
Abstract
Objective:
This study aims to examine the effect of labor comfort on traumatic childbirth perception, post-traumatic stress disorder (PTSD), and breastfeeding after the fourth postpartum week.
Methods:
This prospective longitudinal study was conducted between June 2019 and February 2020 in Turkey (n = 102). A personal information form and the Childbirth Comfort Questionnaire were administered to pregnant women with cervical dilatation of 5–8 cm in the delivery room. They were also administered the Traumatic Childbirth Perception Scale (TCPS), PTSD Scale, and Breastfeeding Self-Efficacy Scale twice, including 4 weeks and 3 months after childbirth. Additionally, the TCPS and PTSD Scale were reapplied 6 months after childbirth.
Results:
The prevalence of traumatic childbirth perceptions and PTSD at 4 weeks of the postpartum period was 68.6% and 59.8%, respectively. The multiple linear regression analysis revealed a significant relationship between physical labor comfort (p = 0.003), transcendence (p = 0.023), family history of labor difficulty (p = 0.027), and feelings about birth before labor begins (p = 0.005) and traumatic childbirth perceptions 4 weeks after childbirth. Additionally, there was a significant relationship between physical labor comfort (p = 0.001), psychospiritual labor comfort (p = 0.006), transcendence (p = 0.001), primiparity (p = 0.009), place of residence (p = 0.044), and traumatic childbirth perceptions (p < 0.001) and PTSD 4 weeks after childbirth. Physical labor comfort affected traumatic childbirth perceptions 3 and 6 months after childbirth (p < 0.05). Physical labor comfort affected breastfeeding self-efficacy 4 weeks and 3 months after childbirth (p < 0.05). A significant relationship was also found between high traumatic childbirth perception levels, high PTSD prevalence, and low breastfeeding self-efficacy 3 months after giving birth (p < 0.05).
Conclusions:
Puerperal women had high traumatic childbirth perception levels and PTSD prevalence. Low labor comfort increased traumatic childbirth perception and PTSD prevalence. There was a significant relationship between low labor comfort, high traumatic childbirth perception level, high PTSD prevalence, and low breastfeeding self-efficacy. Therefore, midwives should support pregnant women to increase labor comfort by using alternative methods. Thus, traumatic childbirth perception may decrease and breastfeeding self-efficacy may increase.
Introduction
Holistic labor comfort is achieved by meeting all needs during labor or experiencing individual satisfaction. Kolcaba defined comfort as the immediate experience of being strengthened through having the needs for relief, ease, and transcendence met in terms of physical, psychospiritual, social, and environmental aspects.1–3 If pregnant women report to be satisfied or peaceful, this indicates that they are relieved. If they cope with labor pain and are not afraid of childbirth, they are in a transcendence dimension. 2 Relaxation techniques applied during labor may increase pregnant women's labor comfort levels. 3 A positive childbirth experience is important for postpartum comfort, mother's psychology, and the mother–baby relationship. 4
Birth trauma is defined as an event occurring during the labor and delivery process that involves actual or threatened serious injury or death to the mother or her infant. The mother experiences intense fear, loss of control, discomfort, or vulnerability. Some mothers may feel that their feelings of self-worth are taken away.5–8 The prevalence of birth trauma among puerperal women was reported as 34% in the United States. 9 Post-traumatic stress disorder (PTSD) may be observed in women with traumatic childbirth experiences.10–15 PTSD may develop in response to a traumatic event. Women with difficult or traumatic childbirth are at risk of developing psychological issues that may turn into PTSD.5,16 The DSM-IV criteria group the symptoms of PTSD into three clusters: persistent avoidance of reminders of the event, reexperiencing the traumatic event through nightmares or flashbacks, and increased arousal such as hypervigilance, irritability, and difficulty concentrating. 15 The prevalence of PTSD in women with traumatic childbirth varies between 1.7% and 21%.10–17 Many women with PTSD have difficulties adapting to a new life and coping with normal routines after childbirth. These patients have been reported to have attention deficit, get angry easily, have difficulty making decisions, and often feel very vulnerable. They experience the birth trauma over and over again in their minds and dreams. Additionally, they may develop symptoms such as keeping away from their babies and being reluctant to breastfeed them.5,6,18–20
