
Abstract
Objective:
Cesarean section rates are increasing in developed countries and could be performed as an emergency or elective procedure. Our research aim was to determine whether elective cesarean section influences the melatonin content, the main circadian hormone, in human milk.
Methods:
Twenty-one women after vaginal delivery and 18 women after elective cesarean section were included. Only healthy mothers with normal newborns exclusively breastfed were recruited. Two samples of human milk were collected for each woman at three stages of lactation: colostrum, transitional milk, and mature milk; at each stage, one daytime sample and another nighttime sample were obtained. In total, 228 milk samples were studied. The melatonin content was analyzed by enzyme-linked immunosorbent assay.
Results:
Melatonin rhythmicity with higher melatonin content at night was maintained at each of the three stages of lactation, regardless of the type of delivery. A higher melatonin content was found in daytime colostrum after cesarean section with respect to colostrum obtained from mothers after vaginal delivery (30.3 pg/mL versus 14.7 pg/mL, p = 0.020). Melatonin content decreased progressively throughout the course of lactation in both groups. This decrease was significant when comparing transitional milk to colostrum in the cesarean group, both in the daytime (p = 0.016) and nighttime samples (p = 0.048).
Conclusions:
Cesarean section is associated with an increase in daytime colostrum melatonin. No difference was observed in mature milk with respect to vaginal delivery. Melatonin values in human milk decrease during the first month of lactation and circadian rhythmicity was observed irrespective of the mode of delivery.
Introduction
Parturition is initiated by hormonal modifications at the end of gestation. A complex interaction network between steroids, vasoactive agents, prostaglandins, inflammatory cells, and the release of chemokines upregulates contraction-associated proteins and further facilitates transformation of the uterus from rest to contractile phenotype. Therefore, parturition is also an inflammatory process. 1
Vaginal delivery is the natural mode of birth in mammals. However, when there is a risk for the mother or the baby, a cesarean section should be performed. Emergency cesarean section is performed when the risk is imminent, but elective cesarean section can be indicated when a risk is presumed. In this case, the surgery will be scheduled, and the mechanisms involved in normal parturition may be absent. However, performing this procedure may have short- and long-term implications for the baby. 2
Human milk is the species-specific food for newborns. It is a highly specialized nourishing and functional substance with a dynamic nature. Many components in this fluid exert beneficial effects on the baby. Some of these components are currently under research. One of these components is melatonin, the main hormone involved in circadian rhythms in vertebrates, and an indolamine secreted mainly by the pineal gland. Melatonin is a highly diffusible molecule whose receptors are ubiquitous in human organisms. 3 It is under the influence of the night/day cycle from the retinohypothalamic tract and suprachiasmatic nucleus. Thus, melatonin secretion reaches its highest levels during the night, whereas it is very low during the daytime.
Outside of its influence on the sleep-wake state, melatonin has several other human physiological implications; it is a powerful antioxidant and has immunomodulatory effects.4–7
The fetus does not secrete melatonin until 9–15 weeks of age. Levels increase to the third trimester of gestation and drop down after parturition.8,9 However, a mature circadian rhythm and response to the light/dark cycle develops later, at ∼2–3 months of life. 10 Thus, human milk is the only melatonin source in the perinatal period, and the infant melatonin level depends in this period on the circadian melatonin rhythm of the mother.11,12 There are few studies about melatonin in breast milk early after birth and the evolution of melatonin levels during the lactation period under normal conditions. Furthermore, some investigations suggest significant differences in pineal melatonin secretion after cesarean section with respect to vaginal delivery,13,14 but the distinction between emergency and elective cesarean section has not been evaluated.
We hypothesized that breast milk melatonin content can be affected by the mode of delivery in the case of elective cesarean section. In this sense, the goal of this study was to assess the differences in breast milk melatonin levels in mothers who underwent elective cesarean section with respect to mothers who had a vaginal delivery and to determine the evolution of breast milk melatonin levels over three periods of lactation: colostrum, transitional milk, and mature milk.
Materials and Methods
A prospective longitudinal study was designed to compare melatonin content in human milk from two cohorts of healthy pregnant women based on mode of delivery at term: vaginal delivery or elective cesarean section. The study was approved by the Institutional Committee for Ethics in Research of the Hospital, and all the women gave informed written consent before participating in the experimental protocol.
