
Abstract
Objective:
To assess whether in-hospital infant formula supplementation impacts later successful breastfeeding among healthy mother–infant dyads in the United States who are not intending to exclusively use infant formula.
Study Design:
Using secondary analysis of a national longitudinal survey (Infant Feeding Practices Study II, n = 2,399), we estimated effects of in-hospital infant formula supplementation on later breastfeeding success by matching mothers whose infants received in-hospital formula supplementation with mothers whose infants did not. Estimates were compared across four matching methods. Outcomes of breastfeeding success included likelihood of following a sustained breastfeeding trajectory for the first year postpartum; feelings of favorability and breastfeeding as long as desired postweaning; and breastfeeding intention, initiation, and duration for subsequent children.
Results:
In-hospital formula supplementation halved the likelihood of following a breastfeeding trajectory characterized by sustained exclusive breastfeeding. Supplementation decreased feelings of favorability toward breastfeeding postweaning but did not impact the likelihood of feeling that one breastfed as long as desired. Supplementation did not impact intention to breastfeed a future child; it did, however, decrease the likelihood of breastfeeding initiation with a subsequent child by >66% and reduced average duration of breastfeeding any subsequent children by >6 weeks.
Conclusion:
A lack of experimental methodologies in previous studies makes it difficult to determine a causal link between infant formula in the hospital and less breastfeeding success. Assuming we have accounted for all appropriate confounders, this study provides evidence for such a causal link. Birth hospital policies and practices should speak of this risk of harm.
Introduction
Early experiences within the birth hospital have the potential to impact later breastfeeding success.1,2 One common early experience is supplementation with infant formula. An abundance of evidence suggests health disadvantages of not breastfeeding; the American Academy of Pediatrics (AAP) recommends that hospitals provide maximal support for exclusive breastfeeding. 3 However, the routine use of in-hospital formula supplementation is a widespread practice, with approximately one quarter of U.S. hospitals supplementing at least 50% of healthy breastfed newborns with formula. 4 Several studies have found that supplementation is associated with shorter overall breastfeeding duration.5–7
Most studies to date have utilized nonexperimental correlational methodologies to examine associations between in-hospital formula supplementation and breastfeeding outcomes. Without experimental/quasi-experimental studies, it remains difficult to determine whether in-hospital supplementation causes or is merely associated with reduced breastfeeding. Nickel et al. 8 used propensity score weighting, estimating that in-hospital formula supplementation decreased the duration of any breastfeeding in the United States by ∼10.5 weeks. A large-scale study in Hong Kong leveraged a natural experiment, finding that a change in hospital policy to paying fair market value for formula led to fewer dyads being supplemented with formula (from 82.3% to 58.7%) and overall longer breastfeeding durations postdischarge (from 8 to 12.5 weeks duration), suggesting a causal link between less accessible in-hospital supplementation and more sustained breastfeeding. 9
In a third study using quasi-experimental design, researchers tested the impact of assigning one wing of a maternity hospital in Canada to restricted infant formula use. 10 The authors found that even though rates of supplementation in the restricted wing decreased from 91% to 37%, the likelihood of predominant breastfeeding at 4 and 9 weeks postpartum for individual mothers did not differ between groups. Although effects sizes from this study differ from more recent studies on the influence of formula supplementation, unanticipated null findings from strong quasi-experimental designs do signal a need for continuing causal inference investigation.10,11
In a recent randomized control trial, early limited formula supplementation for infants with excessive weight loss (10 mL after each breastfeed, discontinued after copious milk production begins) was found to reduce the likelihood of breastfeeding at 12 months by ∼35%. 12 Estimating the impact of supplementation patterns on long-term breastfeeding success in a diverse national sample continues to be imperative for health professionals to effectively inform birth hospital guidelines.11,13,14
One approach to causal inference without randomization is to use observational data to construct two comparable groups—those who received formula in the hospital and those who did not—that can be reasonably compared with assess impact of supplementation.14,15 Propensity score matching (PSM) is the most common matching technique within nonexperimental causal inference paradigms. 16 Other matching techniques have been developed that can achieve closer balance between treatment and control groups than nearest-neighbor PSM; these include genetic matching, optimal matching, and full matching.17,18 No U.S. studies have been conducted to date that use these causal inference matching methods to assess the impact of in-hospital formula supplementation on later breastfeeding success.