Low labor comfort and traumatic childbirth perception levels may prevent breastfeeding.21,22 The World Health Organization (WHO) recommends exclusive breastfeeding for the first 6 months of life and introduction of nutritionally adequate and safe complementary (solid) foods at 6 months together with continued breastfeeding up to 2 years of age or beyond. 23 According to the 2018 Turkey Demographic and Health Survey, the rate of exclusive breastfeeding in the first 6 months was 41%, and 71% of the babies were breastfed within 1 hour of birth. 24 Promoting breastfeeding, which improves the bond between the mother and her baby, is important for both the physical and mental health of the public. 22 In 2012, one of the goals of the World Health Assembly was to increase the rate of exclusive breastfeeding in the first 6 months up to at least 50% by 2025. 23 To achieve this goal, the conditions that prevent breastfeeding should be kept in consideration. Stressful and uncomfortable labor, traumatic childbirth, emergency cesarean delivery, birth-related psychosocial stress, and pain are risk factors for delayed lactogenesis.21,22
Labor discomfort may cause perceived traumatic childbirth.5–7 Additionally, breastfeeding may be prevented because increased cortisol levels due to negative labor comfort suppress oxytocin release and decrease milk production. 25 Mothers with traumatic childbirth due to labor discomfort may have difficulty in breastfeeding because of insufficient milk production, physical discomfort, alienation, or emotional detachment problems. 7 In the literature, there are studies that reported that birth trauma and PTSD negatively affect breastfeeding.6,18,21,22,26 However, there is no study on the effect of labor comfort on breastfeeding and the effect of labor comfort on traumatic childbirth and PTSD. Therefore, this study aimed to determine the effect of labor comfort on traumatic childbirth perception, PTSD, and breastfeeding after the fourth postpartum week.
Methods
Design and location of the study
This prospective longitudinal study was conducted between June 2019 and February 2020 in Turkey. For conducting the study, ethical approval was obtained from the Clinical Research Ethics Committee (No. 2019/57) of the Faculty of Medicine in Turkey.
Study sample
A total of 130 pregnant women who agreed to participate in the study, signed the voluntary consent form, planned a vaginal delivery, and had cervical dilatation of 5–8 cm were included in the study. A total of 4,152 deliveries, including 2,223 vaginal deliveries and 1,929 cesarean section (c-section) deliveries, were performed in 2018 at the hospital where the study was conducted. Since the study aimed to include only women with vaginal delivery, the sample size was calculated according to the number of those with vaginal delivery (n = 2,223). Accordingly, the sample size was calculated as 96 using the Epi Info StatCalc program by considering a 95% confidence interval, 0.05 margin of error, and 7%10–13 prevalence of PTSD in women with traumatic childbirth experience. However, the sample size was extended due to possible data losses during and after childbirth. It was not possible to communicate with 28 puerperal women after childbirth. Therefore, the sample consisted of a total of 102 women. The inclusion criteria of the study were having term pregnancy, planning a vaginal delivery, and having a healthy singleton pregnancy. The exclusion criteria of the study were not having term pregnancy, having multiple pregnancies, and not planning a vaginal delivery.
The diagnostic criteria of PTSD in this study were persistent avoidance of reminders of the event, reexperiencing the traumatic event through nightmares or flashbacks, and increased arousal such as hypervigilance, irritability, and difficulty concentrating. 15 The PTSD diagnosis in the pregnant women was made using the Post-Traumatic Stress Disorder-Short Scale (PTSD-Short Scale).