The study took place at the Department of Pediatrics, Obstetrics and Gynecology of Hospital Quirón, a secondary hospital in Valencia, Spain. Participants were enrolled before parturition, between January 2017 and May 2018. The global cesarean section rate was 30% during the mentioned period. Skin-to-skin after birth was routinely practiced in all cases, including in the operating room, and the kangaroo method was favored during their hospital stay. The exclusive breastfeeding rate at home discharge was 96.8%. All women received individualized advice and follow-up on breastfeeding from the first day after delivery to home discharge by an International Board Certified Lactation Consultant. After discharge, women received telephone follow-up the first week after delivery.
Only healthy women who met the following inclusion criteria were recruited: gestational age at delivery between 37 and 41 + 6/7 weeks; gave birth, either by vaginal delivery or by elective cesarean section, to a strictly healthy infant with APGAR test scores of 9/10 at 1 minute; negative serological reactions for hepatitis, human immunodeficiency virus, and syphilis; full prenatal health care was received; no special diet during pregnancy; and signed the informed consent form. The exclusion criteria were as follows: gestational diabetes; twin pregnancy; and fetal malformations or any kind of perinatal situation with a high risk of oxygen stress for the babies or mothers (preeclampsia, emergency cesarean section, neonatal resuscitation or asphyxia, intrauterine retardation in growth, or acidosis in the newborn). Newborns who received any cow's milk supplementation were also excluded.
All mothers either of vaginal delivery or cesarean section received epidural anesthesia. Elective cesarean section was indicated for mothers who had a previous cesarean section, persistent breech presentation, or suspected cephalopelvic disproportion.
The sample size was calculated while using the standard deviation of the peak nocturnal melatonin secretion found in breast milk from healthy mothers 14 as a reference for a minimal expected precision of 10 pg/mL and an alpha level of 90%. The sample size necessary was 20 patients per group. In total, 44 women were included in the study. Six participants were lost during the follow-up because they did not attend the scheduled visits. The data analysis was thus undertaken in 38 women. According to the type of delivery, 21 had a vaginal delivery and 17 had a cesarean section.
Obstetric characteristics of the pregnant women and newborns were obtained by personal interviews and medical reports (Table 1). Milk samples were collected at three different stages of lactation: colostrum (first 24 hours after birth), transitional milk (from third to 7 days after birth), and mature milk (1 month after birth). Due to known physiological rhythmicity in melatonin secretion, two samples were collected from each mother: one daytime sample (collected between 12 pm and 2 pm) and one nighttime sample (between 12 am and 2 am), at the three different stages of lactation. Overall, six milk samples were collected from each woman. Two hundred twenty-eight milk samples were analyzed: 126 milk samples from mothers who had vaginal delivery and 102 milk samples from mothers who underwent a cesarean section.
Characteristics of Study Population
Data are expressed as median (interquartile range) or number (percentage).
Calculated by Wilcoxon rank sum test for quantitative variables and chi-square test for categorical variables.
All the samples were collected by manual extraction or after electric-pump expression (MEDELA Swing pump. McHenry, Illinois, USA) under appropriate hygienic conditions. The samples were extracted under dim light exposure (<30 lux) and collected in containers covered with light protection paper until defrosting. They were kept at −20°C for a maximum of 48 hours to be later transferred cold to the laboratory of the University of Valencia, where they were stored frozen at −80°C until processing.
The duration of hospital admission in women who had a vaginal delivery was at least 48 hours after delivery. In the women who underwent cesarean section, the minimum duration of admission was at least 72 hours after the procedure. Therefore, the colostrum samples were collected by women with the help and supervision of an International Board Certified Lactation Consultant during their hospitalization. The women were trained in the extraction of human milk, protection of the sample from light, and storage of the sample in the freezer at home. Material for cold transport was delivered to the mothers so that the transitional and mature milk samples could be transported to the laboratory.