The definition of breastfeeding “success” is another important consideration. Many different metrics may be meaningful or useful. Population-measurable metrics are most consistently used in medicine; these include initiation of breastfeeding (did a single breastfeeding attempt occur), overall duration of breastfeeding (how long did a mother provide any breast milk), and exclusivity of breastfeeding (was the infant supplemented with infant formula). A more nuanced metric of success is a sustained breastfeeding trajectory, which approximates a biologically normal nursing relationship (i.e., a pattern of extended exclusive breastfeeding with a slow tapered weaning period).19,20 This is important because the protective effect of breastfeeding has been found to be a function of both breastfeeding exclusivity and duration. This definition of a trajectory also maps more closely onto current AAP recommendations. 3
Mothers' own perceptions of success are also relevant. 21 These include breastfeeding as long as one desires and satisfaction with breastfeeding.7,22,23 Finally, breastfeeding intention and follow through on breastfeeding for subsequent children can aid understanding of the long-term health implications of formula supplementation for mothers and their families. 24
To address these gaps, this study estimates the causal impact of in-hospital formula supplementation on short- and long-term indicators of breastfeeding success, using matching within an observational data set. We hypothesize that each measure of breastfeeding success will be negatively impacted by in-hospital formula supplementation.
Materials and Methods
Data and participants
The Infant Feeding Practices Study II (IFPS-II; administered by the U.S. Centers for Disease Control and Prevention and the Food and Drug Administration) was conducted between 2005 and 2012 on a national sample of pregnant women. 25 Participants were recruited through a national consumer opinion panel of 500,000 households. Inclusion criteria for participants at recruitment included age at least 18 years and pregnant. Exclusion criteria for continuing involvement included infant born <35 weeks, infant or mother diagnosed with condition(s) that would affect feeding, extended neonatal intensive care unit (NICU) admission, and infant weighing <5 pounds.
During the Year 1 study (2005–2007), surveys were mailed to the mother's home ∼30 weeks' gestation (the prenatal wave), ∼3 weeks postpartum (the neonatal wave), and then approximately monthly for the child's first year. The follow-up Year 6 survey (2012) was sent when the index child was ∼6 years old (mean = 6.4 years, standard deviation [SD] = 0.19 years). Out of 4,902 mothers initially sampled, 3,033 mothers returned at least the prenatal and neonatal surveys for the Year 1 study (see Table 1 for demographic characteristics). The Year 6 follow-up survey has a sample size of 1,542 mothers, 708 of whom had had at least one subsequent child. All materials and procedures were approved by the FDA's Research Involving Human Subjects Committee (the institutional review board).
Infant Feeding Practices Study II
Demographic characteristics, n = 3,033.
Breastfeeding friendliness is based on Maternal Practices in Infant Nutrition and Care score, CDC Breastfeeding Report Card (2014).
Measures
Treatment: in-hospital supplementation
The treatment variable is a measure of whether the infant received any formula during the birth hospital stay, collected on the neonatal survey.
Outcome: breastfeeding trajectory
Breastfeeding trajectory was constructed using group-based trajectory modeling (GBTM), which utilizes weekly percentage of breast milk versus formula provided to the infant from the neonatal wave through month 12. 26 GBTM is a longitudinal person-centered technique to explore patterns of behavior over time, and to cluster individuals into latent subgroups that share a common behavioral trajectory. 27 Each individual is given a posterior probability of assignment to each subgroup and is then assigned membership to the subgroup for which they have the highest probability. In other words, each individual is assigned to the cluster that most closely matches their individual trajectory.