Data collection
A personal information form and the Childbirth Comfort Questionnaire (CCQ) were administered to the pregnant women who were referred to the delivery room and had cervical dilatation of 5–8 cm. Postpartum assessments of childbirth-related PTSD have to be performed at least 4 weeks after birth to meet the diagnostic criteria for PTSD and avoid confounding with acute stress disorder. 15 Therefore, the researchers conducted face-to-face interviews with the puerperal women at their houses 4 weeks, 3 months, and 6 months after they gave birth. The Traumatic Childbirth Perception Scale (TCPS), PTSD Scale, and Breastfeeding Self-Efficacy Scale were applied to the puerperal women 4 weeks and 3 months after childbirth. Additionally, the TCPS and the PTSD Scale were reapplied 6 months after childbirth.
Measures
Personal information form
The personal information form, a survey developed by the researchers, consisted of 28 questions divided into two sections: demographic characteristics and pregnancy-related and obstetric history (Table 1).
Relationship Between Pregnant Women's Sociodemographic and Obstetric Characteristics, Traumatic Childbirth Perception, Post-Traumatic Stress Disorder, and Breastfeeding Self-Efficacy
Bold values: p < 0.05, p < 0.001.
Kruskal–Wallis test.
Mann–Whitney U test.
Independent samples t-test.
Childbirth Comfort Questionnaire
The scale was developed by Schuiling et al. (2011) and its validity and reliability study was performed by Potur et al.2,27 CCQ consists of three subscales (physical, environmental, and psychospiritual) and three specific senses of comfort (ease, relief, and transcendence). This is a 5-point Likert-type scale with 9 items, scored between 1 = absolutely disagree and 5 = absolutely agree. The total scale score ranges between 9 and 45. A higher score indicates higher comfort, or vice versa. Potur et al. found the Cronbach's alpha reliability coefficient of the scale to be 0.75. 27 In this study, Cronbach's alpha coefficient was determined as 0.862. In the study, CCQ was administered once when the pregnant women had a cervical dilatation of 5–8 cm.
Traumatic Childbirth Perception Scale
This 13-item scale was developed by Yalnız et al. to determine the traumatic childbirth perceptions of women. 28 Each item is scored between 0 (positive opinion) and 10 (negative opinion). The total scale score ranges between 0 and 130. A total scale mean score of 0–26 indicates very low, 27–52 low, 53–78 moderate, 79–104 high, and 105–130 very high levels of traumatic childbirth perceptions. This scale was administered four times during the postpartum period, aiming to determine whether there was a change in the women's traumatic childbirth perceptions after giving birth. Yalnız et al. found the Cronbach's alpha internal consistency coefficient of the scale to be 0.895. 28 In this study, Cronbach's alpha internal consistency coefficients were determined as 0.967, 0.983, and 0.981 for measurements performed 4 weeks, 3 months, and 6 months after childbirth, respectively.
Post-Traumatic Stress Disorder-Short Scale (Turkish PTSD-Short Scale)
The Turkish validity and reliability study of the scale was performed by Evren et al. The PTSD-Short Scale is a brief scale that is consistent with the DSM-5 interval criterion for diagnosis of PTSD symptoms in the past 7 days. The items of the questionnaire were adapted to address childbirth as a traumatizing event. This is a 5-point Likert-type scale with 9 items. Each item is scored between 1 = almost never and 5 = almost always. The total scale score ranges between 9 and 45. A higher score indicates a higher likelihood of PTSD (a cutoff score of 24). Evren et al. found the Cronbach's alpha reliability coefficient of the scale to be 0.87. 29 In this study, Cronbach's alpha internal consistency coefficients were determined as 0.998, 0.949, and 0.996 for measurements performed 4 weeks, 3 months, and 6 months after childbirth, respectively.
