
Abstract
Purpose:
The protocol for postoperative follow-up time after lingual frenotomy in breastfeeding infants with ankyloglossia was changed from 2 weeks to 1 week at our institution. This study examined the impact of this change in practice on frenotomy revision rate.
Materials and Methods:
A retrospective chart review of breastfeeding infants who underwent lingual frenotomy for ankyloglossia from January 2016 to December 2017 was performed. Subjects were divided into 1-week (1–9 days) and 2-week (10–20 days) follow-up groups. Statistical analyses were performed to investigate the relationship between revision rate and postoperative follow-up time, as well as additional patient characteristics.
Results:
Of the 369 patients included in the study, 34 (9.2%) underwent frenotomy revision. The individual revision rates of the 1- and 2-week follow-up cohorts were 5.2% and 12.7%, respectively. The difference in revision rate was statistically significant (p = 0.022), and logistic regression revealed the odds of revision for the 2-week cohort to be 2.67 times (95% confidence interval: 1.207–5.918) greater than the 1-week cohort (p = 0.015).
Conclusion:
This study demonstrates a significant association between a shorter postoperative follow-up time and decreased frenotomy revision rate. With earlier follow-up, manual adjustment can be performed sooner in the postoperative period as needed, which may prevent scarring or healing complications that usually necessitate full revision. Our findings support a shift to a shorter postoperative follow-up time as a means of improving frenotomy outcomes.
Introduction
Ankyloglossia, also known as “tongue-tie,” is a condition in which the lingual frenulum restricts the range of motion, mobility, and function of the tongue because of abnormal length or thickness. 1 The lingual frenulum is defined anatomically as a midline tissue of fascial fibers that extends anywhere from the apex to the submucosa of the ventral tongue and attaches to the floor of the mouth.
The prevalence of ankyloglossia has been reported between 2.1% and 10.7%. 2 The exact etiology remains unclear, but a genetic predisposition suggested as a male predominance has been observed in multiple studies. 3 Infants with ankyloglossia can have feeding difficulties because of restricted tongue movement, which can lead to poor weight gain resulting from insufficient milk transfer during breastfeeding.4,5 The condition can additionally cause problems for the breastfeeding mother, who may experience increased breast pain, nipple damage, and decreased milk supply—all of which are also associated with the infant's inability to correctly latch onto the breast. 6 The prevalence of breastfeeding difficulties in infants with ankyloglossia has been reported to be as high as 80%. 7
The impact of ankyloglossia on tongue movement and breastfeeding ability is critical for both diagnosis and the decision to proceed with frenotomy, an outpatient procedure in which the frenulum is divided using instrumentation. 1 Release of the frenulum allows for increased range of tongue motion and can result in improved breastfeeding abilities for both the infant and mother.5,8,9
Reviewing best practices for frenotomies has never been more relevant than the current times. For the past 20 years, the diagnosis of ankyloglossia and subsequent treatment with frenotomy have increased >800%. 3 However, controversy regarding frenotomy efficacy exists owing to differing literature reports and few well-established prospective cohort studies and randomized control trials.3,7,10 Although some systematic reviews have supported frenotomy as an effective intervention for both infants and mothers experiencing ankyloglossia-related breastfeeding difficulties,6,11 others report that the benefit of frenotomy still remains unclear because of low strength of evidence in existing studies; small sample sizes and flawed methodological approaches render the current data inconclusive.2,7,12 As the efficacy of frenotomy still remains a relevant debate, the need for additional research is clear. More data on frenotomy practices are necessary to establish better evidence-based guidelines for treatment protocols.
Very few studies have been conducted to specifically investigate recurrent ankyloglossia and factors that influence frenotomy outcomes. This study aims to address both the aforementioned topics by analyzing how changes in postoperative follow-up time influence frenotomy revision rate. Before 2017 at our institution, the first follow-up status postlingual frenotomy was normally scheduled for 2 weeks after the procedure. In January 2017, a 1-week postoperative follow-up time was adopted by the senior author. The change in practice was implemented after the anecdotal observation that patients who followed-up earlier than 2 weeks tended to have a lower revision rate; the reduction was attributed to easier manipulation of the incision site before complete wound healing occurred, subsequently preventing the need for full revision.
This study was conducted to test the hypothesis that a 1-week postoperative follow-up time would lead to a decrease in revisions compared with a 2-week follow-up. Overall, we aim to examine how this change in practice influenced frenotomy revision rate and to identify what patient characteristics may be associated with improved frenotomy outcomes—with the hope that our findings may guide future clinical practices, reduce health care costs associated with revision, and improve the breastfeeding experience of both infants and mothers.