We reconstructed the GBTM from Whipps et al., 26 which describes four latent groups of mothers in the IFPS-II Year 1 sample of 3,033 mothers: (1) Formula Feeding; (2) Combination Feeding, Early Weaning; (3) Combination Feeding, Later Weaning; and (4) Sustained Breastfeeding (Fig. 1, reproduced with permission). For this study, the outcome variable is the likelihood of membership in the Sustained Breastfeeding trajectory relative to the three other groups combined. This trajectory is closest to the recommendations given by the AAP for both exclusivity and duration of breastfeeding and the closest to a biologically normal breastfeeding trajectory.3,19
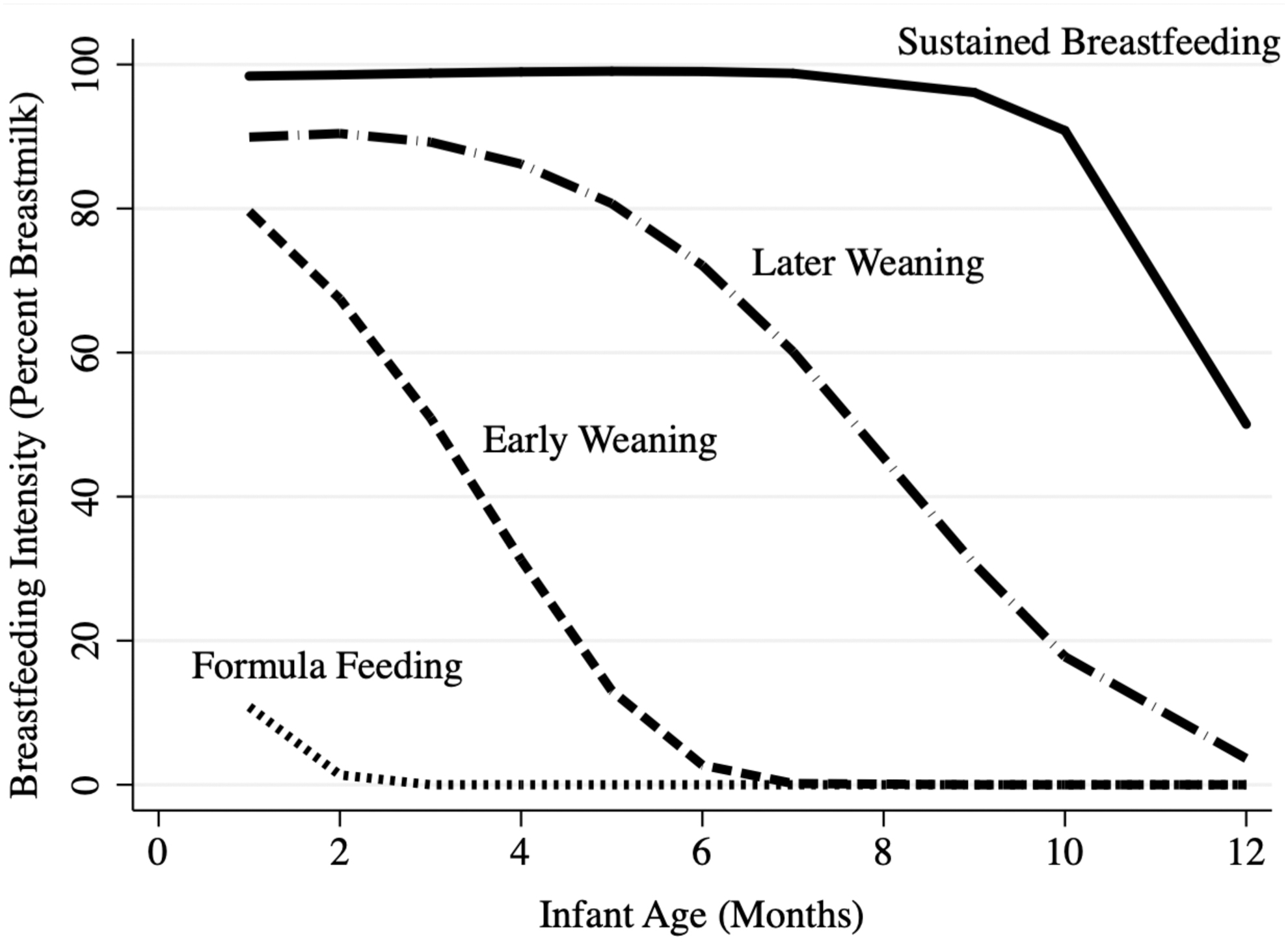
Breastfeeding trajectories in the first year postpartum. Four trajectories of infant breast milk consumption over the first postpartum year. Figure reproduced with permission from Whipps et al. 26
Outcome: maternal favorability toward having breastfed
In the monthly survey on which the participant reported ceasing breastfeeding, participants reported how they felt about their breastfeeding experience on a 1–5 Likert scale from Very Unfavorably to Very Favorably. This scale was treated as continuous.
Outcome: breastfeeding as long as desired
On this same survey wave, participants reported Yes/No to the question “Did you breastfeed as long as you wanted to?”
Outcome: intention to breastfeed a future child
On this same survey wave, future breastfeeding intention was measured on a 1–5 Likert scale from Very Unlikely to Very Likely to breastfeed a future child.