Melatonin content in human milk (pg/mL) was measured by using the standard enzyme-linked immunosorbent assay (ELISA) kit (DRGMelatonin ELISA-EIA-1431; DRG International, Inc., Springfield, NJ, USA). All procedures were performed according to the manufacturers' instructions after the samples were defrosted completely. Cream and milk fat globules were separated from the milk using delipidation centrifugation at 1,500 rpm. Delipidated breast milk (100 μL) was incubated together with primary antibody and TMB buffer substrate solution under darkness conditions and centrifuged at 500 rpm for 3 minutes. Colorimetric readings of absorbance were carried out using VICTOR Multilabel Plate Reader plates (Waltham Massachusetts, USA) to 450 nm versus filter control to 595 nm.
Statistical analysis
Statistical analysis was performed using SPSS 22.0 (SPSS, Inc., an IBM Company, Chicago, Illinois, USA). Due to the asymmetrical distribution of the sample, nonparametric tests were used. Median and interquartile range were used to describe the data.
To check the physiological rhythmicity of melatonin secretion, the comparison of melatonin content in human milk samples between daytime and nighttime was performed. Differences in human milk melatonin content depending on the type of delivery were also evaluated. Furthermore, to study whether human milk melatonin content evolves differently throughout the course of lactation according to the type of delivery, variations in the melatonin content in transitional and mature milk with respect to the melatonin content in colostrum were compared between mothers who had a vaginal delivery and mothers who underwent elective cesarean section.
Wilcoxon signed rank test was used for comparisons intragroup and Wilcoxon rank sum test for comparisons intergroup (vaginal vs cesarean). A p-value <0.05 was considered significant.
Results
Human milk melatonin rhythmicity
Compared with daytime milk, the concentrations of melatonin were significantly higher at night. Difference in the values of melatonin content between day and night are shown in Table 2. Higher melatonin content in all nocturnal samples of colostrum, transitional milk, and mature milk was found in both the vaginal delivery group and cesarean section group. Thus, melatonin rhythmicity in breast milk through the 24-hour cycle is maintained, regardless of the type of delivery.
Night-Day Difference in Melatonin Content (pg/mL) According to the Mode of Delivery
Values expressed as median and interquartile range.
For comparisons intragroup in vaginal delivery, calculated by Wilcoxon signed rank test.
For comparisons intragroup in cesarean section, calculated by Wilcoxon signed rank test.
For comparisons intergroup, calculated by Wilcoxon rank sum test.
Human milk melatonin content
In general, the melatonin content of human milk was higher in colostrum than in the other stages of lactation following both vaginal delivery and cesarean section. More melatonin content in daytime colostrum was found in samples from mothers who had cesarean sections with respect to colostrum obtained from mothers after vaginal delivery (p = 0.020). Although the human milk melatonin content was higher at every lactation period studied in the cesarean section group, no significant differences were found in transitional or mature milk with respect to vaginal delivery (Table 3).
Melatonin Content at Three Different Stages of Lactation According to Mode of Delivery
Values are expressed as medians and interquartile range.
Calculated by Wilcoxon rank sum test.
Evolution of human milk melatonin content during lactation
Melatonin content decreased progressively throughout the course of lactation in both groups. No differences in the evolution of the melatonin content of human milk were found between the two groups during the first month of lactation. However, a significant decrease in the content of melatonin in transitional milk compared to colostrum, both in diurnal and nocturnal samples in the cesarean section group, was found (p = 0.016 and p = 0.048, respectively) (Fig. 1). No significant decrease in melatonin content in transitional milk versus colostrum after vaginal delivery was found. Thus, the mechanisms involved in the increase of melatonin content in colostrum in the milk of mothers after cesarean section are related to the mode of delivery.