Materials and Methods
A retrospective chart review was completed for breastfeeding infants who underwent a lingual frenotomy by the conventional technique using tenotomy scissors at the Pediatric Otolaryngology Tongue-tie and Breastfeeding Clinic at Medstar Georgetown University Hospital. Expedited review and approval to perform this study was received from the Georgetown-Medstar Institutional Review Board. Additional study inclusion criteria included a diagnosis of ankyloglossia and a procedure date between January 1, 2016 and December 31, 2017. None of the included frenotomy cases was performed using laser technique. Exclusion criteria removed patients who followed up at 21 days or longer postoperatively, patients who were lost to follow-up completely, and patients who pursued bottle-feeding instead of breastfeeding status after frenotomy (as a frenotomy revision would not be considered for patients who are no longer breastfeeding) (Fig. 1).
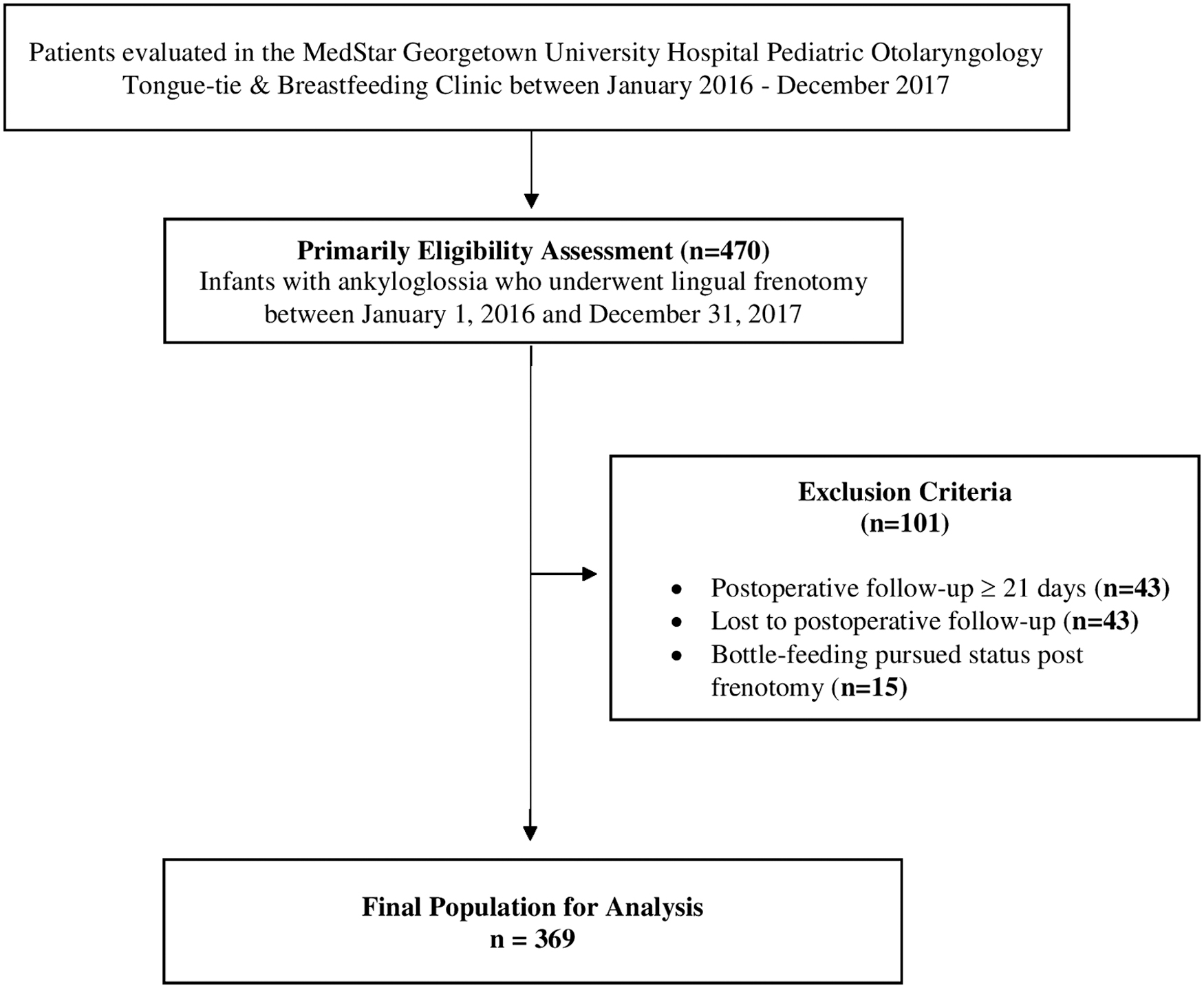
Flowchart depicting study inclusion and exclusion criteria. Subjects who met the primary eligibility assessment criteria (n = 470) were identified using electronic medical records. Exclusion criteria removed 101 subjects owing to a postoperative follow-up time of ≥21 days (n = 43), lack of postoperative follow-up (n = 43), and bottle-feeding status (n = 15). In total, 369 subjects were included in the study.