Outcome: initiation and duration of breastfeeding for subsequent children
In the Year 6 survey, mothers who had had subsequent children (708 mothers, 935 total children) were asked to specify how long they breastfed each subsequent child. Initiation for the next subsequent child was dichotomized (Any Breastfeeding versus No Breastfeeding). Duration of subsequent breastfeeding was operationalized as the average breastfeeding duration in weeks over all subsequent children reported by the participant at Year 6, not including currently breastfeeding mother–infant dyads.
Covariates
The 27 potentially confounding pretreatment covariates used in matching analyses (demographics, maternal health and reproductive history, birth outcomes, and psychosocial resources) are defined in Supplementary Appendix SA1. These are similar to covariates used in other studies.6,8
Data analysis
Matching
We estimate the impact of any formula supplementation during the birth hospital stay on breastfeeding outcomes for mothers who supplemented—the average treatment effect on the treated. For greater robustness of results, four matching methods were used: nearest-neighbor PSM, 16 genetic matching, 17 optimal matching, 18 and full matching. 18 Each approach uses a different matching algorithm to restructure the data to create matched treatment and control groups; thus, each resulted in a different analytic sample.16–18
Missing data
For Year 1, 3,033 mothers were assigned to a breastfeeding trajectory in the previous study. 26 GBTM uses an expectation-maximization algorithm 28 to account for missing data and attrition. Of those 3,033 mothers, 585 (19%) were missing the treatment variable or did not know whether the child was given formula and were thus excluded from analysis. Those who prenatally intended to exclusively formula feed (49 mothers, 2%) were also dropped from analysis, as this variable is nearly perfectly colinear with in-hospital formula use. Missingness on other variables was <10%. Matching covariates were singly imputed within treatment condition using a chained-equation procedure (multiple imputation by chained equations [MICE]) before matching.29,30 Our analytic sample is 2,399 mothers; 1,005 (42%) supplemented with formula in the hospital.
Matching treated with control individuals
Using the four matching techniques already described, all 1,005 treated individuals were matched with control individuals using the MatchIt package in R. 31 All matching methods used identical matching covariates. Nearest-neighbor PSM and full matching were conducted without replacement, optimal and genetic matching utilized replacement. Adequate balance was defined a priori as <0.10 standard deviations between treated and control groups. 32 Individuals were weighted in the impact analyses to reflect whether or not they were matched, and in the case of optimal and genetic matching, how many times they were matched. Propensity scores were estimated using a binomial model regressing infant formula supplementation on all matching variables, that is, the probability of using infant formula given the covariates.
Analyses assume ignorability—which we have accounted for all possible confounding covariates in our model—and sufficient overlap such that appropriate counterfactuals in the control condition can be found for all treated individuals. 33 Analyses also assume that in-hospital supplementation for one participant was not impacted by another participant, and that there is only one version of the treatment (i.e., stable unit treatment value assumption, or SUTVA 33 ). Given the sampling design, 25 we can be reasonably certain of the first SUTVA. The second SUTVA is less plausible; it is likely that some infants were supplemented with only a few milliliters of formula, while others received many fluid ounces over several days. Our analyses cannot assess heterogeneity of impact across this spectrum of treatment.
Impact analyses
The impact of in-hospital formula supplementation on those who received formula was estimated using weighted multivariate logistic regression for dichotomous outcomes and weighted multivariate ordinary least squares regression for continuous outcomes. The weights in these analyses reflect the number of times each participant's information was used in postmatching restructured data sets. All impact analyses were adjusted for multiple comparisons within matching method using Simes' procedure to derive a q-value (i.e., adjusted p-value) that accounts for the false discovery rate over multiple comparisons.34–36
Results
Overlap and balance
Before matching, we compared mothers who supplemented with infant formula with those not supplementing on all outcomes of interest. Prematching group differences were tested using either analysis of variance (ANOVA) (for continuous outcomes of interest) or Pearson's χ 2 (for dichotomous outcomes; Table 2). We found that mothers who supplemented with infant formula were less likely to follow a trajectory characterized by sustained exclusive breastfeeding, less likely to have breastfed as long as they wanted, and less likely to initiate breastfeeding with the next child. Mothers who supplemented also felt less favorably about having breastfed, had weaker intentions to breastfeed in the future, and breastfed their subsequent children for fewer weeks. We found sufficient area of common support to suggest that matching is appropriate (Supplementary Appendix SA2). 37
Descriptive Results for Unmatched Analytic Sample
Significance tested using one-way ANOVA and Pearson χ 2 .
ANOVA, analysis of variance.
