
Abstract
Introduction:
Evaluation of the safety of taking lamotrigine (LTG) during lactation in breastfed infants varies according to the information sources. As it is possible that prescribers may avoid prescribing LTG despite of it being one of the essential drugs, more information needs to be accumulated to facilitate its use.
Materials and Methods:
We retrospectively compared the safety of LTG during the lactation period in 20 pairs of mothers and infants with 20 pairs as the control group.
Results:
The mean dose of LTG in 20 mothers was 161.1 mg/day (range: 50–400 mg/day). None of the infants showed a neonatal withdrawal syndrome score of 2 or more up to 1 month after delivery. Although drowsiness (n = 3), skin rash (n = 11), jaundice (n = 8), heart murmur (n = 1), poor suckling (n = 1), and retractive breathing (n = 1) were observed in infants, none of these adverse events were serious and the infants recovered. Nineteen of 20 pairs could continue lactation until 1 month after delivery. One pair discontinued breastfeeding because of pain in the mother's nipples. All pairs could continue maternal medication. We then compared the results with those of the control group. There were no significant differences in the presence of adverse events between the LTG and control groups.
Conclusion:
These data suggest that taking low to moderate doses of LTG during the lactation period might be relatively safe, at least for a period of 1 month after delivery.
Introduction
Breastfeeding plays many important roles in the well-being of infants, which include providing nutrition, 1 reducing the risk of infection,2,3 facilitating the establishment of attachment between mothers and infants, 4 and reducing the risk of occurrence of breast cancer in mothers. 5 According to the results of a Japanese national nutrition survey on preschool children in 2015, 96.5% of infants were breastfed including mixed feeding at 1 month after delivery. 6
With the recent introduction of new generation anti-epileptic drugs (AEDs) in clinical setting, treatment strategies for patients with epilepsy have been developed. Lamotrigine (LTG) is one of the major AEDs and is used for the treatment of epilepsy and bipolar disorder. Patients with these diseases require long-term pharmacotherapy, even during the perinatal period. In the guidelines published by the Japanese Society of Neurology in 2018, 7 LTG was identified as one of the AEDs with a low incidence of infant malformation when used as a single agent in pregnant women. However, the information available so far is still insufficient for medical staff to recommend breastfeeding to maternal patients after delivery because there have been some discrepancies in the description of evaluation of safety for taking LTG during lactation among information sources. LTG was evaluated as “L2 (Probably Compatible)” in Medication and Mothers' Milk (MMM) 20198 and described as “Limited Human Data—Potential Toxity” in Drugs in Pregnancy and Lactation (DPL), 11th edition. 9 The website LactMed contains information about using drugs for breastfeeding mothers, where it is described that breastfed infants should be carefully monitored for side effects and if skin rash occurs in infants, mothers should discontinue breastfeeding until the cause can be established. 10 This discrepancy is a concern while prescribing LTG for women of childbearing age. It was reported that the frequency of prescribing AEDs, including LTG, for women from the preconception period to after conception has decreased and has not recovered to the previous levels even after delivery. 11
The oral bioavailability of LTG is ∼98% 12 and it can significantly penetrate breastmilk. 13 LTG is mainly metabolized via hepatic UGT1A4. 14 However, it is known that fetal glucuronidation enzymes are immature and develop postnatally. 15 The LTG blood levels in infants can increase because of the limited capacity to metabolize LTG. 16 Birnbaum et al. reported that there were large differences in the blood levels of LTG between infants. 17 Previous reports have indicated that LTG taken by mothers during lactation may cause mild elevation in platelet count 13 and severe apnea 16 in infants. Furthermore, LTG can cause life-threatening skin rash as an adverse event (AE)18,19 and a Blue Letter (one of the warning letters regarding medical safety) was issued in Japan on February 4, 2015. 20 This may be one of the reasons for avoiding the use of LTG in pregnant and breastfeeding mothers.
With the aim of accumulating clinical data through a comprehensive survey, we evaluated the safety of LTG therapy during lactation period on the well-being of the infants.
