
Abstract
Background and Objectives:
Feeding of human milk is associated with improved health outcomes in preterm infants. Mothers of preterm infants have difficulty establishing and maintaining an adequate milk supply. Our institution participated in Best Fed Beginnings (BFB), a national breastfeeding quality improvement collaborative, in 2012. Although most practice changes targeted healthy term infants, we hypothesized that mother's milk feeding (MMF) to preterm infants would also improve. Our objective was to compare MMF in very low-birth weight (VLBW) infants at discharge before and after our participation in BFB.
Materials and Methods:
We completed a retrospective chart review of VLBW infants born between January 2006 and June 2016. The primary outcome measure was the percentage of VLBW infants receiving MMF at hospital discharge. We used Fisher's exact test to determine the difference before and after 2012 and performed the Kruskal–Wallis test to determine changes in median time to pump initiation in mothers of VLBW infants. Multiple logistic regression was used to determine variables associated with the primary outcome.
Results:
A total of 1,077 VLBW infants were eligible. After launching BFB, MMF at discharge increased in VLBW infants, from 35.2% to 46.0%, p < 0.001. Median time to pump initiation decreased from 11 to 5 hours after 2012, p = 0.0001. Factors significantly associated with receiving MMF at discharge included birth post-BFB; private insurance; non-Black race; shorter length of stay; older maternal age; and mother's milk as first feeding.
Conclusions:
Hospital culture supportive of breastfeeding impacts not only healthy term infants but also VLBW infants. Earlier initiation of milk expression significantly improves provision of MMF to preterm infants at discharge.
Introduction
Feeding of human milk is associated with improvement in several health outcomes in preterm infants, including a decreased risk of the development of necrotizing enterocolitis and late onset sepsis, and improved neurodevelopment.1–5 However, mothers of preterm infants face multiple challenges in establishing and maintaining an adequate milk supply to meet their infants' needs over a prolonged hospitalization. 6 Although breastfeeding rates have steadily risen in the United States over time, 7 a recent report from the Centers for Disease Control and Prevention (CDC) revealed that the likelihood of receipt of human milk feeding decreased with decreasing gestational age. 8
The Baby-Friendly Hospital Initiative (BFHI) is a global effort aimed at protecting, promoting, and supporting breastfeeding. 9 A facility can be designated Baby-Friendly only after implementing evidence-based practices, the 10 steps to successful breastfeeding, 9 which have been associated with improved breastfeeding initiation and duration.10,11 Although the focus of these breastfeeding practices is primarily on healthy full-term infants, there have been efforts to adapt the 10 steps to meet the needs of infants born prematurely or with other conditions requiring admission to the neonatal intensive care unit (NICU). Two models include Neo-BFHI 12 and the Spatz 10 Steps for Promoting and Protecting Breastfeeding for Vulnerable Infants. 13 In addition, the World Health Organization and UNICEF updated the BFHI guidelines in 2018 to support breastfeeding for mothers of preterm and low-birth weight infants. 14
In June 2012, University of Cincinnati Medical Center (UCMC) sought to improve our hitherto low breastfeeding rates by participating in the Best Fed Beginnings (BFB) program. BFB was a national breastfeeding quality improvement collaborative, targeting facilities located in areas with lower breastfeeding rates and serving populations at highest risk of not breastfeeding. The objective of BFB was to improve maternity care nationally and to increase the number of hospitals designated as Baby-Friendly in the United States.
The primary outcome measure of the project was exclusive breastfeeding rates among breastfed term and late preterm infants not admitted to the NICU. UCMC was 1 of 90 hospitals selected to participate in BFB. We achieved our ultimate goal of Baby-Friendly designation in December 2014 and experienced increased breastfeeding rates in infants not admitted to the NICU. 15 Although the main focus of the project was on the healthy full-term population, we sought to determine if the strong, institutional lactation support that developed during our participation with BFB impacted breastfeeding outcomes in the NICU. Our specific aim was to compare rates of very low-birth weight (VLBW, birth weight <1,500 g) infants receiving mother's milk feeding (MMF) at discharge pre- versus postparticipation in BFB.
Materials and Methods
Study setting
UCMC is a large, urban, academic medical center that serves southwestern Ohio, northern Kentucky, and southeastern Indiana. During the fiscal year of application to BFB (2011), there were 2,352 births; 51% of mothers were Black; 82% of mothers were covered by public insurance; and there were 141 VLBW admissions to the NICU.
