
Abstract
Introduction:
Human donor milk is widely used to feed premature and sick newborns when the milk of their own mothers is insufficient. All treatment processes involving human milk affect its composition. The aim of this study was to assess changes in the macronutrients and bioactive protein (lactoferrin and lysozyme) content in human milk caused by freezing and Holder pasteurization.
Materials and Methods:
Milk samples were collected from 42 mothers 14–16 days after delivery. Each sample was divided into two parts and tested twice for macronutrient content, once upon being freshly collected and again after freezing at −40°C, thawing and Holder pasteurization. The lysozyme and lactoferrin concentrations were first determined in the unpasteurized thawed human milk after it was stored frozen at −80°C for up to 10 months and again after Holder pasteurization. The macronutrient concentrations were determined by midinfrared spectrophotometry, and enzyme-linked immunosorbent assay was used to measure the lysozyme and lactoferrin concentrations.
Results:
Freezing and Holder pasteurization had no significant effects on the macronutrient concentrations. The mean lactoferrin content before and after pasteurization was 2.5 ± 1.07 and 0.03 ± 0.03 mg/mL, respectively (p < 0.001), and the lysozyme content was 19.57 ± 20.11 and 12.62 ± 14.14 μg/mL, respectively (p = 0.007).
Conclusions:
Freezing and Holder pasteurization did not decrease the nutritional value of human milk but caused considerable loss of lactoferrin and lysozyme. New methods for treating human milk are needed that ensure the destruction of pathogenic microorganisms while retaining the biological and nutritional value of the milk. The Clinical Trial Registration number: NCT04382989.
Introduction
Human milk is the optimal food for infants and not only due to its nutritional content. Human milk contains a broad spectrum of biologically active components that play an important role in the body and meet other needs of the growing infant, in particular, protection against infectious diseases and maturation of the immune, intestinal, central nervous, and other body systems.1–3 There is currently no doubt that fresh human milk is the best food for newborns and infants.4–6 Unfortunately, a mother's milk may sometimes be unavailable or insufficient due to maternal health, various perinatal complications, insufficient lactation, or other reasons.
Human donor milk should be the second choice for feeding preterm and sick infants when the mother's own milk is unavailable or insufficient. 7 Human donor milk should be obtained from human milk banks where donors are strictly selected and screened and donated milk is specially treated and inspected to determine its bacteriological content and nutritional value. Donor milk is usually pasteurized, then frozen and stored as such until the time of use.7–10 Holder pasteurization (heating at 62.5°C for 30 minutes) is the most commonly used method in human donor milk banks. After treatment, donor milk is a completely safe food for infants, but it is not equivalent to fresh human milk because pasteurization destroys not only pathogenic bacteria and viruses but also almost the whole microbiota of human milk.11,12 In addition, all procedures performed on human milk (transfer of milk to different containers, refrigeration, freeze–thaw cycles, pasteurization, and others) affect its nutrient and biologically active component compositions.7,13,14 As data from the literature on the effects of freezing and Holder pasteurization on the composition of human milk are quite contradictory, it is not yet completely clear which components of human milk are affected most by these processes and to what extent they are affected.
We hypothesized that freezing and Holder pasteurization change the compositions of macronutrient and bioactive protein in human milk. The aim of our study was to assess how freezing and Holder pasteurization affect macronutrients (proteins, fats, and carbohydrates), energy content, and bioactive protein (lactoferrin and lysozyme) concentration in human milk.
Materials and Methods
This study was conducted at the Neonatology Centre of Vilnius University Hospital Santaros Klinikos from October 2017 to July 2018. The study was approved by the local bioethics committee (permission No. 158200-17-925-443). All the women signed informed consent forms to participate in this study. The study enrolled healthy unmedicated women who were unable to breastfeed due to premature birth, an ill newborn, or other reasons but who were expressing milk. Only mothers whose expressed milk that was in surplus to their babies' nutritional needs during the study period were enrolled in the study. Breastfeeding women were excluded from the study to avoid adverse effects on natural feeding. Other exclusion criteria were maternal chronic infections (tuberculosis, hepatitis B and C, or HIV), oncologic diseases, diabetes mellitus, milk expression by hand, and a history of multiple pregnancies.
A flow diagram for this study is shown in Figure 1.

Procedure diagram. HM, human milk; V, volume per sample (mL); n, number of samples.