Materials and Methods
Plan-sheets for lactation
In 2011, we started the systematic evaluation of risk for infants whose mothers breastfed while taking psychotropic drugs in the Department of Obstetrics, Tohoku University Hospital. At first, pregnant women were asked to provide information about their disease symptoms, drugs used, dosage regimen, and their desire to breastfeed after delivery on the check sheets named as “plan-sheets for lactation” at ∼28 weeks of gestation. Based on the check sheets, midwives interviewed each pregnant woman about her background and noted her comments on mother's concerns and requirements regarding breastfeeding after delivery, and sent it to the Department of Pharmaceutical Sciences. Pharmacists collected the information about the safety of taking drugs, which are described on plan sheets for lactation during lactation period from sources such as MMM and DPL,8,9 and then provided those information with the pharmacists' comments to the obstetricians. The obstetricians discussed the risk of breastfeeding of infants by mothers taking drugs during the lactation period with pediatricians, and explained the results of evaluation of the pregnant women by the medical staff.
Data collection and statistical analysis
Pregnant women taking LTG were evaluated for the risk using plan sheets for lactation from January 2011 to November 2017. We excluded the following cases from our examination: women who delivered in other hospitals and infants who were exclusively formula-fed. The remaining participants were included in the LTG group. In addition, women not taking LTG and using the plan sheets from April 2017 to March 2018 were enrolled as the control group, with the exclusion criteria being the same as for the LTG group. They were matched with the LTG group according to gestational weeks at delivery, infants' sex, and body weight (BW) at birth (1:1 ratio).
We collected their characteristics based on medical records (MRs) and plan sheets for lactation. Maternal characteristics including age, body mass index (BMI), daily dose of LTG, purpose of taking LTG, number of psychotropic class of drugs taken (including LTG), and gestational weeks at delivery were collected. BMI was calculated using maternal height and BW that was measured for the first time after delivery. Infant characteristics including sex, BW at birth and 1-month checkup, weight gain from birth to 1-month checkup, nutritional methods (exclusive breastfeeding or mixed feeding), Isobe's neonatal withdrawal syndrome (NWS) score, 21 and number of AEs from just after birth to 1 month after delivery were collected from their MRs retrospectively. The NWS scoring system is a modified version of Finnegan's score, 22 which is one of the assessment tools for NWS and is used for the purpose of early treatment. The Isobe's scoring system is based on a point addition system that mainly evaluates the symptoms related to the digestive, autonomic, and central nervous systems. According to Isobe's scoring system, medical treatment is often considered to be needed when the NWS score is 8 or more. 22 Medical staff routinely evaluated the infant's symptoms at 2 hours, 1–6 days, 2 weeks, and 1 month after delivery according to the scoring system, and calculated the NWS score. We used the highest score among the infant's score as the NWS score. The data were compared using Student's t-test, Mann–Whitney U-test, chi-square test, and Fisher's exact test, as appropriate. Values of p < 0.05 were considered statistically significant.
This study protocol was reviewed and approved by the Ethics Committee of Tohoku University Graduate School of Medicine (2018-1-594).
Results
Characteristics of individual patients in the LTG group
We identified 22 pairs of mothers and infants for whom the plan sheets for lactation, including LTG were applied (Table 1). Two women were excluded (one woman delivered in another hospital, and the other woman was exclusively formula feeding). Finally, 20 women were included in the LTG group (Fig. 1) and their characteristics are given in Table 1. Two mothers received a relatively high dose of LTG (300 and 400 mg/day).