The maternity services at UCMC include an antepartum wing, a Labor and Delivery unit, a Postpartum unit, and the NICU. These units are in separate locations on the same floor of the hospital. After delivery, all mothers, once stable, are transferred to the Postpartum unit, including mothers of preterm infants. The nursing staff in these units are distinct and under the direction of the Women's Health Services leadership; however, there are occasionally instances when cross-coverage occurs. We performed a retrospective chart review of VLBW infants born at UCMC between January 2006 and June 2016. This study was approved by the institutional review boards at Cincinnati Children's Hospital Medical Center and UCMC.
Best Fed Beginnings
BFB was led by the National Institute for Children's Health Quality in partnership with the CDC, Baby-Friendly USA (BFUSA), and the United States Breastfeeding Committee. BFUSA provided content expertise and was part of the faculty team of BFB. A learning collaborative model 16 was utilized, such that representatives from similar institutions shared their experiences while individually implementing best practices. The UCMC multidisciplinary team included an administrative leader, obstetrics and neonatal physicians, a mother–infant nurse manager, labor and delivery and postpartum staff nurses, lactation consultants, a Women, Infants, and Children administrator, and a family partner.
The primary objective of the project was to achieve Baby-Friendly designation, and 80% of participating institutions had been designated or had scheduled a site visit upon completion. 17 The main outcome measure was exclusive breastfeeding rates among breastfed term and late preterm infants not admitted to the NICU. There were eight process measures that included prenatal breastfeeding education, assistance and support of breastfeeding, skin-to-skin contact after vaginal and cesarean birth, rooming-in, feeding on cue, and discharge support. Our specific improvement activities at UCMC are detailed elsewhere 15 and followed the 10 steps to successful breastfeeding. 9
Patients
VLBW infants were identified through NICU admission logs. Patients were excluded if the gestational age was >33 weeks or if data were missing for the outcome
Data sources
Data on maternal gravidity, parity, age, insurance coverage, mode of delivery, and the hour after delivery that pumping was initiated were collected from electronic medical records and entered into REDCap, a secure, electronic web-based application for building and managing databases. The following infant data were collected: gestational age, birth weight, first feeding type (mother's milk, donor milk, or formula), MMF at discharge, length of hospital stay, and discharge disposition (discharge, transfer, or death). Infants were considered small for gestational age if the birth weight was less than the 10th percentile for gestational age and gender based on the Olsen curve. Mother's marital status, education, and race/ethnicity were determined from the birth certificate within the infant's medical record. As members of the Vermont Oxford Network, we obtained comparison data for MMF at discharge for the Ohio Perinatal Quality Collaborative (OPQC) subgroup through the Nightingale Internet Reporting System.
Outcome measures
The primary outcome was the percentage of VLBW infants receiving MMF at discharge, defined as receipt of any MMF in the 24-hour period before initial disposition. Secondary outcomes included the pump initiation rate in mothers of VLBW infants; time (in hours) after delivery to initiation of pumping; and type of infant's first feeding (mother's milk, donor milk, or formula).
Statistical analyses
We used Fischer's exact test to determine the difference in the percentage of VLBW infants discharged (on MMF) before and after 2012, the year we began participation in BFB. To calculate the difference in MMF rates comparing pre- and post-2012 periods adjusted for multiple covariates, we used the adjusted odds ratio obtained from a multiple logistic regression model that included race, ethnicity, Medicaid status, maternal age, gravidity, marital status, length of hospital stay, and multiple births.
Multiple logistic regression was used to determine variables independently associated with the primary outcome. We performed the Kruskal–Wallis test to determine changes in time to pump initiation in mothers of VLBW infants and chi-square analysis to determine differences in rates of MMF at discharge between UCMC and OPQC before and after 2012.
Results
Study population
One thousand seventy-seven patients were included in the study. A total of 115 infants were excluded: 21 for gestational age >33 weeks and 94 for missing data (MMF at discharge, n = 70; first feeding type, n = 66; and either of these two variables, n = 94). Maternal and infant characteristics are described in Table 1.
Infant and Maternal Characteristics
The bold represents statistical significance.
SD, standard deviation.
Infants in the cohort had a mean (standard deviation) gestational age and birth weight of 28.3 (2.5) weeks and 1,072 (280) g, respectively, and an average length of hospital stay of 53 (31.6) days. Mean maternal age was 26.9 years (range 14–48), with 35% married, 65% publicly insured, and 40.8% Black. Mothers who gave birth after BFB were more likely to deliver by cesarean section (75.6% versus 69.2%; p = 0.02), older, and publicly insured. Infants were less likely to be discharged home from the NICU after 2012 (p = 0.02) and had a trend toward lower birth weight.