Breastfeeding Self-Efficacy Scale
The Turkish validity and reliability study of the scale was performed by Eksioglu and Ceber. This is a 5-point Likert-type scale with 33 items. Each item is scored between 1 = not at all confident and 5 = always confident. The total scale score ranges between 36 and 165. A higher score indicates a higher level of breastfeeding self-efficacy. Eksioglu and Ceber found the Cronbach's alpha reliability coefficient of the scale to be 0.91. 30 In this study, Cronbach's alpha internal consistency coefficients were determined as 0.991 and 0.961 for measurements performed 4 weeks and 3 months after childbirth, respectively.
Ethical disclosures
For conducting the study, ethical approval was obtained from the Clinical Research Ethics Committee (No. 2019/57) of the Faculty of Medicine, Balikesir University, Turkey. The pregnant women who agreed to participate in the study were explained the purpose of the study, emphasizing that their identity information would be kept confidential. Written informed consents were obtained from the pregnant women by using a voluntary consent form.
Data analysis
The data were evaluated using means, standard deviations, medians, frequencies, and percentages. The Kolmogorov–Smirnov test was used to assess the normal distribution of data. The Mann–Whitney U test, independent samples t-test, and Kruskal–Wallis test were used to examine the relationships between the pregnant women's sociodemographic and obstetric characteristics, traumatic childbirth perceptions, PTSD, and breastfeeding self-efficacy at the fourth postpartum week. Additionally, the independent samples t-test and analysis of variance (ANOVA) were used to examine relationships between labor comfort, traumatic childbirth perceptions, and PTSD at the fourth week, third month, and sixth month in the postpartum period. Pearson's correlation test was used to examine the relationship between labor comfort and breastfeeding self-efficacy, and PTSD and traumatic childbirth perception. The independent samples t-test and ANOVA were used to examine the relationship between traumatic childbirth perception, PTSD, and breastfeeding self-efficacy at the fourth week and third month of the postpartum period. Multiple linear regression analysis was performed to assess factors affecting breastfeeding self-efficacy, traumatic childbirth perceptions, and PTSD.
Results
The mean age of the pregnant women was 25.94 ± 4.53 years (min. 18, max. 40) and their mean number of pregnancies was 2.09 ± 1.19 (min. 1, max. 6). Table 1 presents the relationship between the pregnant women's sociodemographic and obstetric characteristics, traumatic childbirth perceptions, PTSD, and breastfeeding self-efficacy. The pregnant women living in the city center had significantly higher traumatic childbirth perception levels (p = 0.003) and PTSD prevalence (p = 0.018) than those living in counties and villages. The primiparous pregnant women had significantly higher traumatic childbirth perception (p < 0.001) and PTSD (p < 0.001) levels and lower breastfeeding self-efficacy levels (p < 0.001) than the multiparous pregnant women. The pregnant women with a family history of labor difficulty had significantly higher traumatic childbirth perception (p = 0.001) and PTSD (p = 0.002) levels and lower breastfeeding self-efficacy levels (p = 0.006) than those without a family history of labor difficulty. The pregnant women who considered labor as a difficult and painful process had significantly higher traumatic childbirth perception (p = 0.004) and PTSD (p = 0.001) levels and lower breastfeeding self-efficacy levels (p = 0.003) than those who considered labor as a natural and happy process.
For high traumatic childbirth perception levels, the cutoff score was 79 on the TCPS. For high PTSD prevalence, the cutoff score was 24 on the PTSD-Short Scale. The prevalence of traumatic childbirth perceptions and PTSD at the fourth week of the postpartum period was 68.6% and 59.8%, respectively. Table 2 presents the relationship between labor comfort, traumatic childbirth perception, and PTSD. Accordingly, the pregnant women with high traumatic childbirth perception levels 4 weeks, 3 months, and 6 months after giving birth had significantly lower physical labor comfort than those with low traumatic childbirth perception levels (p < 0.05). Additionally, the pregnant women with high PTSD levels 4 weeks and 3 months after giving birth had significantly lower physical and psychospiritual labor comfort levels than those with low PTSD levels (p < 0.05).