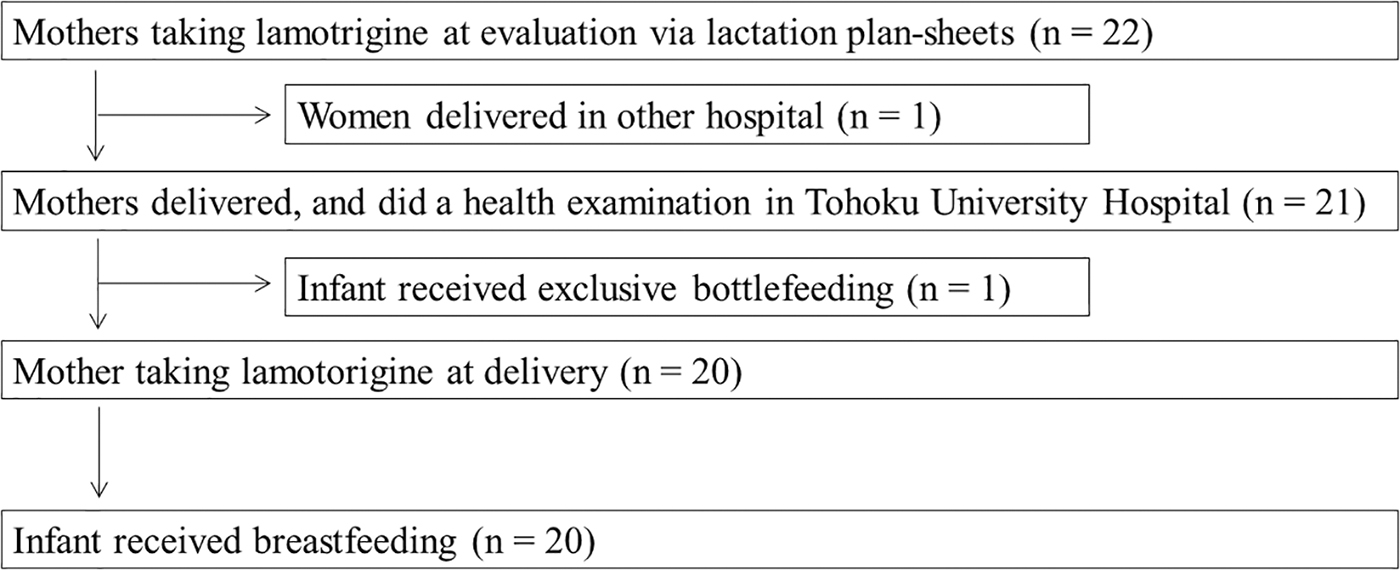
Flowcharts of the research subjects. We identified 22 pairs of mothers and infants for whom the plan sheets for lactation, including LTG were applied. Two women were excluded (one woman delivered in another hospital, and the other woman was exclusively formula feeding). Finally, 20 women were included in the LTG group. LTG, lamotrigine.
Maternal and Infant's Characteristics
BD, bipolar disorder; BMI, body mass index; BW, body weight; DRS, drowsiness; EPI, epilepsy; Ex, exclusive breastfeeding; F, female; JD: jaundice; LTG, lamotrigine; M, male; Mix, mixed feeding; NWS, neonatal withdrawal syndrome; PD, psychotropic drugs; Skin, skin rash; Wks, gestational weeks at delivery.
Characteristics of mothers and infants in the LTG and control groups
The mean maternal age at gestation was 31.2 years (range: 17–39 years) (Table 2). We could not collect information about weight at delivery for three women, but the mean BMI of the remaining 17 women was 22.9 kg/m2 (range: 18.6–27.8 kg/m2). The mean dose of LTG was 161.1 mg/day (range: 50–400 mg/day). None of the women changed the LTG dose from the time of plan sheets based evaluation to 1-month checkup. The mean number of psychotropic drugs administered was 1.45 (range: 1–6 drugs) at the time of describing the plan sheets for lactation by pregnant women. Fifteen women did not take any psychotropic drugs other than LTG. The diagnoses were as follows: epilepsy (n = 14) and bipolar disorder (n = 6). One pair discontinued breastfeeding at 14 days after delivery because of pain in mother's nipples. The gestational age at delivery was 38.8 weeks (range: 37–41 weeks), and no infants were born pre-term and post-term. The number of male and female infants was 14 and 6, respectively. More infants were exclusively breastfed compared with the number of infants who were given mixed feeding in the LTG group. The average infant's birth weight was 3,062 g (range: 1,916–4,110 g) and included one infant with low birth weight. The average BW at 1-month checkup was 4,165 g (range: 3,162–5,172 g). We were unable to obtain the data for one infant. The average weight gain from birth to 1-month checkup was 1,100 g (range: 512–1,746 g). The exclusive breastfeeding rate was 55%. The mean value of BMI of mothers (p = 0.028) and nutrition methods of infants (p = 0.0082) were significantly different between the groups.