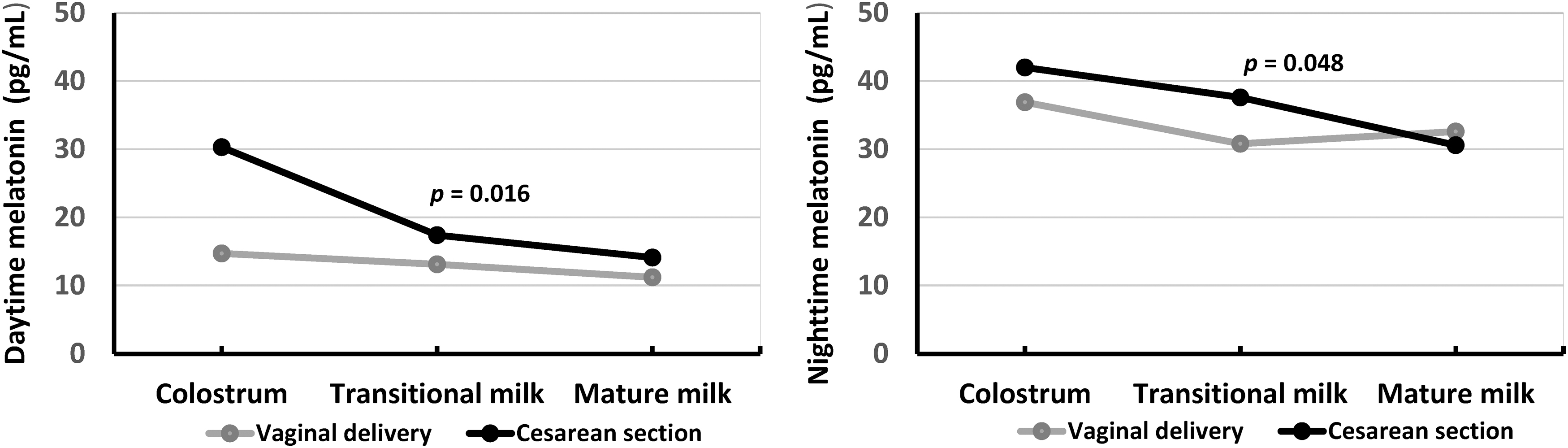
Evolution of melatonin content in human milk during the first month of lactation according to the mode of delivery. Significant difference was found between colostrum and transitional milk in caesarean section (p = 0.016 in day samples and p = 0.048 in night samples).
With respect to the evolution of melatonin content in the first month after birth, no significant differences were found between vaginal delivery and elective cesarean section in mature milk obtained at one month of lactation.
Discussion
The main results of this study are as follows: (1) the melatonin rhythm in breast milk is maintained independent of mode of delivery; (2) there is more daytime melatonin content in the colostrum of mothers who have delivered by cesarean section; (3) melatonin content decreases throughout the lactation time, mainly between colostrum and transitional milk, and the decrease is significant following elective cesarean section; and (4) at 1 month of life, no differences were found in melatonin content between vaginal delivery and elective cesarean section.
Our results show that human milk exhibits a daily rhythm of melatonin concentration similar to other body fluids 15 ; melatonin is more elevated at night than during the day, independent of mode of delivery, under physiological maternal and neonatal conditions. This condition was maintained at the three stages of lactation studied (colostrum, transitional milk, and mature milk).
These findings support the results from previous studies, 16 which investigated the melatonin content in human milk for the first time. Circadian rhythmicity on the third day and 1 month after birth was showed, similar to that observed in plasma of mother. Recently, other authors 17 found more melatonin in nighttime human milk than in daytime samples, with melatonin levels significantly higher in the colostrum of mothers of preterm babies. The daytime values of melatonin were lower than the values from this study. We collected samples in dim light of less than 30 lux and carefully protected the samples from light by covering the collection containers with opaque paper; this methodology could have influenced the results because if samples were collected under natural lighting, the observed values can decrease.18,19
We found a melatonin circadian rhythm in breast milk irrespective of the mode of delivery (vaginal or elective cesarean section). Only mothers with normal gestation were recruited. Specifically, possible infant or mother confounding factors, such as prematurity, asphyxia, gestational diabetes, hypertension, preeclampsia state, or any diseases experienced by the mother, were ruled out. Therefore, melatonin values were obtained under strictly controlled physiological conditions, except elective cesarean. Some stressful conditions not ruled out in other studies may modify the results. 20 Indeed, the characteristics of the population studied in this research are more homogeneous, and fewer adverse inflammatory or oxidative effects were expected.
