
Abstract
Background:
Limited data are available on the perinatal and postnatal transmission of novel coronavirus disease 2019 (COVID-19). The Centers for Disease Control and Prevention (CDC) and World Health Organization (WHO) recommended breastfeeding with necessary precautions to mothers with COVID-19.
Case Presentation:
A 20-year-old pregnant woman with no symptoms of COVID-19 presented to the hospital for delivery at 39 weeks of gestation. She was tested for severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) by reverse transcriptase polymerase chain reaction (RT-PCR) because her father had been diagnosed with COVID-19. A nasopharyngeal swab RT-PCR test was positive for SARS-CoV-2. Therefore, the baby and the mother were cared for separately after delivery. Breast milk obtained after first lactation was tested by real-time RT-PCR and was positive for SARS-CoV-2.
Conclusions:
In this article, we aimed to report the presence of SARS-CoV-2 in breast milk. Although further studies are needed, this situation may have an impact on breastfeeding recommendations.
Introduction
Although there are limited published data regarding the vertical transmission of severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), the possibility of perinatal transmission has been reported.1,2 There are currently two reports of SARS-CoV-2 in human breast milk detected by polymerase chain reaction (PCR).1,3 Lackey et al. evaluated studies that had tested 46 breast milk samples of 30 women for SARS-CoV-2 and all but 1 resulted negative for the virus. 2 However, the important question of whether SARS-CoV-2 can be transmitted from mother to baby through breastfeeding remains unsettled.
Currently, the World Health Organization (WHO) encourages mothers diagnosed with coronavirus disease 2019 (COVID-19) to breastfeed while practicing precautions such as hand and respiratory hygiene. In light of current scientific information, breast milk is not believed to play a significant role in the transmission of SARS-CoV-2, like other respiratory viral infections. 4 In addition, a recent preprint suggests that infants born to mothers with COVID-19 may benefit from secretory-IgA antibodies against SARS-CoV-2 in the breast milk. 5 In contrast, the U.S. Centers for Disease Control and Prevention (CDC) recommends that mothers with confirmed COVID-19 temporarily separate themselves from the neonate and express breast milk with a dedicated breast pump after practicing hand hygiene and wearing a face mask. 6
In this article, we report a pregnant woman with subclinical COVID-19 whose breast milk sample obtained after delivery tested positive for SARS-CoV-2 by reverse transcriptase PCR (RT-PCR). In addition, although an initial nasopharyngeal swab (NPS) sample from the neonate resulted negative, neonatal NPS, stool, and blood samples obtained after breastfeeding were all positive in real-time RT-PCR assay.
Case Presentation
A 20-year-old gravida 2 para 2 pregnant woman with no COVID-19 symptoms presented for delivery to another hospital at 39 weeks of gestation. She was tested for SARS-CoV-2 by RT-PCR because her father was diagnosed with COVID-19 a week earlier. She wore a surgical mask during normal vaginal delivery of a baby boy weighing 2,980 g (normal for gestational age). Meanwhile, her NPS SARS-CoV-2 RT-PCR test result was positive, so mother and baby were separated immediately after delivery. Thus, the mother had no contact with the baby after birth. Both were transferred to our hospital within 8 hours of delivery with the maternal diagnosis of subclinical COVID-19, on April 5, 2020.
The infant was admitted to the neonatal intensive care unit, while the mother was admitted to the infectious diseases and clinical microbiology ward. SARS-CoV-2 PCR test of an NPS obtained from the infant on admission (8–10 hours after birth) was reported as negative. The mother and infant were cared for in different clinical units to avoid contact with each other until discharge. In addition, the baby was not brought into contact with any other family members until discharge. Both mother and baby were healthy without fever or any other symptoms during their hospital follow-up. Their vital signs were stable and oxygen saturation levels were 98–99%. Their demographic and clinical characteristics and laboratory findings are summarized in Table 1.
Demographic and Clinical Characteristics and Laboratory Findings
Cycle threshold values.
BW, birth weight; CT, computed tomography; eGFR, estimated glomerular filtration rate; ND, not determined; NPS, nasopharyngeal swab; RT-PCR, reverse transcriptase polymerase chain reaction.
In line with current CDC recommendations, expressed fresh breast milk (without pasteurization or freezing) was given to the infant by health care professionals under strict precautions (hand hygiene, face mask, etc.) within the first 24 hours of admission, on April 6, 2020. 6 Meanwhile, after the first lactation, a breast milk sample was sent to the virology department of Ankara University for SARS-CoV-2 real-time RT-PCR testing. A positive result was returned, upon which feeding with expressed breast milk was discontinued. Breast milk samples were then tested for SARS-CoV-2 for the next 2 consecutive days to determine the viral shedding time.