Comparison of Lamotrigine Group and Control Group
Statistical methods: *Unpaired t-test, **Mann–Whitney U-test, †Chi-square test, ‡Fisher's exact test.
BMI, body mass index; BW, body weight; Ex, exclusive breastfeeding; LTG, lamotrigine; Mix, mixed feeding; NWS, neonatal withdrawal syndrome.
AEs of infants in the LTG and control groups
There were no infants with an NWS score of 8 or more at any point of evaluation (Table 2). AEs after birth to 1 month after delivery were as follows: drowsiness (n = 3), skin rash (n = 11), jaundice (n = 8), heart murmur (n = 1), poor suckling (n = 1), and retractive breathing (n = 1). It was observed that most children had some skin conditions such as jaundice or skin rash; a few infants received phototherapy for the treatment of jaundice. However, there was no association established to indicate that jaundice was caused by LTG consumed during lactation in MRs. None of the cases discontinued lactation or medication for infants because of AEs. There were no significant differences in the number of reactions between the AEs in the LTG and control groups.
Discussion
In this study, we evaluated the safety of taking LTG during lactation. The descriptions regarding the safety of taking LTG during lactation period differ among information sources.8,9 The reason for this difference is that the systematic evaluation of the safety of lactation is difficult owing to limited human data. The results of our research contribute toward the improvement of the accuracy of safety assessment.
It has been reported that the estimated dose of LTG for infants through breast milk is ∼0.2–1.0 mg/kg/day in previous studies.23,24 According to Japanese package inserts, the therapeutic dose of LTG for children with epilepsy is 1–10 mg/kg/day, and the LTG dose through breast milk is close to the therapeutic dose. It is possible that the blood concentration of infants reaches the therapeutic range depending on the expression of UGT1A4, which is the main enzyme involved in the metabolism of LTG. It has been reported that the activity of UGT1A4 at birth is <50% to that of the adult population.15,25 In other studies, genetic polymorphism of the enzyme, UGT1A4*3, is known to be associated with the glucuronidation of LTG 26 and is present in 32% of Japanese population. 27 It has been reported that taking LTG through breast milk causes elevation in the infant plasma concentration of LTG to within the therapeutic range.16,28
In our study, there were significant differences in maternal BMI and nutrition methods between the two groups and mothers in the LTG group tended to receive a greater number of psychotropic drugs than mothers in the control group. The LTG group more frequently contained mothers with low BMI, compared with the control group. It was thought that the mothers with low BMI tended to receive relative high dose of drugs per volume of distribution, which could increase the amount of drugs contained in breast milk. The LTG group contained many infants who received exclusive breastfeeding. Therefore, those infants who breastfed exclusively would receive more breast milk with LTG than those who did not. Considering these backgrounds, infants in the LTG group probably receive higher amount of the drugs. However, there was no significant difference in the incidence of AEs. Therefore, we concluded that receiving LTG is unlikely to increase the occurrence of AEs in infants.
According to the results of a representative birth cohort study, the weight gain 1 month after birth was 1,098.7 g, which is almost similar to our result. 29 In our study, there was one infant who gained only 512 g. It was described in the MR that the infant tended to sleep after birth and could not continue sucking for a long time. This process might contribute to poor weight gain. The mother was taking six psychotropic drugs for the treatment of diseases, such as bipolar disorder, and the effects of using multiple drugs on infant cannot be ruled out. Tomita et al. reported that infants breastfed from mothers taking three AEDs (LTG, gabapentin, and clobazam) became lethargic and were hospitalized. 30 These symptoms could have been caused by AEDs administered through breast milk. Our research suggests that consuming LTG through breast milk has little effect on the infants' BW gain if the mothers used the drug as a single agent. However, the medical staff must evaluate infants' weight gain in case mothers use LTG with other psychotropic drugs. There were no descriptions regarding infants' symptoms or therapy associated with platelet increase in MRs in our study. It was assumed that there were no cases of severe thrombocytopenia. Newport et al. reported that lactation with LTG caused mild elevation in platelet count in seven of eight infants (average maternal LTG dose: 386.5 mg/day), although the theoretical infant dose (0.51 mg/kg/day) was lower than the therapeutic dose (1–10 mg/kg/day) and the relative infant dose (9.2%) was <10%. 13 It is considered that asymptomatic secondary thrombocytosis does not require platelet reduction therapy. 31 However, it is necessary to observe the occurrence of certain symptoms, such as blood coagulation and bleeding, in infants to differentiate from essential thrombocytosis.