Relationship Between Labor Comfort, Traumatic Childbirth Perception, and Post-Traumatic Stress Disorder
Bold values: p < 0.05, p < 0.001.
Table 3 presents the correlation coefficients for breastfeeding self-efficacy and labor comfort, and PTSD and traumatic childbirth perception. Accordingly, as the physical labor comfort increased, the breastfeeding self-efficacy increased at 4 weeks (p = 0.001) and 3 months (p = 0.019) after giving birth. As the traumatic childbirth perception increased, the PTSD level increased at 4 weeks after birth (p < 0.001).
Correlation Coefficients for Breastfeeding Self-Efficacy and Labor Comfort and Post-Traumatic Stress Disorder and Traumatic Childbirth Perception
Bold values: p < 0.05, p < 0.001.
Table 4 presents the relationship between traumatic childbirth perception, PTSD, and breastfeeding self-efficacy 4 weeks and 3 months after giving birth (Fig. 1). Accordingly, the pregnant women with high traumatic childbirth perception levels had significantly lower breastfeeding self-efficacy levels than those with moderate and low traumatic childbirth perception levels (p < 0.001). Additionally, the pregnant women with PTSD had significantly lower breastfeeding self-efficacy levels than those with low PTSD levels (p < 0.001).
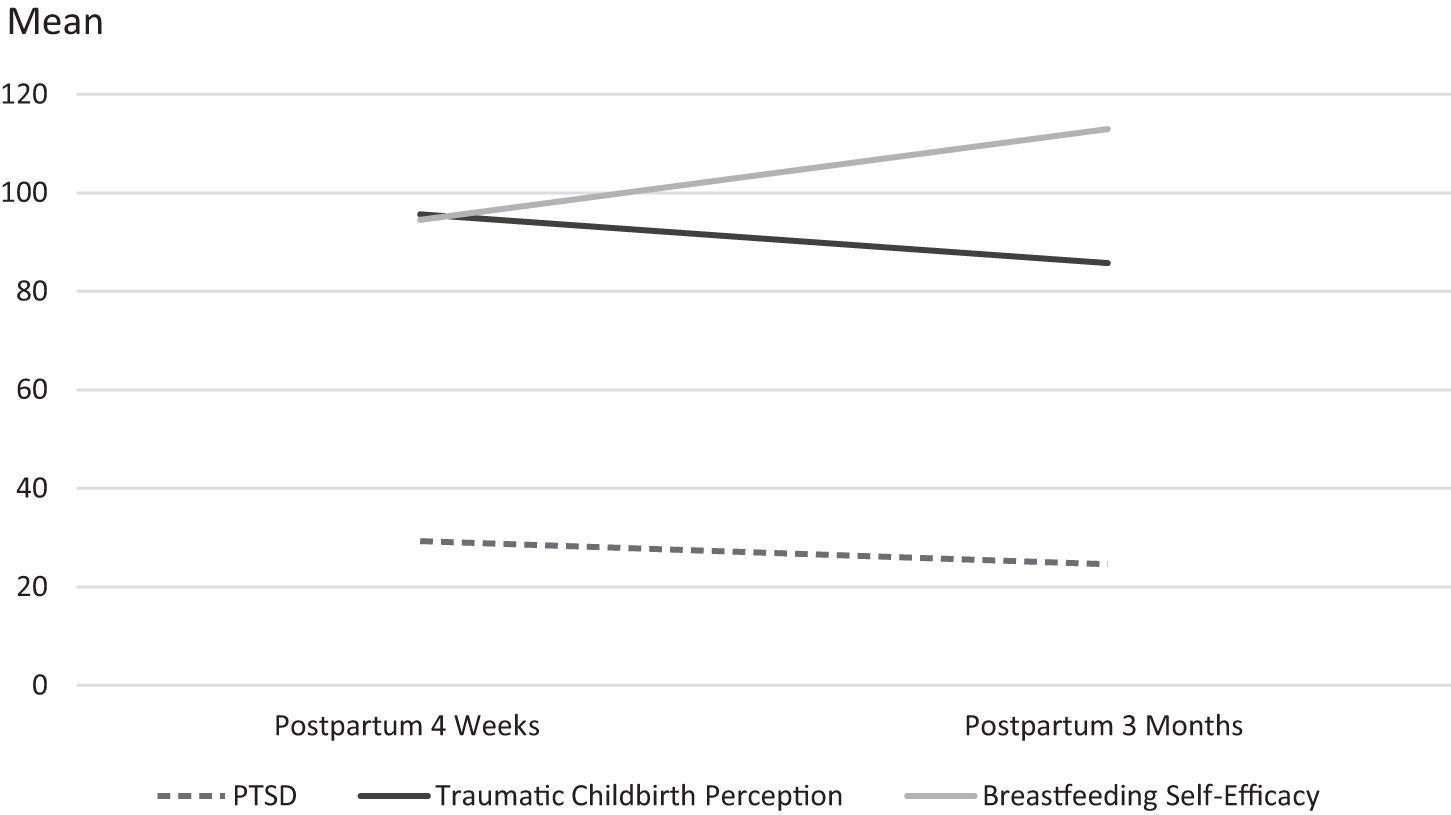
Change in traumatic childbirth perception, PTSD, and breastfeeding self-efficacy 3 months after childbirth. PTSD, post-traumatic stress disorder.
Relationship Between Traumatic Childbirth Perception, Post-Traumatic Stress Disorder, and Breastfeeding Self-Efficacy
Bold values: p < 0.05, p < 0.001.
Table 5 evaluated the factors affecting breastfeeding self-efficacy, traumatic childbirth perceptions, and PTSD with multiple linear regression analysis. Accordingly, models 1 and 2 found a significant relationship between physical labor comfort and breastfeeding self-efficacy after childbirth (p < 0.05). Models 3 and 4 found a significant relationship between