Human milk samples were collected for 24 hours on days 14 to 16 after delivery. Milk was expressed from one or both breasts with an electric or mechanical breast pump until the breast(s) were fully emptied. Women admitted to the neonatal unit to nurse their babies normally express milk every 3 hours, that is, seven to eight times a day. Women were asked to place a 10-mL milk sample from each portion of expressed milk (the milk was still warm, unsettled, and well mixed by rotation) into a sterile plastic container for testing. The remaining expressed milk was used for infant feeding. After each expression, the milk samples were drawn into syringes and stored in a refrigerator for ∼1 hour before being placed into a test container to ensure a uniform temperature of the milk collected at different times. Milk samples with a volume of 70–80 mL were collected daily and stored in the refrigerator at +4°C (for ∼24 hours from the start of collection) until nutrient analysis. A total of 42 human milk samples were collected from the mothers of 22 preterm infants (gestational age <37 weeks) and 20 term infants (gestational age ≥37 weeks).
Macronutrient composition was tested twice, once in freshly collected human milk and again in thawed pasteurized milk. A volume of 10 mL was taken from the daily sample of freshly collected milk (well mixed by rotation), and the nutrients were analyzed using the Miris Human Milk Analyser (Miris AB, Sweden), which is based on midinfrared spectrophotometry. Before analysis, the milk samples were heated to 40°C in a water bath according to the Miris analyzer manufacturer's recommendations and were then homogenized using an ultrasound homogenizer (Miris Sonicator).
The concentrations of bioactive proteins (lactoferrin and lysozyme) were also measured twice, once in unpasteurized thawed human milk and again in pasteurized human milk. Volumes of 10 mL from the daily sample of freshly collected human milk were placed in separate plastic containers, and the samples were transported to the hospital laboratory on ice and centrifuged at 500 g, at 4°C, for 15 minutes. The supernatant was stored at −80°C until testing by enzyme-linked immunosorbent assay (ELISA).
The remaining part of the daily milk sample (50–60 mL) was kept at −40°C in a freezer until pasteurization and then repeatedly assayed for macronutrient content and by ELISA to measure lactoferrin and lysozyme concentrations (Fig. 1). The pasteurizer PAS 10000/1 (HSC, France) was used for milk pasteurization. The night before pasteurization, all the frozen human milk samples were thawed at +4°C overnight in a refrigerator. Another 10 mL of milk was collected from each sample after Holder pasteurization for repeated measurements of nutrient composition using the Miris analyzer. The remaining pasteurized milk was delivered to the hospital laboratory on ice to be immediately analyzed to determine the lactoferrin and lysozyme concentrations. ELISAs were simultaneously performed for pasteurized milk samples and thawed unpasteurized samples (using one ELISA kit each for the analysis of lactoferrin and lysozyme).
Samples were collected for 10 months until pasteurization and analysis by ELISA. Lactoferrin concentration was measured with ELISA using the commercial Human Lactoferrin ELISA kit (BIOVendor, Czech Republic). The minimum concentration that could be measured was 1.1 ng/mL. The samples were tested at a 100,000-fold dilution. The lysozyme concentration was measured by means of ELISA using the commercial CircuLex Human Lysozyme ELISA Kit (MBL, Japan). The minimum concentration that could be measured was 23.0 pg/mL, and the samples were diluted 500,000-fold. Intra-assay precision for the assessment of lactoferrin and lysozyme was 3.1% and 5.7%, and the interassay precision was 5.6% and 6.0%, respectively.
After completion of all the tests, the content of macronutrients, energy, and bioactive proteins (lactoferrin and lysozyme) in human milk was compared before and after Holder pasteurization.
Open-source R version 3.5.2 was used for statistical analysis. Quantitative indicators were assessed based on calculation of the arithmetical mean, median, and standard deviation. The t-test or Wilcoxon criterion was applied to compare two related samples. Differences were considered statistically significant when the p-value was <0.05.
Results
A total of 84 paired human milk samples were analyzed. The characteristics of the women enrolled into the study are given in Table 1. No statistically significant differences were found between the groups of preterm and term mothers with respect to infant gender, method of birth, maternal age, or parity.
Comparative Characteristics of Study Participants
CS, cesarean section; GA, gestational age; Md, median; n, no. of group participants;
Holder pasteurization did not significantly affect the mean concentration of macronutrients or energy content in human milk (Table 2). However, Holder pasteurization did significantly reduce the concentrations of lactoferrin and lysozyme (difference of >99% and 35%, respectively) (Fig. 2).