Before matching, 37% of the 27 matching covariates were within ±0.10 SDs' difference between the control and treated samples. Across all methods, matching substantially improved this covariate balance. Balance meeting our 0.10 SD criteria on all 27 covariates was achieved with genetic matching. Optimal matching resulted in two out-of-range covariates, whereas full matching resulted in one out-of-range covariate. Nearest-neighbor PSM performed the worst, with seven out-of-range covariates. The pruning necessitated by various matching methods (e.g., dropping unmatched control cases) also resulted in differential sample sizes (Table 3).
Balance on Matching Pretreatment Covariates Between Treated and Control Samples by Matching Strategy
Insufficient balance (standardized mean treatment control difference >|0.10|) denoted with
API, Asian-American & Pacific Islander; BF, breastfeeding; Std., standard.
Impact analyses
Results in this section are presented as estimates of causal effects under the assumptions of no hidden bias, no interference between units, and sufficient overlap across treatment and control groups. 33 All estimated effects correspond to the group of treated individuals and are relative to the counterfactual of no in-hospital formula supplementation. Inferences are made only for those mothers who did not report prenatal intent to exclusively formula feed. Across matching methods, results consistently show a statistically significant negative impact on several indicators of future breastfeeding success from in-hospital infant formula supplementation (Table 4).
Impact of Early Infant Formula Supplementation by Matching Strategy
p-value adjusted to q-value to control for multiple comparisons using Simes' method; +q < 0.10, *q < 0.05, **q < 0.01, ***q < 0.001.
AOR, adjusted odds ratio; Coeff., coefficient; PSM, propensity score matching; SE, standard error.
Breastfeeding trajectory
In-hospital supplementation reduced the likelihood of membership in the sustained breastfeeding trajectory by at least 50% (adjusted odds ratio [AOR] across matching method ranging from 0.35 to 0.47, q < 0.001).
Maternal favorability toward having breastfed
In-hospital supplementation with formula slightly reduced postweaning feelings of favorability toward the breastfeeding relationship. This finding was consistent across all matching methods, with coefficients ranging from −0.248 (q < 0.01) to −0.307 (q < 0.001).
Breastfeeding as long as desired
Supplementation did not significantly change whether mothers report breastfeeding as long as desired. Although a significant reduction in this measure was seen with PSM (AOR = 0.761, q < 0.05), there was no significant effect when treatment-control participants were matched using the other methods and adjusting for multiple comparisons.
Intention to breastfeed a future child
There was no significant impact of formula supplementation on the strength of the intention to breastfeed a future child after adjusting for multiple comparisons.
Initiation and duration of breastfeeding for subsequent children
In-hospital formula supplementation reduced the likelihood of initiating breastfeeding with the next subsequent child by at least 66% (AOR range from 0.196 to 0.331). Findings were consistent across all matching methods in magnitude and direction, although the effect was slightly weaker and only reached marginal significance using the genetic matching method (AOR = 0.257, q < 0.10). We found a similar pattern for average duration of any breastfeeding for all subsequent children: using PSM and full matching, supplementation reduced average breastfeeding duration by >6 weeks, compared with the average breastfeeding duration had that mother not supplemented with formula in the hospital (coefficients of −6.241 and −6.7 respectively, q < 0.05). The effect sizes were similar for optimal matching and genetic matching, although the effects did not reach significance.
Discussion
Across four PSM methods, and conditional on the assumption that we have accounted for all confounding covariates, we find consistent results in terms of magnitude and direction of the effect of in-hospital infant formula supplementation on short- and long-term measures of breastfeeding success. As hypothesized, supplementation reduced the likelihood of following a breastfeeding trajectory characterized by sustained exclusive breastfeeding; it also reduced feelings of favorability toward having breastfed. Supplementation reduced both the likelihood of initiating breastfeeding for the subsequent child and overall average duration of breastfeeding for all subsequent children. These findings suggest that in-hospital supplementation may be a cause of later breastfeeding difficulty, not just a marker.2,10 Our results align with previous observational research,5–8 recent randomized trials, 12 and relevant theory. 38
We intentionally expanded the notion of breastfeeding “success” in this study, going beyond the traditional biomedical definitions of total duration and/or breastfeeding exclusivity to 6 months for a single mother–infant dyad.3,39 These success metrics included person-centered longitudinal behavioral measures, postweaning perceptions of breastfeeding, and breastfeeding behaviors for subsequent children born later in the reproductive life course of the mother. Given the dominance of a relatively small number of biomedical definitions of breastfeeding success39,40 and the paucity of research on breastfeeding outcomes beyond a single mother–child dyad, 41 broadening the definitions of success in this way represents an important contribution to the literature.