traumatic childbirth perception, PTSD, and breastfeeding self-efficacy (p < 0.005). Model 5 revealed a significant relationship between physical labor comfort, transcendence, family history of labor difficulty, feelings about birth before labor begins, and traumatic childbirth perception 4 weeks after childbirth, which explained 32.8% of the variance (R 2 = 0.328) (p < 0.0001). Model 6 revealed a significant relationship between physical labor comfort, psychospiritual labor comfort, transcendence, number of pregnancies, place of residence, traumatic childbirth perception, and PTSD 4 weeks after childbirth, which accounted for 68.1% of the variance (R 2 = 0.681) (p < 0.0001).
Evaluation of Factors Affecting Breastfeeding Self-Efficacy, Traumatic Childbirth Perception, and Post-Traumatic Stress Disorder with Multiple Linear Regression Analysis
Bold values: p < 0.05, p < 0.001.
Model 1. The effect of physical labor comfort on breastfeeding self-efficacy 4 weeks after childbirth.
Model 2. The effect of physical labor comfort on breastfeeding self-efficacy 3 months after childbirth.
Model 3. The effect of traumatic childbirth perception and PTSD on breastfeeding self-efficacy 4 weeks after childbirth.
Model 4. The effect of traumatic childbirth perception and PTSD on breastfeeding self-efficacy 3 months after childbirth.
Model 5. The effect of physical labor comfort, transcendence, number of pregnancies, family history of labor difficulty, feelings about birth before labor begins, and place of residence on traumatic childbirth perception 4 weeks after childbirth.
Model 6. The effect of physical labor comfort, psychospiritual labor comfort, transcendence, number of pregnancies, family history of labor difficulty, feelings about birth before labor begins, place of residence, and traumatic childbirth perception on PTSD 4 weeks after childbirth.
B, regression coefficient; CI, confidence intervals; p, significance value; T, degree of freedom.