The infant received a total of ∼240 cc of expressed breast milk in the first 36 hours of life. Because the infant was fed with breast milk for 24–36 hours until the mother's PCR test results were received, neonatal blood, stool, and NPS samples were obtained at 96 hours of age for SARS-CoV-2 real-time RT-PCR testing.
The timeline of asymptomatic SARS-CoV-2 infection of the mother and baby is summarized in Figure 1.
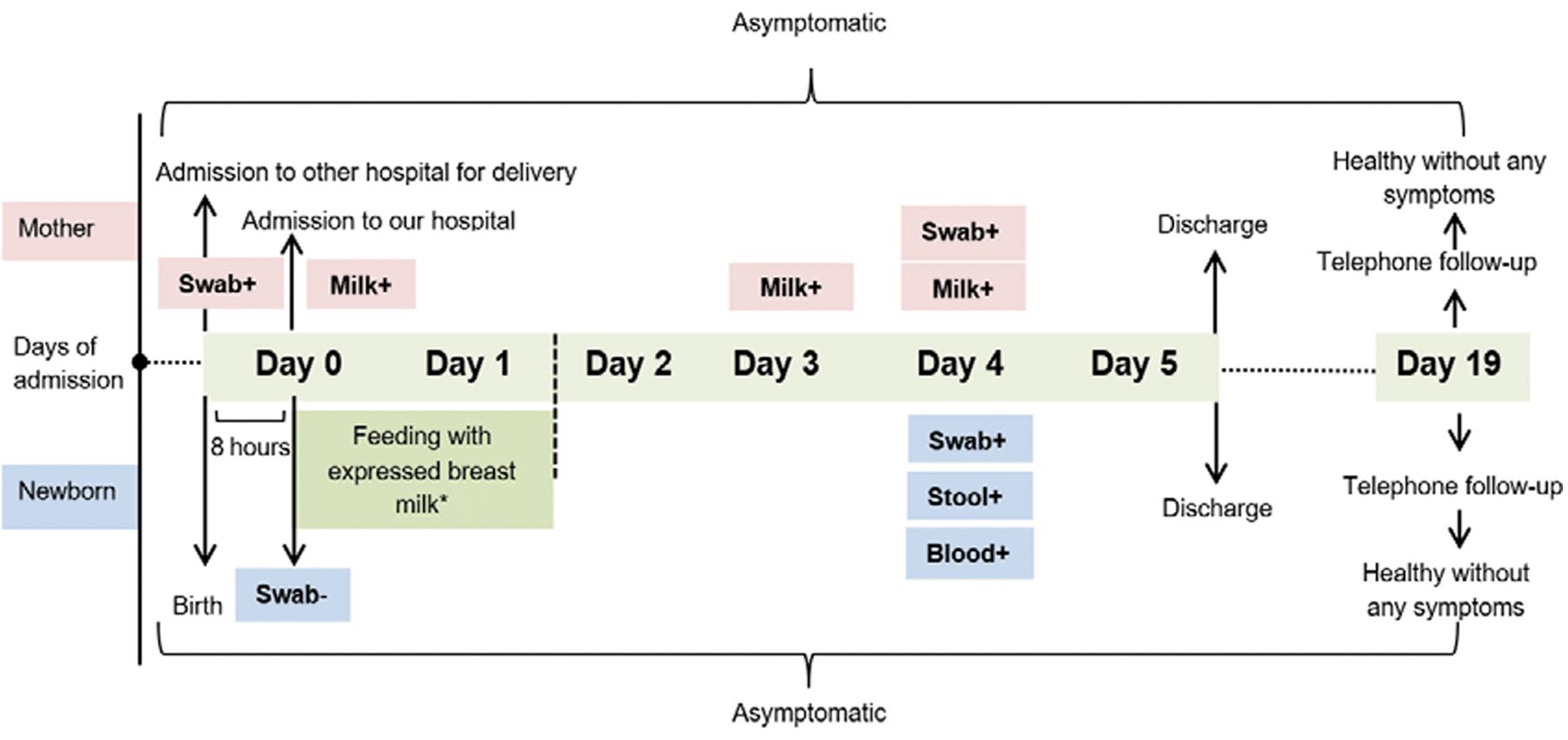
Timeline of asymptomatic SARS-CoV-2 infection of mother and newborn. Day 0, refers to admission time to Ankara City Hospital (April 5, 2020) and the first 8 hours of age of the newborn. Handling time of the samples was given in timeline (day 0, 8 hours of age; day 3, 72 hours of age; and day 4, 96 hours of age). Colostrum sample at 8–10 hours after birth and milk samples at ∼72 and 96 hours were positive for SARS-CoV-2 by PCR test. *Expressed fresh breast milk was given to the neonate till the test result of colostrum was handled on day 1. The timing of the different testing relative to birth; 8–10 hours after birth, the infant had a negative NPS PCR and at 96 hours had a positive NPS, stool and blood for SARS-CoV-2 by PCR. NPS, nasopharyngeal swab; PCR, polymerase chain reaction; SARS-CoV-2; severe acute respiratory syndrome coronavirus-2.
