
Abstract
Background:
Dicloxacillin is a beta-lactam antibiotic that is commonly used in the treatment of lactational mastitis in breastfeeding women. Although penicillins have long been considered safe for breastfeeding mothers and their infants, there is almost no data on the transfer of dicloxacillin into human breast milk despite the fact that it is commonly used for mastitis.
Case Report:
This study determined the drug concentration-time profile of dicloxacillin in milk samples collected from three lactating mothers consuming 500 mg dicloxacillin taken every 6 hours for treatment of mastitis. Milk levels were measured using liquid chromatography mass spectrometry. The maximum concentration of dicloxacillin in milk was 67.6 ng/mL. The relative infant dose (RID) was calculated to be 0.03%. This value is well below the theoretical level of concern of 10%.
Discussion:
The limited transfer of dicloxacillin into human milk is probably explained by the high plasma protein binding of dicloxacillin and its subsequent poor penetration into human milk.
Conclusion:
In this case series, the level of dicloxacillin in milk was found to be very low, and the RID to be only 0.03% of the maternal dose. Although the levels detected were low, dicloxacillin does transfer into breast milk. Caution should be exercised in infants with hypersensitivity to penicillins.
Introduction
Infectious mastitis occurs in 2–10% of breastfeeding women, often repeatedly, and is cited as a common reason women stop breastfeeding before the infant is 6 months old. 1 Since there is an overwhelming amount of evidence demonstrating the benefits of breastfeeding to mother and the infant, it is important to demonstrate carefully and clearly the safety behind using antibiotics to treat mastitis.
Dicloxacillin is generally considered the first line in the treatment of mastitis in breastfeeding mothers due to its coverage of methicillin-sensitive Staphylococcus aureus. This medication inhibits bacterial cell wall synthesis by binding to penicillin binding proteins. These are essential to the final step of building the peptidoglycan structure used in the bacterial cell wall making the antibiotic bactericidal. A typical dose is 125–500 mg PO every 6 hours for 7–14 days. 2 Less than 10% of patients taking this medication experience some side effects of abdominal pain, diarrhea, nausea, or a hypersensitivity reaction. 3 Dicloxacillin has rapid but incomplete absorption in the gut with poor bioavailability of 49–76%. 3 It is highly plasma protein bound to albumin in the serum (95–99%). It is largely excreted in its unchanged form in the urine with an elimination half-life of ∼0.7 hours. The time-to-peak serum concentration is 1–1.5 hours. This class of penicillins has long been considered safe in breastfeeding women. 4
Although it is commonly used for mastitis, there is only limited information published on the transfer of this drug into human milk at a confirmed steady state. This study describes the drug concentration–time profile in milk, at the steady state of dicloxacillin. Samples were collected over a single dosing interval from three lactating mothers consuming 500 mg every 6 hours for treatment of mastitis. The relative infant dose (RID) estimated in this case series is calculated using average milk concentration (AUC) and the infant dose was divided by the weight-adjusted maternal dose.
Methods and Case Presentation
A total of three patients volunteered to donate their milk samples after administration of dicloxacillin 500 mg taken every 6 hours for treatment of mastitis. Breast milk was donated on or after the fourth day of the antibiotic course, thus was at steady state. Milk samples were collected at 0, 1, 2, 3, 4, 5, and 6 hours after the maternal dose. All the infants had a normal gestational age and weight gain.
Case 1 is a 33-year-old woman weighing 97 kg, breastfeeding her 6-month-old infant. She was taking Synthroid for hypothyroidism and prenatal vitamins. She donated her milk on the seventh day of therapy.
Case 2 is a 34-year-old woman weighing 57 kg, breastfeeding her 1-month old infant. She was also taking flax supplements. She donated her milk on the fourth day of therapy. She missed her hour 5 sample donation.
Case 3 is a 39-year-old woman weighing 75 kg, breastfeeding her 3.5-month-old infant. She was also taking lactase, ranitidine, iron, and vitamin supplements. She donated her milk on the fourth day of therapy. She missed her 3-hour sample donation.
All the participants continued to pump to donate milk samples for this study. To preserve the homogeneity of the samples, the participants were advised to pump both the breasts completely, gently mix them together, and collect one to two ounces into a collection tube. The samples were frozen at −20°C and mailed to our research facility overnight. When the samples reached our facility, they were stored at −80°C until analyzed.
Quantification of dicloxacillin was determined using an Agilent 1260 Quadrapole mass spectrometer. A Phenomenex Luna C-18 column, 50 × 2 mm, 3-μm particle size was used. Isocratic elution was followed using water and acetonitrile with a flow rate of 0.5 mL/min. Single ion monitoring for dicloxacillin at m/z 470 was analyzed. Extraction from milk was accomplished using protein precipitation with acetonitrile. Milk samples containing no dicloxacillin were defined as blank milk, and were spiked with appropriate concentrations of dicloxacillin for determining the calibration curve. All the samples were analyzed in triplicate and described as a mean of values.