Discussion
Childbirth is a versatile experience. Midwifery care contributes to the sense of security, control, personal support, participation in the decision-making process, and labor comfort experience. Childbirth experience may be defined both positively and negatively. Inability to cope with labor pain, lack of sufficient midwifery support, and low labor comfort may cause a negative childbirth experience. This is an important result of childbirth as it has the potential to have a permanent or long-term negative impact on women's lives. 4 In this study, the prevalence of traumatic childbirth perceptions and PTSD at 4 weeks after childbirth was 68.6% and 59.8%, respectively. In the literature, the prevalence of birth trauma was reported as 34% 4 weeks after childbirth 9 and the prevalence of PTSD was stated between 1.7% and 21% 4 weeks–12 months after childbirth.10–17 In these studies, different measurement instruments were used than those used in this study. There has been no study that was conducted with the scales used in this study after childbirth. This study found a higher prevalence of traumatic childbirth perceptions and PTSD than those in the literature. Additionally, this study determined a significant relationship between labor comfort, traumatic childbirth perception, and PTSD. The pregnant women with low physical labor comfort had higher traumatic childbirth perception levels at 6 months after giving birth. The pregnant women with low physical and psychospiritual labor comfort had higher PTSD levels at 3 months after childbirth. The pregnant women with low transcendence at labor had higher PTSD levels at 1 month after childbirth. These results suggested that traumatic childbirth perceptions and PTSD are significantly related to subjective recall of labor experience. In the literature, there is no study on the effects of labor comfort on traumatic childbirth perceptions and PTSD. Studies have reported that women who experience difficult, complicated, stressful, or traumatic childbirth are more likely to have a risk of developing psychological issues that may turn into PTSD.5,17,31,32 In their meta-analysis study, Ayers et al. found a significant relationship between operative delivery, lack of labor support, inability to cope with labor and stress, and PTSD. 16 Hollander et al. stated that physical discomfort and intense labor pain lead to a traumatic childbirth experience. 33 Therefore, health care professionals should determine the level of labor comfort in pregnant women during labor, make interventions to increase their labor comfort levels, minimize traumatic practices at birth, be sensitive to pregnant women's needs, and measure their traumatic childbirth perceptions before hospital discharge. Additionally, health care professionals should follow-up PTSD symptoms in mothers for at least 6 months after childbirth. Depending on the severity of symptoms, they can refer mothers to mental health professionals for psychological support.
In this study, the pregnant women who considered labor as a difficult and painful process had significantly higher traumatic childbirth perception levels than those who considered labor as a natural and happy process. One of the most important causes of traumatic childbirth perceptions is fear of labor. Ayers et al. reported that PTSD was associated with fear of labor. 16 In this study, the pregnant women with a family history of labor difficulty had higher traumatic childbirth perception levels. Zambaldi et al. determined that women with a family history of PTSD are more at risk in terms of traumatic childbirth perceptions. 34 These women were considered to perceive labor as a traumatic event because they were influenced by family stories and therefore they were prejudiced against labor. This study found that pregnant women living in the city center had significantly higher PTSD prevalence than those living in counties and villages. As women living in rural areas can cope better with labor because of being involved in agricultural activities, they have low PTSD prevalence. Additionally, the primiparous pregnant women had significantly higher PTSD levels. Hollander et al. reported that primiparous pregnant women marked high intensity of pain/physical discomfort, long duration of delivery, and discrepancies among their expectations and reality more often and fear for own health/life, a bad outcome, and delivery going too fast less often than multiparous pregnant women. 33 In this study, it was found that as the traumatic childbirth perception increased, PTSD increased. It was reported that among the risk factors that increase the possibility of post-traumatic stress symptoms in the postpartum period is traumatic childbirth experience.32,35,36