Upon chart review, the following data points were collected: age, gender, ethnicity, ankyloglossia classification, family history of ankyloglossia, time (in days) to initial postoperative follow-up appointment, and whether or not a revision frenotomy was performed. Ankyloglossia classification was established using the Coryllos criteria, which identifies four different types of ankyloglossia based upon the location of frenulum attachment relative to the tip of the tongue. 13
Univariate analysis was conducted to primarily examine the relationship between revision rate and postoperative follow-up time. Patients were divided into two separate groups based upon the number of days between their procedure date and initial postoperative follow-up appointment: Group 1 was classified as the “One-Week” follow-up cohort and included patients who were seen 1–9 days postoperatively, and Group 2 was classified as the “Two-Week” follow-up cohort and included those who were seen 10–20 days postoperatively. This grouping was designed to reflect the change in postoperative follow-up protocol that was implemented at our institution between 2016 and 2017. The cohorts were designated based upon a range of days rather than precise time points (i.e., 10–20 days versus 14 days) because of the variable nature of appointment scheduling. Any patient who followed up postoperatively at 21 days or longer were excluded from the study.
Univariate analysis was also performed to investigate the relationship between revision and other patient characteristics such as age, gender, ethnicity, ankyloglossia classification, and family history of ankyloglossia. All variables found to be statistically significant (p < 0.05) were further analyzed using a logistic regression model that was built with revision as the outcome of interest.
Results
A total of 369 breastfeeding infants who underwent lingual frenotomy by conventional technique between January 1, 2016 and December 31, 2017 were included in the study. A total of 172 (46.6%) patients followed up postoperatively within the 1-week time period (Group 1), whereas 197 (53.4%) followed up within the 2-week time period (Group 2). Table 1 details the patient demographics and ankyloglossia classification.
Demographics and Characteristics of Lingual Frenotomy Patients
IQR, interquartile range; SD, standard deviation.
Frenotomy revision was performed for 34 (9.2%) patients overall. A total of 9 (5.2%) patients underwent revision in Group 1, and 25 (12.7%) patients underwent revision in Group 2. The difference in revision rate between the two groups was statistically significant (p = 0.022). Patient age (in days) was also found to be significantly different between subjects who underwent revision and those who did not (14.9 days versus 20.7 days, respectively; p = 0.029). No significant associations were found between revision rate and the other independent variables of gender, ethnicity, ankyloglossia type, and family history of ankyloglossia (p > 0.05) (Table 2).
Frenotomy Patient Demographics and Characteristics Organized by Revision
IQR, interquartile range; SD, standard deviation.
When age and follow-up group were further analyzed with logistic regression, follow-up time was found to be a significantly predictive indicator of frenotomy revision rate. The odds of revision for Group 2 was 2.67 times (95% confidence interval: 1.207–5.918) greater than the odds of revision for Group 1 (p = 0.015). Logistic regression did not find patient age to be a prognostic factor for revision (p = 0.076), despite its initial significance in the univariate analysis.
Discussion
Although the efficacy of lingual frenotomy for infants with ankyloglossia-related breastfeeding issues has been studied numerous times and continues to be a source of debate in the literature,4–11 there is a much more limited body of research focused on identifying specific variables that impact frenotomy outcomes. In an effort to expand the current evidence on this topic, this study sought to provide more data on frenotomy revision and postoperative practice protocols associated with improved frenotomy outcomes.
Earlier studies have reported rates of lingual frenotomy revision (in infants) ranging between 2.6% and 13%.14–16 Our results fell within this range and were consistent with the previously documented numbers: the overall revision rate for our subjects was 9.2% (34 of 369 infants). Within the 1- and 2-week follow-up groups, the revision rates were 5.2% (9 of 172) and 12.7% (25 of 197), respectively.