One-step RT-PCR test targeting the S coding gene performed using the QuantiNova Pathogen Kit (cat. no: 208654; Qiagen) showed almost equal viral load values in breast milk samples taken on April 5, 8, and 9 (cycle threshold [Ct]: 29.20, 28.85, 32.28, respectively). Ct values of the infant's NPS, blood, and stool samples taken on April 9 were detected as 32.71, 33.10, 32.84, respectively (Table 1).
During follow-up, neither the mother nor infant exhibited any symptoms that required any intervention or treatment. Five days after admission, the mother was encouraged to breastfeed while taking the necessary precautions, and both were discharged from the hospital. On follow-up conducted by phone 2 weeks after discharge (on postnatal day 19), both mother and baby were reported to be healthy with no COVID-19 symptoms. The reassuring outcome in this infant may have been secondary to the protective effect of breastfeeding.
Discussion
Emerging infections have a critical impact on pregnant women and their babies. As the current COVID-19 pandemic spread to Turkey, it brought important implications to public health. Besides the other clinical and public health issues, it has raised serious concern regarding the impact of the disease on pregnant women and fetuses/neonates.
There are insufficient data on the perinatal and postnatal transmission of COVID-19. One study reported that none of 30 neonates born to mothers with COVID-19 infection was positive for SARS-CoV-2 RT-PCR test. 7 In another study, breast milk samples from 6 of 9 postpartum women with SARS-CoV-2 infection all tested negative for SARS-CoV-2 nucleic acid. 8 This result may be due to a low viral load in breast milk, the testing method used (test validation, etc.), or the timing of sample collection. In addition, the transport and storage of milk is important for the results.
As already mentioned, a literature review by Lackey et al. showed that only 1 of 46 breast milk samples obtained from 30 women was positive for SARS-CoV-2. 2 Although there have been only two reports of PCR viral detection in breast milk to date, the role of breastfeeding in vertical transmission is still uncertain.1,3
In the present case, SARS-CoV-2 PCR testing of breast milk was performed immediately after birth and on the following days. In addition, neonatal blood, stool, and NPS samples collected after breastfeeding were all positive for SARS-CoV-2 in real-time RT-PCR test. Unfortunately, we did not have the opportunity to test cord blood and placenta, since the delivery took place in another hospital. Although the first neonatal NPS sample obtained at ∼8–10 hours of age tested negative, it is difficult to say that the baby did not have SARS-CoV-2 perinatal infection. The American Academy of Pediatrics (AAP) recommends that testing of newborns not be done until ∼24 hours of age. 9 In addition, some infants may have a negative test even at 24 hours.
Therefore, transmission in the present case may be due to horizontal transmission through breast milk or congenital/perinatal infection at delivery with a false-negative NPS test on postnatal day 1. However, there remain other possibilities. The infant could have been infected from contact with blood or secretions during vaginal delivery. In addition, the possibility of infection from contact with family or staff cannot be ruled out, as the infant was cared for by multiple personnel at the two hospitals and during transport.
Conclusion
In this report, we present a case of subclinical SARS-CoV-2 infection in a mother and her infant. SARS-CoV-2 was detected in colostrum and breast milk by SARS-CoV-2 RT-PCR testing at ∼8 hours, 72 hours, and 96 hours after delivery. It remains unclear whether the infant's first NPS SARS-CoV-2 RT-PCR test result was a false negative, consistent with congenital or peripartum infection, or whether the infant was subsequently infected through breast milk. Although the benefits of breastfeeding may outweigh the risks, this decision should be made together by the parent and the doctor. The present report contributes important data demonstrating the presence of SARS-CoV-2 nucleic acid in breast milk. We believe these findings may have important public implications for both mothers and newborns.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.