Breast milk feeding at discharge
The proportion of VLBW infants discharged from the NICU on MMF increased from 35.2% before BFB to 46.0% after 2012 (p < 0.001). While the rate of MMF at discharge before 2012 at UCMC was similar to other NICUs within OPQC (35.2% versus 34.4%, not significant), it was significantly greater following our participation in BFB (Fig. 1).
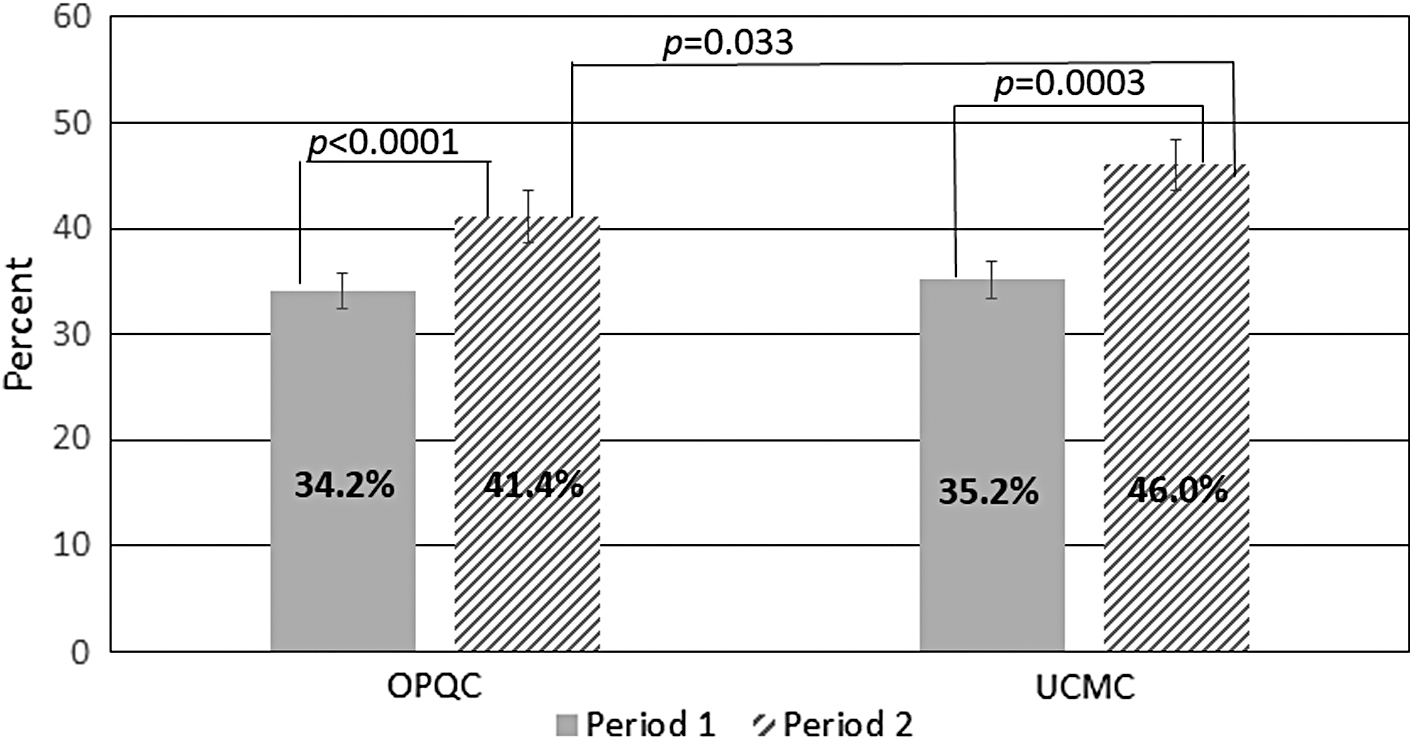
Mother's milk feeding at discharge in very low-birth weight infants, OPQC versus UCMC. No significant difference between OPQC and UCMC in period 1 (2006–2011), p = 0.595. Rates in both OPQC and UCMC increased significantly between periods 1 and 2 (2012–2015 for OPQC and mid-2016 for UCMC). Rates in UCMC increased significantly more than OPQC between periods 1 and 2. OPQC, Ohio Perinatal Quality Collaborative; UCMC, University of Cincinnati Medical Center.