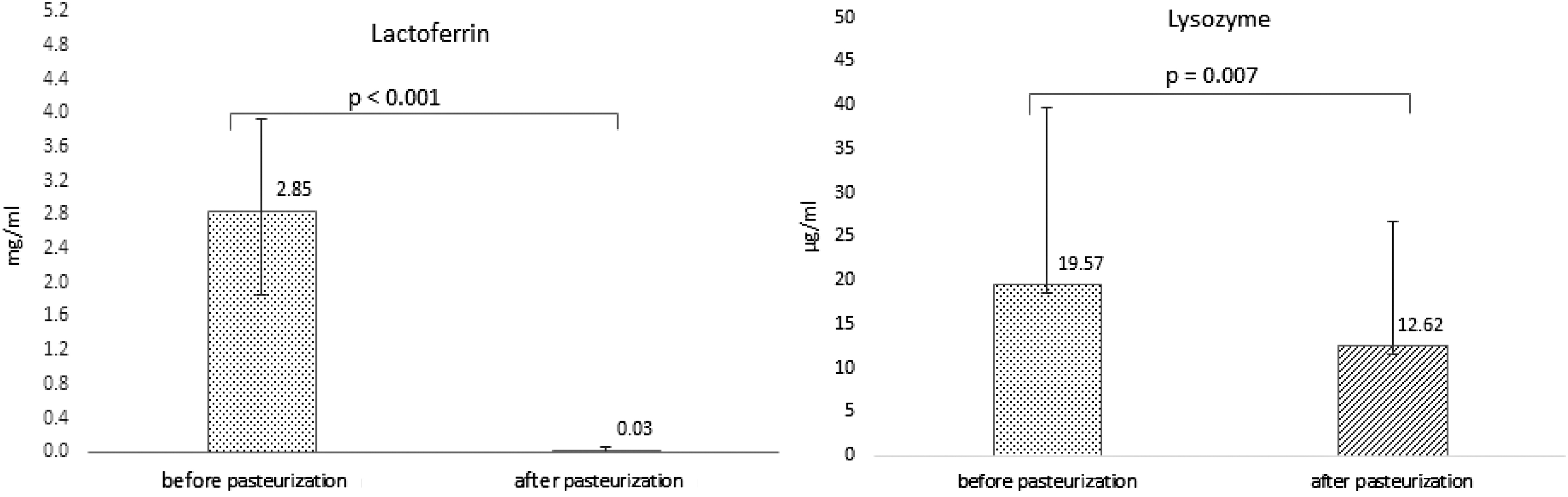
Lactoferrin and lysozyme concentrations before and after Holder pasteurization (n = 42).
Difference in the Mean Macronutrient Concentrations in Human Milk Before and After Holder Pasteurization (n = 42)
Discussion
The quality of human donor milk, as well as the maximum retention of its biological and nutritional properties during the treatment process, is a highly relevant issue today. Pasteurized donor milk is not equivalent to fresh human milk with respect to its properties. Despite numerous studies carried out to date that have estimated the effects of freezing and Holder pasteurization on the composition of macronutrients and bioactive components of human milk, the results are quite different or even contradictory. A summary of 44 articles 15 demonstrated that Holder pasteurization has the highest effect on the composition of bioactive components in human milk. Inconsistent findings from previous studies could be explained by the duration and temperature at which milk samples are stored before pasteurization,16,17 by the method of thawing, 18 by the quantities of milk being pasteurized, by the choice of equipment for Holder pasteurization,15,19 and finally by the method used to prepare the milk samples for testing. 20
Our study has demonstrated that the storage of frozen human milk at −40°C up to 10 months, followed by thawing and pasteurization, has no significant effect on macronutrient (protein, fat, and carbohydrate) or energy content of human milk. According to previous studies, Holder pasteurization of human milk does not affect carbohydrate content but may lead to reductions in fat and protein, although the given results are discordant.8,15 These differences in findings could be partially explained by the prepasteurization storage of human milk samples because not only pasteurization but also freezing influences human milk composition. 21
Freezing and thawing can alter the fat globule structure in human milk, promoting fat aggregation and adhesion to the walls of the containers used. Moreover, proteins are likely to be absorbed into the membranes of disrupted fat globules. 18 It was also reported that human milk lipase activity is maintained at a milk storage temperature of −20°C, resulting in active lipolysis and lipid content reduction. 22 Orbach et al. described a relationship between lower freezing temperatures and reduced loss of fat content in human milk. 16
Furthermore, the methods of collection and preparing the milk samples for macronutrient analysis may affect the results. 23 Common problems faced when handling milk samples are creaming and adherence of fat to container walls, and it is influenced by the surface-to-volume ratio of containers used. It is more pronounced in smaller sample containers compared with larger containers. 23 There is also evidence that milk homogenization before analysis ensures representative results.20,23,24
Overall, however, even though some studies indicate that several nutrients are altered by Holder pasteurization, researchers rarely consider these nutritional changes to be clinically relevant.8,25 In our study, the unchanged nutrient content of thawed pasteurized milk compared with fresh human milk can be explained by the fact that the milk samples were stored frozen at low temperature (−40°C) and homogenized before Miris analysis.
