the newborns in both groups were similar in terms of age, employment, and educational status, and there was no statistically significant difference between them. The newborns in both groups were observed to be similar in terms of gender, mode of delivery, gestational week, birth weight, head circumference, length, and Apgar score distribution, and there was no statistically significant difference between them.
While no statistically significant differences were detected between the NIPS scores of groups before sampling (p = 0.166), the newborns in breast milk group had lower NIPS scores during (p = 0.001) and after (p = 0.001) sampling compared to the newborns in the formula milk group. At the same time, in both groups, a statistically significant difference was detected between the NIPS scores before, during, and after sampling (breast milk group, p = 0.001; formula milk group, p = 0.001) (Table 2).
NIPS Scores, Heart Rates, and SpO2 Levels of the Newborns Exposed to the Odor of Breast Milk and Formula Milk Before, During, and After the Procedure
Before the transaction.
During the transaction.
After the transaction.
Friedman Test.
Wilcoxon signed ranks test.
Mann–Whitney U test.
Repeat measure test.
Student's t test.
Bonferroni test.
While no statistically significant differences were detected between the heart rates of groups before sampling (p = 0.571), the newborns in breast milk group had lower heart rates during (p = 0.001) and after (p = 0.001) sampling compared to those in the formula milk group. At the same time, in both groups, a statistically significant difference was detected between the heart rates before, during, and after sampling (breast milk group, p = 0.001; formula milk group, p = 0.001) (Table 2).
While no statistically significant differences were detected between the SpO2 levels of the two groups before sampling (p = 0.099), the newborns in breast milk group had higher SpO2 levels during and after sampling compared to the newborns in the formula milk group (p = 0.001). Statistically significant differences were found in both groups of newborns in terms of SpO2 levels before, during, and after sampling (p = 0.001) (Table 2).
The crying duration of the newborns that sniffed formula milk was significantly longer during sampling compared with the newborns sniffing breast milk (p = 0.001) (Table 3). While there were no statistically significant differences between the groups in terms of the salivary cortisol measurements before sampling (p = 0.820), the salivary cortisol levels of the newborns in breast milk group after sampling were found to be statistically and significantly lower than those of the newborns in the formula milk group (p = 0.004) (Table 4 and Fig. 2).
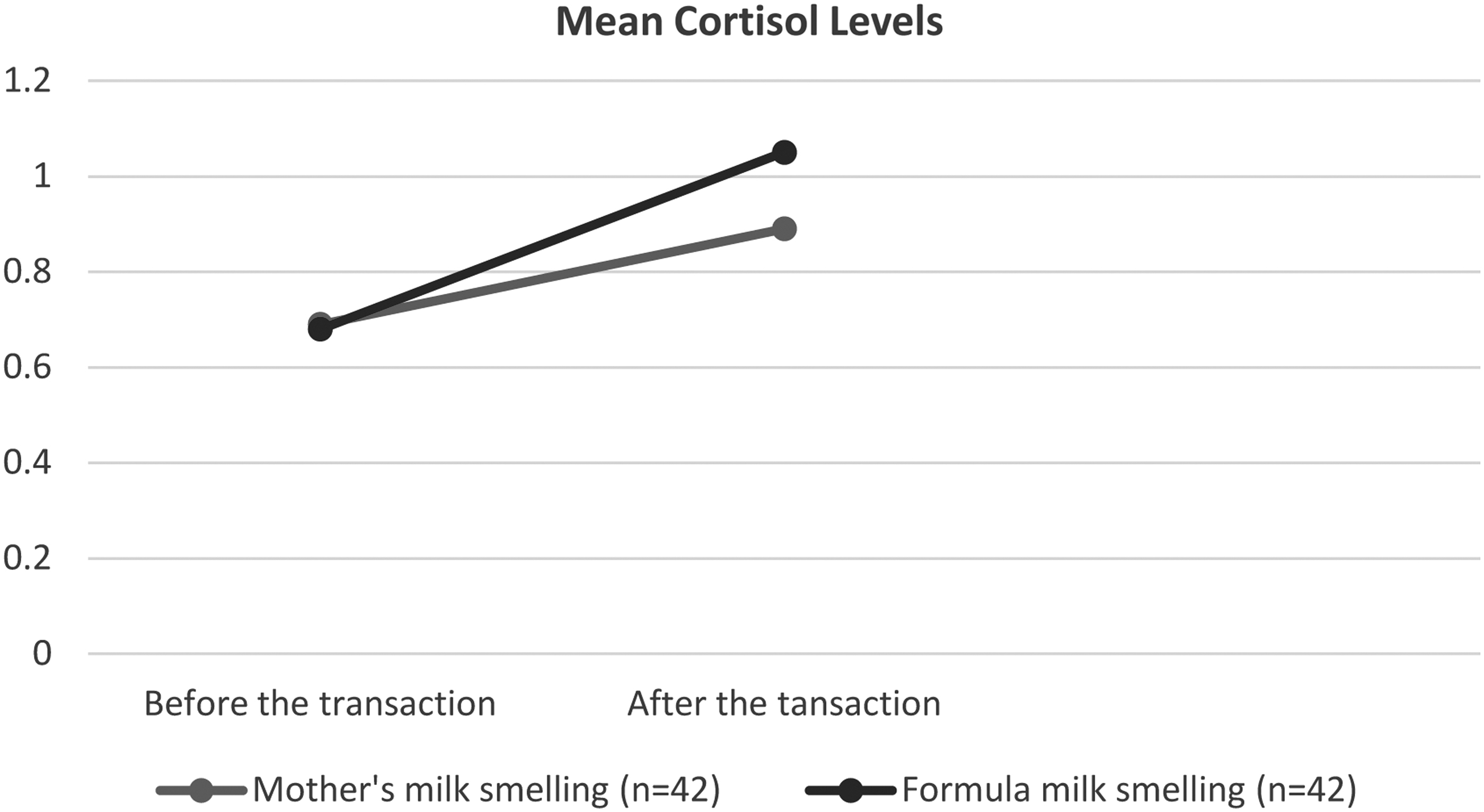
Distribution of cortisol levels of the newborns exposed to the odor of breast milk and formula milk before, during, and after the procedure.