Retractive breathing is a symptom associated with infant respiratory distress syndrome (IRDS). The known risk factors of IRDS are as follows: premature birth, male infants, elective caesarean section, small for the gestational age, severe birth asphyxia, and maternal–fetal infection. 32 Male sex was the only risk factor that was matched in the infant. The infant did not have a severe respiratory disorder. However, severe apnea requiring resuscitation was reported in a 16-day-old infant whose mother took a high dose of LTG (850 mg/day); the infant's blood concentration of LTG was 4.87 μg/mL, which was within the therapeutic concentration range (2.5–15 μg/mL). 16 The apneic episode was caused because of consuming LTG through breast milk. Serious AEs can occur in infants depending on the background such as maternal LTG dose, although 850 mg/day was much higher than the approved adult dose of LTG in Japan (maximum dose: 400 mg/day). Observation of respiratory symptoms over a period of time may be necessary regardless of the maternal LTG dose.
Infants who received a high dose of LTG did not experience severe AEs in our study. In addition, it is known that several drugs induce changes in glucuronidation of LTG during the process of metabolism. In this study, one maternal participant took drugs, phenobarbital and valproic acid (VPA), which caused drug interaction with LTG. Phenobarbital induces the activity of UGT1A433 and reduces the serum concentration of LTG. 7 However, VPA inhibits the metabolism of LTG.34,35 It is possible that the effects of these drugs were offset. Medical staff should pay special attention to infants of the mothers under the following conditions: (1) if taking a high dose of LTG and (2) if taking VPA in combination with LTG.
As Horiguchi and Bauer reported that the physiological incidence of jaundice is 57.39% in Japanese newborn infants, 36 the prevalence of jaundice in our research was not so high. We considered that taking LTG through breast milk is unlikely to affect the increase in infants' jaundice. In addition, many infants had skin rash and one infant was prescribed topical preparations (steroid and antibiotics). Their skin rash did not correspond with common symptoms in Stevens–Johnson syndrome such as blisters on lips or in mouth, fever, and other systemic symptoms. Pediatricians did not prescribe the medicine continuously and referral to a dermatologist was not done. After using the medicine, infants' skin symptoms recovered. Thus, it is considered that skin rash was not severe. Kutlubay's publication suggests that skin rash is a common symptom in newborns 37 ; however, that it is important to recognize serious skin disorders.
This study has several limitations: (1) there were six infants whose NWS scores were not recorded. Our study is a retrospective study based on MRs. Therefore, the NWS scores were not found in the MRs as the infants had no symptoms associated with NWS, although medical staff evaluated the infants' condition. (2) The concentration of LTG in breast milk and infant blood was not measured. In particular, blood sampling is invasive to infants. It would not have been necessary to measure the concentration as none of the infants experienced severe AEs. Therefore, we could not evaluate the relationship between LTG concentration in these samples and infant safety, and it needs further consideration. (3) We could not investigate the long-term safety of the infants. Therefore, these data must be carefully interpreted, and further research is needed. (4) We could not examine the gene polymorphism of UGT1A4. Although no infants had severe clinical problems, as mentioned earlier, 32% of the Japanese population showed enzyme polymorphism. 27 It is necessary to observe the condition of infants during the lactation period.
Conclusion
Our study shows that taking <400 mg/day of LTG during lactation may not cause serious AEs in infants, at least for the period of 1 month after delivery. Thus, the results of this study provide important information regarding the safety of LTG administration in breastfeeding mothers.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This research was partly supported by a grant from the Japan Society for the Promotion of Science (18H00431).