There are several mechanisms by which in-hospital supplementation might impact breastfeeding success. Formula supplementation can displace early at-breastfeeds, limiting the nipple stimulation and breast emptying necessary for a full milk supply to develop. 42 Supplementation by bottle may be especially deleterious due to flow preference and subsequent breast refusal. 6 Another potential mechanism is proclivity to develop the perception of an inadequate milk supply. 43 This perception can lead to more negative feelings regarding breastfeeding in general, 44 and perhaps a lower likelihood of breastfeeding subsequent children. Future studies should examine whether substance (donor milk versus infant formula) and mode (bottle, cup, syringe, or finger feeding) of supplementation have differential impacts on these understudied metrics of breastfeeding success.
We did not find strong evidence that in-hospital supplementation impacted breastfeeding as long as desired. This is surprising, given that supplementation decreased actual breastfeeding. One hypothesis is that breastfeeding intentions and goals are dynamic throughout the breastfeeding relationship; they can change over time and in response to shifting circumstances.1,38,45 We also found equivocal evidence that in-hospital formula supplementation impacts intention to breastfeed a future child. Social desirability bias might be one explanation. In our sample, ∼90% reported a “5” or “4” on the response scale from 1—Very Unlikely to 5—Very Likely to breastfeed a hypothetical future child. Mothers may be motivated to report intent to breastfeed their next child, regardless of the strength of those intentions.
The null effects for these two outcomes of interest may also reflect treatment heterogeneity. However, lack of strong evidence for an effect does not necessarily mean that there is not a meaningful effect in reality; absence of evidence is not evidence of absence. 46 Future studies should further probe these sources of heterogeneity.
The finding that in-hospital formula supplementation can negatively impact later breastfeeding success has implications for clinical practice, including pediatrics, mental health support services, and obstetrics. Although there is a clear need for medically indicated supplementation (with infant formula or donor breast milk) under certain circumstances, routine supplementation of healthy breastfed infants should be avoided where possible. Birth hospitals in the United States should have policies in place that speak of this risk of harm.
Limitations
There are several limitations to this study. The IFPS-II is an older data set. As far as we are aware, no other national longitudinal data exist encapsulating the outcomes of interest. Although patterns of infant formula supplementation have changed in the 15 years since the IFPS-II began, there is evidence that many healthy breastfeed infants are still being supplemented without medical indication in the United States. 4 Therefore, this study, which leverages the rich longitudinal methodology and national sampling of the IFPS-II, is still an important contribution. However, future research initiatives should prioritize representative sampling on a more regular basis—perhaps every 5 years—to reduce the reliance on decade-old data and to more accurately capture trends over time in breastfeeding behaviors and the societal supports for those behaviors.
Another limitation is that the IFPS-II is a national data set, but not nationally representative. White mothers, married mothers, and higher -income mothers are overrepresented. 25 The relatively small number of participants from marginalized groups limits generalizability to these communities and precludes testing for heterogeneity across these groups. Future data collection efforts should oversample from these underrepresented groups to better characterize and ameliorate the structural and institutional barriers to breastfeeding facing mothers of color, single mothers, and mothers with lower income.47,48 Relatively larger samples of these currently underrepresented communities, and the data disaggregation that those larger samples allow, would also provide the basis for more accurate descriptions of the unique strengths and needs of each of these subpopulations.
Finally, PSM methods using observational data can adjust for imbalance across groups based on observed characteristics, but not unobserved characteristics. 16 There may be unmeasured factors that are the cause of both in-hospital supplementation and less breastfeeding success; for example, other characteristics of the hospital, 49 or unmeasured physiological factors that contribute to delayed or failed lactogenesis. 50 Future studies should continue addressing these issues of ignorability, 33 as well as issues of mediation and the temporal cascades between early breastfeeding problems and formula supplementation.
Conclusion
This study suggests that links between infant formula use in the hospital and negative breastfeeding outcomes both for the index child and future children may be causal in nature, not merely correlational. These findings are conditional on the assumption that we have accounted for all confounding covariates. There are several hypothesized mediating pathways through which supplementation may be impacting breastfeeding outcomes across the reproductive life course, encompassing physiological as well as psychological processes. Although there are significant limitations to the current data, including lack of representativeness of the sample and length of time since the first wave of data was collected, these findings still have clinical significance for health care providers working within obstetrical and pediatric settings in the United States and in other high-income countries.
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.