These circadian variations in the composition of human milk would have nonnegligible functional importance. It is supposed that daily fluctuation in the level of melatonin might communicate time of day information to newborns, promoting the establishment of biological rhythms. This fact highlights the importance of breastfeeding for infant neurodevelopment and reveals that human milk is a powerful source of chrononutrition information to the newborn. Chronobiological variations in human milk may represent an additional mechanism that improves breastfed newborn adaptation to environmental conditions. 21 This advantage is not present in the case of infant formulas.
When searching for differences depending on mode of delivery, we found more melatonin content in the colostrum collected during the first 24 hours after elective cesarean section. This increase was observed in both the nighttime or daytime samples when compared with colostrum from mothers after vaginal delivery, but the differences were only significant for the daytime samples. This finding differs from those from a study conducted initially, 14 which compared the breast milk melatonin levels of women who had a vaginal delivery versus women who underwent cesarean section on the third day of life of the baby. In this study, there was a nocturnal surge in breast milk melatonin levels following vaginal delivery, but not following cesarean section.
On the other hand, no significant difference between diurnal and nocturnal secretion of melatonin was detected in the colostrum of cesarean mothers on the third day of life. The authors suggested that increased levels of tumor necrosis factor alpha following cesarean section could block melatonin production at the pineal level. The discordant results observed in our research may be due to differences in surgical procedures. It should be noted that the indications for and conditions of cesarean section are currently very different. In our investigation, all the procedures were performed under epidural analgesia. Emergency cesarean section or mothers who underwent general anesthesia were excluded. Due to improvement in anesthesia procedures, elective cesarean section is less stressful and could be further associated with less intense inflammation.22,23
In this study, carried out exclusively in term newborns, despite the higher diurnal melatonin content found in colostrum from mothers after cesarean section, the circadian rhythm remained, and higher nocturnal levels were found in this group. This is consistent with previous studies that found higher levels of melatonin in nighttime colostrum after elective cesarean section with respect to emergency cesarean section. 24 However, contrary to our results, in this study, breast milk melatonin levels after vaginal delivery were higher than those after caesarian section. This finding might be secondary to the study design, where preterm deliveries and asphyctic newborns were included.
Both vaginal delivery and cesarean section are a kind of stress to women and newborns, which could lead to oxidative stress and an inflammatory response. Melatonin is a potential neuroprotective agent against oxidative damage. 25 The increase in melatonin in the daytime colostrum from mothers after cesarean section may be interpreted as a protective mechanism to the newborn against oxidative and inflammatory stress consequences of a surgical procedure. In this sense, melatonin in colostrum is important not only for synchronization of the infant's circadian rhythm but also for the protective effects of breast milk. 26
In addition, we found a decrease in breast milk melatonin levels as lactation progressed. Our findings confirm those from Ref. 17 with the highest melatonin level in the colostrum, followed by transitional and mature breast milk. Moreover, we found a significantly greater decrease only after cesarean section in melatonin content in transitional milk with respect to colostrum once inflammation has presumably improved. Although higher melatonin content was found in all milk samples after cesarean section compared to vaginal delivery, no differences were found between the two groups on day 30 of lactation.
Limitations
Our study has some important strengths: the homogeneity of the participants, the strict inclusion and exclusion criteria that allow the description of melatonin content in human milk under nonpathological situations, and the rigorous methodology. The sample studied included only normal gestations that would likely increase the statistical validity. Human milk extraction, collection, and storage were carried out under dark conditions. However, as a result of the strict criteria, this study has a limited sample size.
Conclusions
The day/night rhythmicity remains in the three stages of lactation following both vaginal and elective cesarean delivery. A higher content of melatonin in diurnal colostrum could suggest more oxidative and inflammatory stress after elective cesarean section, and this higher melatonin content may play a protective role for the newborn. As lactation progressed during the first month after birth, the melatonin content gradually decreased in both the vaginal and elective cesarean delivery groups. Melatonin content in human milk after vaginal delivery remained more stable than after cesarean section. Our study may help to improve the administration of expressed human milk according to the time of day and the mode of delivery, and its potential therapeutic use under conditions of oxidative stress.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding was provided by the Foundation for the Promotion of Health and Biomedical Research in the Valencian Region (FISABIO), Valencia, Spain. Grant number 001/0017.