Pump initiation
Overall, most mothers initiated pumping to provide milk for their VLBW infants (90.4%), and this rate was similar at baseline (90.9%) and after 2012 (89.9%) (p = 0.67). However, the median time to pump initiation after delivery decreased after BFB to 5 hours (range 2–69, n = 248), compared with 11 hours before 2012 (range 0–78; n = 398); p < 0.0001.
Variables associated with VLBW infants receiving mother's milk at discharge
VLBW infants were more likely to receive MMF at discharge if their first feeding was their mothers' milk, older maternal age, and if the year of birth occurred before BFB (Table 2). In addition, older maternal age and year of birth before BFB were associated with VLBW infants receiving MMF at discharge. Factors associated with a decreased likelihood of VLBW infants receiving MMF at discharge included a longer length of hospital stay, infants born to unmarried mothers, public insurance coverage, non-Hispanic ethnicity, and multigravidas. Black infants and multiple gestation were each associated with a nonsignificant trend toward not receiving MMF at discharge (p = 0.08 and 0.09, respectively). Both Black and White infants saw increases in MMF rates after BFB, with a slightly higher (but not significant) increase in Black (11.2%) than White (9.5%) infants (Table 3).
Demographic Factors and the Provision of Mother's Milk Feeding at Discharge
MMF, mother's milk feeding.
Multiple Logistic Regression Model of Factors Associated with Very Low-Birth Weight Infants Receiving Mother's Milk Feeding at Discharge (n = 1,044)
R-squared 18.1%.
MMF, mother's milk feeding.
Discussion
We sought to evaluate the impact of strong institutional support on provision of MMF at NICU discharge in VLBW infants. As our facility implemented hospital practices that promote successful breastfeeding, there was a significant increase in MMF at discharge in this population. Although most of the 10 steps to successful breastfeeding 9 target healthy full-term infants (Table 4), applying Step 2 (“Train all health care staff in the skills necessary to implement this [breastfeeding] policy”) required didactic and clinical skill sessions across multiple units, which included the NICU. We suspect that this extensive education laid the foundation to breastfeeding support in the NICU and contributed to the improvements we experienced.
The 10 Steps to Successful Breastfeeding, with Improvement Activities at the University of Cincinnati Medical Center Relevant to Preterm Infants
NICU, neonatal intensive care unit.
Furthermore, we measured our adherence to step 5 (“Show mothers how to breastfeed and how to maintain lactation, even if they are separated from their infants”) 9 by tracking the time to pump initiation following delivery and found a significant decrease over time. In addition to providing staff education on early initiation of milk expression for couplet separation across all units, extra electric pumps and hands-free pumping bras were obtained. This too may have played a role in our success. There is evidence that early breast milk expression is associated with higher milk volumes in mothers of VLBW infants, which could facilitate successful establishment and maintenance of sufficient milk supply over prolonged hospitalization.18,19 For instance, Hoban et al. found that pump-dependent mothers of VLBW infants who achieved milk volumes of ≥500 mL/day within the first 14 days postpartum were significantly more likely to provide MMF at discharge. 20
Although the proportion of VLBW infants receiving MMF at discharge from the NICU was significantly improved, it is important to acknowledge that the majority of VLBW infants in our institution are still not receiving MMF at discharge despite a high initiation rate. It is known that mothers of preterm infants are more likely to experience insufficient milk supply than those of full-term infants, which is a major reason cited for discontinuation of breastfeeding or pumping. 21 The 10 steps target the early phases of lactation, which are critical for successful establishment of lactogenesis. However, our next steps will include strategies that promote maintenance and optimization of sustained milk supply in the immediate postpartum period and earlier identification and mitigation of ongoing challenges for our pump-dependent mothers.
We found that receipt of mother's milk as the first feeding was strongly associated with MMF through discharge. This is consistent with findings from a large, European cohort study that examined factors associated with provision of MMF at discharge. 22 The practice within our institution is to initiate feeding in VLBW infants within 48 hours, so this finding could reflect the impact of early initiation of pumping. Alternatively, it could represent mothers who have an abundant milk supply from early on.
Additionally, there is a relationship between prenatal intention to breastfeed and both breastfeeding initiation and duration. 23 Given our high initiation rate, our experience is that many mothers of VLBW infants change their feeding goal from formula feeding to providing breast milk once they are counseled by our staff, which includes antenatal consults by physicians and postnatal lactation consults. It could be that the early provision of breast milk reflects a stronger commitment to providing MMF. Assessment of prenatal breastfeeding intention was outside the scope of our study.