According to the data in the literature, lactoferrin accounts for ∼15–20% of the total protein content in human milk, with lactoferrin concentrations being the highest in colostrum (∼5.05 mg/mL) and then gradually decreasing thereafter (to 3.3 mg/mL in transitional milk and 1.44 mg/mL in mature milk on average). 26 Our mean lactoferrin concentrations in unpasteurized transitional human milk (2.845 ± 1.07 mg/mL) are close to those reported by other sources.26,27 We found that lactoferrin was almost completely degraded after Holder pasteurization (by >99%), whereas other studies reported a 35–90% loss of this bioactive protein. 15 In our study, all the milk samples were Holder pasteurized simultaneously. This process was performed in strict accordance with the manufacturer's recommendations and was controlled by a computer, and no temperature regime violations were reported. After pasteurization, the samples were immediately delivered to the laboratory for ELISA analysis. Accordingly, our findings revealed that lactoferrin loss caused by Holder pasteurization may be even higher than reported by other studies.
According to previous studies, the average lysozyme concentration is 0.32 mg/mL in colostrum and ranges from 0.28 to 1.1 mg/mL in transitional and mature human milk. 26 We found significant individual variations in the lysozyme concentration in transitional human milk (19.568 ± 20.11 mcg/mL), which are lower than those reported in some studies,26,27 but similar to results obtained by Hsu et al. 28 We speculate that the reduction in the lysozyme concentration in the prepasteurized thawed human milk samples could be caused by freezing the human milk and its storage time until pasteurization. According to Chang et al., freezing human milk at −20°C for a prolonged period results in a significant reduction in lysozyme content (by as much as 39.8%), whereas freezing-induced lactoferrin loss in human milk was only 11.5%. 29 In contrast, we found a 35% reduction in lysozyme as a result of Holder pasteurization, which is consistent with results from previous studies. 15
Strengths and limitations of this study
Our study is useful for supplementing the data described to date on the effects of freezing and Holder pasteurization on the composition of human milk. The sample size is rather large compared with previous studies published on this topic.
Unfortunately, we cannot distinguish between the effects of freezing, the duration of storage, and Holder pasteurization on the macronutrient, lysozyme, and lactoferrin contents in human milk. Understanding the contribution of each of these processes to these effects would allow the selection of optimal methods for human milk processing to minimize the loss of nutrients and bioactive components.
As homogenization was not performed each time after milk expression, but milk was only mixed by rotation, we cannot absolutely rule out the possibility of milk creaming and adherence of fat to container walls during milk transfer to different containers, possibly resulting in some fat loss. This is also the limitation of our study. In contrast, the main task of our study was to evaluate the changes in macronutrient composition of human milk due to freezing and pasteurization but not the absolute values of the macronutrient content.
Conclusions
Freezing and Holder pasteurization had no significant effects on the nutritional content of human milk but caused considerable loss of biologically active proteins (lactoferrin and lysozyme). To improve the quality of human donor milk, new methods for human milk treatment and optimal conditions of milk storage need to be identified that ensure the destruction of pathogenic microorganisms while retaining the biological and nutritional value of the milk to the maximum extent possible.
Footnotes
Acknowledgments
We are grateful to the staff members of the Vilnius Donor Milk Bank for their technical assistance in performing human milk analysis.
Disclosure Statement
No competing financial interests exist. This research was conducted as a part of I.J.P.'s doctoral studies at Vilnius University.
Funding Information
Funding for the analysis of lactoferrin and lysozyme by the ELISA method was granted by the Vilnius University, grant number: 300949340.