Distribution of Crying Durations of Newborns Exposed to the Odor of Breast Milk and Formula Milk
Mann–Whitney U test.
SD, standard deviation.
Mean Cortisol Levels of the Newborns Exposed to the Odor of Breast Milk and Formula Milk Before, During, and After the Procedure
Wilcoxon signed rank test.
Mann–Whitney U test.
Discussion
The comparison of the NIPS mean scores of the newborns exposed to the odor of breast milk and formula milk in the present study showed no statistically significant differences before sampling. However, after sampling, the NIPS scores of the newborns exposed to the odor of breast milk were observed to be statistically and significantly lower than the scores of the newborns exposed to the odor of formula milk. The results of this study indicated that the odor of breast milk was effective in reducing the pain felt by newborn newborns. Similar to the results of this study, a variety of studies conducted through exposing term newborns to the odor of breast milk and other odors have revealed that exposing the newborn to the odor of breast milk is a useful method to reduce the pain.9,10,13,16,29 In studies with preterm infants, it has been observed that the odor of breast milk reduces preterm infants' pain scores and increases and strengthens sucking.12,30
In the present study, the heart rates and oxygen saturation levels of newborns were assessed before, during, and after sampling performed to draw blood from the heel for the purpose of a physiological evaluation. The increase in the heart rate of the newborns exposed to breast milk was observed to be statistically and significantly lower during sampling compared with the newborns sniffing formula milk. In the comparison of the oxygen saturation levels of the newborns exposed to breast milk and formula, it was detected that the decrease in the level of oxygen saturation during sampling was significantly higher among newborns sniffing breast milk compared to those exposed to the odor of formula milk. The results of the study were similar to the findings of other research on the same subject.16,31 The studies on breast milk and pacifiers and the studies on the odors of breast milk, lavender, amniotic fluid, 16 and sucrose to reduce pain of newborns undergoing invasive interventions have indicated that the increases in heart rates and decreases in oxygen saturation levels are lower in newborns exposed to these methods. 31
One of the most prominent reactions of newborns during invasive procedures is crying. In the present study, the newborns exposed to the odor of formula milk were detected to cry for a significantly longer time during sampling than the newborns exposed to the odor of breast milk. Similarly in some studies, the crying duration of newborns exposed to the odor of breast milk during invasive interventions was reported to be shorter.10,31–33 In the study conducted on newborns undergoing heel-prick blood sampling, Yılmaz and Inal examined the correlation between the crying time of newborns and their method of feeding. The researchers found that breastfed newborns had shorter crying time than other groups. 33
An increase in cortisol levels is another short term effect of the pain. In the present study, while we found no difference in the salivary cortisol levels of the groups before sampling, the salivary cortisol levels of the newborns exposed to the odor of breast milk were statistically and significantly lower after sampling than those of the newborns exposed to the odor of formula. The results of the study were similar to the findings of other research on the same subject.10,12,34 Nishitani et al. conducted a study on term newborns in which the experimental group was exposed to the odor of breast milk, but no exposure to odor was implemented to the control group during a heel-prick blood sampling. A prominent increase was observed in the cortisol levels of the newborns in the control group after the sampling, while no significant increase was observed in the newborns who had been exposed to the odor of breast milk. 10 In the study conducted by Badiee et al., preterm infants were exposed to the odor of breast milk and formula milk during heel-prick blood sampling. The infants exposed to the odor of breast milk had lower increases in their cortisol levels after sampling compared to the infants exposed to the odor of formula milk. 12
Conclusions
The newborns exposed to the odor of breast milk during and after the heel-prick blood sampling felt less pain than those exposed to the odor of formula milk, their stress hormones displayed a less increase on vital signs, their heart rates showed a less increase, and their oxygen saturation levels displayed a less decrease.
Footnotes
Authors' Contributions
T.K.A. designed the study. B.T. collected the data. All authors contributed to interpretation of results and prepared the article. All authors read and approved the final article.
Acknowledgments
The authors thank Professor Murat Can for measuring saliva cortisol levels. This study was prepared as a master thesis. All study participants provided informed consent, and the study design was approved by the appropriate ethics review boards.
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by Zonguldak Bülent Ecevit University Scientific Research Projects Unit No. 201719093093-01.