This study found that traumatic childbirth perceptions and PTSD levels decreased over time within 6 months of the postpartum period. One study showed that pain intensity and comfort levels experienced during labor are remembered or perceived as less severe over time. 4 Milosavljevic et al. reported decreased PTSD symptoms 3 months after delivery. 37
The most significant reason for low breastfeeding self-efficacy among mothers is lack of a sufficient amount of breast milk production. Stressful childbirth, inability to cope with labor pain, and negative labor comfort increase the cortisol levels, suppressing oxytocin release and decreasing milk production. This may prevent breastfeeding. 25 In this study, as the physical comfort during labor increased, the breastfeeding self-efficacy increased. In the literature, there is no study on the effects of labor comfort on breastfeeding self-efficacy. Some women may have a natural labor expectation and therefore they may feel their body fail in case of a need for medical intervention during labor. Sense of failure reduces labor comfort, in the case of which the woman may not be sure of her body's ability to provide nutrition to her baby and thus her breastfeeding self-efficacy may be negatively affected. 7
Risk factors for delayed or unsuccessful lactogenesis include stressful delivery, birth-related psychosocial stress, and labor pain.7,21,25 This study found that traumatic childbirth perceptions and PTSD negatively affected breastfeeding self-efficacy 3 months after giving birth. When a mother experiences birth trauma, she may have difficulty breastfeeding due to insufficient milk production or physical discomfort (holding the baby, sitting, and finding the right position). 7 In their systematic review, Cook et al. reported a relationship between PTSD and reduced breastfeeding. 18 In their qualitative study, Beck and Watson reported that birth trauma caused unpleasant obstacles restricting women's breastfeeding attempts. 21 Garthus-Niegel et al. and Beck et al. found a significant relationship between postpartum PTSD and the inability to start breastfeeding.14,25 Halperin et al. reported that postpartum PTSD negatively affected maintenance of breastfeeding for 6 to 8 weeks after childbirth. 4 Taghizadeh et al., Dekel et al., and Williams et al. found that women with psychological birth trauma could not bond with their babies and they were reluctant to breastfeed them.19,26,38 Women with postpartum PTSD may have difficulty in interpreting their babies' emotions, making them less sensitive to their needs.7,12 Therefore, health care professionals should observe traumatic childbirth symptoms in the postpartum period, including reluctance to breastfeeding, delayed milk production, discomfort in breastfeeding, and difficulty in holding the baby in the right position for breastfeeding. It should be noted that birth trauma negatively affects both the mother and her relationship with the baby. Women with birth trauma should be referred to breastfeeding counselors. Traumatized mothers may need one-on-one intense support while breastfeeding. In such cases, health care professionals should always seek permission before touching the mother's breasts while helping them breastfeed.
Limitations
This study had some limitations. First of all, the results cannot be generalized to all pregnant women in Turkey. Second of all, this is the first study conducted to determine the effects of labor comfort on traumatic childbirth perceptions, PTSD, and breastfeeding self-efficacy. Therefore, it was not possible to compare its results with those of previous studies.
Conclusions
In this study, labor comfort affected traumatic childbirth perception and PTSD. Health care professionals should determine the level of labor comfort in pregnant women during labor, focus on their needs, and make interventions to increase their labor comfort levels. They should avoid interventional procedures as much as possible to minimize traumatic childbirth perceptions, and they should examine the traumatic perception levels of mothers before hospital discharge. They should also follow-up PTSD symptoms in mothers for at least 6 months after childbirth. Additionally, this study found that labor comfort, traumatic childbirth perception, and PTSD affected breastfeeding self-efficacy. Therefore, it is important for health care professionals to monitor the relationship of mothers, who have undergone an uncomfortable and traumatic childbirth, with their babies. This is because traumatized mothers may need one-on-one intense support while breastfeeding. In such cases, the mothers should be referred to breastfeeding counselors and their relationship with the baby and breastfeeding patterns should be followed for at least 3 months after childbirth.
Footnotes
Acknowledgments
The authors express their thanks to the pregnant women in the sample for participation in the study.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.