Significant racial disparities have been reported in many aspects of neonatal intensive care, including MMF. 24 Although national breastfeeding rates have increased over time, Black mothers have disproportionately lower breastfeeding initiation and duration rates. 25 We also identified disparities in the provision of MMF at discharge. Consistent with other studies, we found that demographic factors such as older maternal age and private insurance influenced the likelihood of longer duration of MMF. 26
Infants born to Black mothers in our study were less likely, although not significantly, to receive MMF at discharge. However, the relative percentage increase was higher than in Whites after work with BFB. This suggests that Baby-Friendly designation could be a strategy to narrow gaps between these two groups. Since Black mothers were just as likely to initiate pumping as White mothers, there may be specific barriers in this population to sustaining the milk supply, which need to be addressed.
Strengths and limitations
Our findings are strengthened by the large sample size of this VLBW cohort that examines predictors of provision of MMF at discharge and may be generalizable to other institutions or settings interested in improving their outcomes with respect to breastfeeding. The provision of breast milk at discharge is a highly visible quality indicator of perinatal care, with benchmarking available through the Vermont Oxford Network and the Joint Commission. It is also a national performance metric in ranking neonatology subspecialty in the U.S. News & World Report Best Children's Hospitals. Our results contribute to the evidence base that maternity care practices supportive of breastfeeding are critical to all infants, even the vulnerable population that are unable to experience all 10 steps to successful breastfeeding.27,28
We acknowledge certain limitations to this study. Because this was a retrospective analysis, we cannot rule out the possibility that other practice changes or factors unrelated to BFB may have contributed to improvements in the primary outcome. For example, one intervention that was promoted through our participation in OPQC was the consistent encouragement of kangaroo care, a practice that is associated with improvement in milk supply, 29 and we did see improvement in this measure from 2011 to 2013. On the other hand, the increase in MMF at discharge in VLBW infants at UCMC was significantly greater than what was reported statewide in OPQC, suggesting that our participation in BFB may have played a role. While the crude, unadjusted, 10.8% absolute increase seen in our hospital before and after BFB does not account for shifts in clinical population structure or care practices, after adjusting for multiple covariates, we found that the adjusted difference was higher at 14.6%, strengthening the association. However, we were unable to make similar adjustments for the OPQC MMF rates.
Although there had been long-standing improvement work around the provision of human milk in our NICU, BFB required frequent and formal reporting of our adherence to step 5 (“Show mothers how to breastfeed and how to maintain lactation, even if they are separated from their infants”). Strong leadership support for the improvement work coupled with formal accountability strengthened compliance and gave our efforts more credibility. Furthermore, whereas our previous improvement work tended to be unit specific, Baby-Friendly designation requires institutional transformation that extends beyond the NICU.
This time span of this study included a transition from paper charting to an electronic medical record. Before this change, there were instances of missing documentation. In addition, certain fields were not populated in the chart. For instance, time to pump initiation was not tracked until 2010. Furthermore, we did not measure maternal milk volumes or breastfeeding intention on admission.
In addition, there were some differences in the demographics of the patient population pre- and post-BFB. The infants tended to be smaller and were less likely to be discharged home after 2012, suggesting a population with higher acuity. We suspect that this could be explained by an increasing number of deliveries over time in patients, followed by the Cincinnati Fetal Center, with complex fetal conditions that often require transfer to subspecialty care. In addition, mothers of VLBW infants born after 2012 were more likely to be older, publicly insured, and to deliver by cesarean section. However, older maternal age and delivery by cesarean section are characteristics that are associated with lower milk volumes in mothers of preterm infants, 30 and public insurance may be a proxy for lower socioeconomic status, which is associated with a lower likelihood of MMF at discharge. 31
Conclusions
Institutional support for breastfeeding improves MMF for infants in the NICU as a result of change in attitude, knowledge, and practice of care providers. Prompt initiation of breast pumping is one of the most important factors for improving MMF in the NICU. Given the importance of MMF for VLBW infants, devoting resources and research into sustaining MMF through NICU hospitalization and beyond discharge should be prioritized.
Footnotes
Acknowledgment
BFB was supported by the Centers for Disease Control through the National Initiative for Children's Health Quality (NICHQ).
Disclosure Statement
No competing financial interests exist.
Funding Information
A.L.M. has received a research grant from the Abbott Health and Nutrition Institute and is on scientific advisory boards of Biostime Institute, FrieslandCampina, and Glycosyn.