Results
The maximum concentration of dicloxacillin in milk (Cmax) was 67.6 (± 12.5) ng/mL and was observed at 4 hours after the dose. The average concentration (Cavg) in 3 mothers' milk was 57.65 ng/mL as described in Table 1. The concentration of dicloxacillin was relatively stable over the 6-hour time course as evident in Figure 1. Derived from the area under the curve, the average concentration (Cavg) was used to calculate the RID. In this case study area under the curve calculated for 6 hours was multiplied by 4 to calculate for 24 hours period of exposure. Based on the assumption of the infant's daily milk intake of 150 mL/kg/day, the infant dose was calculated at 0.008 mg/kg/day. The RID was calculated to be 0.03%, well below the standard theoretical level of concern of 10%.
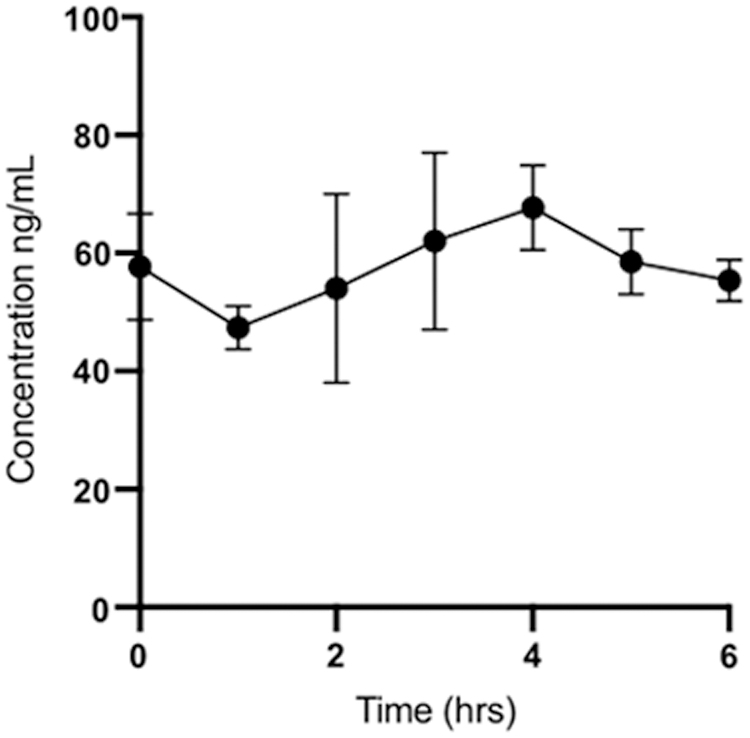
Mean milk concentration-time profile of dicloxacillin after the oral administration of 500 mg taken every 6 hours daily (n = 3). Error bars represent the standard error of mean.
The Pharmacokinetic Parameters of Dicloxacillin in Human Milk Samples (n = 3)
AUC = area under the drug concentration − time curve, Cavg = average drug concentration; Cmax = maximum drug concentration, and Tmax = time at which maximum concentration is observed; RID = relative infant dose.
Discussion
In the one previous report by Matsuda, only the Cmax of dicloxacillin was reported in breast milk. 5 In this prior study, after oral administration of 250 mg dose of dicloxacillin, the maximum milk concentration ranged from 0.2 to 0.3 mg/L between 2 and 4 hours. The drug was undetectable at 1 and 6 hours after the dose. However, the patients were only given one dose of dicloxacillin, were not at steady state, and thus no AUC was reported. In our study, the patients were all at steady state, consuming four 500 mg doses daily, and the AUC was carefully evaluated at one dose interval where the plasma levels were uniform and stable.
Compared with other antibiotics commonly used in the treatment of lactational mastitis, our study found that dicloxacillin had a low RID per day of only 0.03%. In comparison, clindamycin has an RID of 1.36%, cephalexin has an RID of 0.49%, and erythromycin has an RID range of 1.4–1.7%. 6 Thus, all of these antibiotics are well below the theoretical level of concern (RID of <10%). 7 Other studies have reported that antibiotics may produce slight changes in gut flora, so it is important to monitor for GI disturbances, particularly diarrhea, candidiasis, and skin rash in the breastfeeding infant.
The limitations of our study included small sample size and lack of corresponding infant blood samples. Considering the benefits of breastfeeding and the importance of having a properly treated infection, dicloxacillin should be considered safe to use in breastfeeding women with close monitoring and precautions.
Conclusions
This case series on three lactating mothers adds to the body of evidence, suggesting a clinically insignificant transfer of dicloxacillin into milk. The RID per day for dicloxacillin is 0.03% and there is a low risk of infant toxicity. However, additional studies are required to verify our findings and to document any effect of dicloxacillin on breastfeeding infants. We recommend that the infant be monitored for issues such as gastrointestinal side effects and hypersensitivity reactions.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.