One result that was not consistent with previous reports in the literature, however, was the lack of association between ankyloglossia type and frenotomy revision rate. In a 2010 study by Hong et al., posterior ankyloglossia was correlated with a significantly higher rate of revision compared with anterior ankyloglossia. 17 In this study, none of the ankyloglossia types (Coryllos types 1–4) were found to have a significant association with revision rate. The dichotomy between these results may be owing to a number of factors, including the use of differing ankyloglossia classification schemes and an uneven distribution of ankyloglossia types in both studies. Neither result is conclusive, and additional research on the impact of ankyloglossia type on frenotomy revision rate is indicated.
The most remarkable finding of our study was the prognostic correlation demonstrated between postoperative follow-up time and revision rate. Our analysis revealed that a 2-week follow-up time is associated with a 2.67 times greater likelihood of revision compared with a 1-week follow-up time (p = 0.015). This finding is hypothesized to relate to the clinical tasks that take place during the initial postoperative visit—namely frenotomy site inspection and manual adjustment (performed as needed).
The lower number of revisions seen with the shorter follow-up period may be explained by the procedure site's greater amenability to manual adjustment when performed by approximately 1 week after the original procedure (as was noted in the senior author's original anecdotal observation that prompted this study). The manual adjustment specifically involves use of the thumbs—occasionally assisted with a cotton tip applicator—to lyse any adhesions that are forming underneath the tongue at the procedure site. This manual adjustment can facilitate improved wound healing and prevent formation of unwanted scar tissue, which in turn may prevent the need for formal revision.
In contrast, when postoperative follow-up is performed at 2 weeks, a longer period of wound healing has elapsed and is thought to have progressed to a point where manual adjustment alone would no longer be sufficient to fully correct an impaired recovery because of scar tissue formation (if it were present). As a result, it is possible that the subjects seen at 2 weeks postoperatively were more likely to require revision frenotomy as a consequence of the natural course of wound healing that was not intervened at an earlier time point. This hypothesis is supported by the notably lower revision rate seen in our 1-week follow-up group (5.2%) compared with the 2-week follow-up group (12.7%; p = 0.022), in addition to the significance of the aforementioned odds ratio (OR) analysis. A shorter follow-up time appears to be favorable because it allows for closer postoperative management that decreases the risk of recovery complications and the need for revision.
Although this study is one of the first to document a specific clinical practice protocol that significantly influences frenotomy outcomes, there are several limitations to acknowledge. The design of the study was a retrospective chart review involving patients with natural variability in appointment scheduling, and thus not all patients were able to follow-up at exactly 1- or 2-week time points. To account for this, the designation of patients into each follow-up group cohort had to be based on a range of days (i.e., 1–9 days for the 1-week cohort) rather than a single time point (i.e., 7 days). Although this slight variability may have influenced the comparison between 1- and 2-week time points specifically, our overall analysis still supports the association between a shorter postoperative period and reduced revision rate. Repeat studies with stricter adherence to specific follow-up time points are needed to help strengthen the evidence for this association.
Another limitation to acknowledge is the incomplete inclusion of patient characteristics for a small subset of subjects (n = 8); five patients lacked data for their family history of ankyloglossia, and three patients lacked data for ankyloglossia type. Of note, these cases were included in the general analysis because they still contributed to the data for revision rate—our primary outcome of interest. The few instances of missing data stemmed from a lack of documentation in the electronic medical record system at the time of patient care and is another factor related to the retrospective nature of this study.
A final limitation we recognize is the use of clinical data from two separate time periods (which reflected the change in clinical practice described earlier). We acknowledge the potential bias involved in the use of these temporally separated cohorts, but the bias is minimized, however, by the fact that the operating surgeon and practitioners remained the same throughout both time periods. Furthermore, the frenotomies and postoperative follow-up examinations were performed in the same manner without variation over time. Thus, continuity was maintained for the clinical evaluation and interventions for all subjects in each cohort.
In the future, prospective studies are recommended and would be advantageous for addressing and eliminating the limitations we have discussed. Additional research is necessary to help further elucidate other practice protocols and patient characteristics that may significantly influence frenotomy outcomes.
Conclusion
Our findings identify a significant association between postoperative follow-up time and lingual frenotomy revision rate in breastfeeding infants with ankyloglossia. A shorter follow-up time appears to be associated with a lower number of revisions, as it allows manual adjustment of the incision site to be performed earlier in the postoperative period if needed. This adjustment facilitates optimal healing of the operative site, which in turn helps to prevent scarring or healing complications that may otherwise lead to a need for revision. This holds implications for clinical practice, supporting that a shift in protocol to a shorter postoperative follow-up time may be a means of improving frenotomy outcomes by reducing revision rate.
Footnotes
Acknowledgment
Xue Geng, MS, Department of Biostatistics, Bioinformatics and Biomathematics, Georgetown University Medical Center.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.