
Abstract
Objective:
Mothers of many preterm babies are unable to produce sufficient milk for their babies during the prolonged hospitalization. Domperidone stimulates the release of prolactin, thereby increasing breast milk production. The primary outcome was to study the efficacy of domperidone in augmenting breast milk production in mothers with lactation failure (LF). The secondary outcomes included the effect of domperidone on prolactin levels, adverse effects of domperidone, and outcome on breastfeeding rates at discharge.
Materials and Methods:
This was a randomized, double-blinded, placebo-controlled trial where mothers with LF were either allocated domperidone (10 mg) or placebo, 2 tablets three times a day for 14 days. Milk volumes were recorded daily for 14 days. Serum prolactin levels were measured at the start and at day 7 of study.
Results:
Out of 166 women eligible for the study, 119 (71.7%) mothers were able to increase their breast milk production without pharmacological treatment after being counseled on the advantages of human milk and proper breastfeeding management. Forty-seven mothers were finally enrolled in the study; 24 in the domperidone group (DG) and 23 in the placebo group (PG). Breast milk production increased from a baseline of 156 + 141.1 to 400.9 + 239.2 mL in the DG and increased from a baseline of 175.8 + 150.7 to 260.5 + 237.5 mL in the PG, after 14 days (p < 0.01). The prolactin levels in the DG and PG increased from 72.85 (22.2–167.15) and 42.33 (14.02–93.54) ng/mL, respectively, to 223.4 (49.79–280.2) ng/mL (p = 0.005) in the DG and 60.08 (14.31–132.14) ng/mL (p = 0.232) in the PG on the 7th day of treatment. No adverse effects were recorded. Ninety-five percent of babies in the DG were exclusively breastfeeding at hospital discharge, compared with 52.4% in the PG (p = 0.008).
Conclusion:
Domperidone treatment can result in an increase in breast milk production with no adverse effects. The study was registered with the Thai Clinical Trials Registry ID TCTR2020091008.
Introduction
Human milk (HM) is the gold standard for infant feeding. The short- and long-term benefits of HM for term infants are well established. 1 However, since the last two decades, there has been growing evidence of the dose-dependent benefits of HM for premature babies. These benefits include a decrease in necrotizing enterocolitis, neonatal mortality, sepsis, bronchopulmonary dysplasia, retinopathy of prematurity, rehospitalization after discharge, and improvement in neurocognitive outcomes in vulnerable premature infants.2–9 The World Health Organization (WHO) and the American Academy of Pediatrics (AAP) have recommended own mothers' fresh milk as the feeding of choice for premature babies.
Unfortunately, insufficient milk supply is a frequent reason given by mothers for discontinuing breastfeeding. 10 This is even more evident in mothers who give birth to premature babies that are subsequently admitted to the neonatal intensive care unit (NICU).11,12 Maternal stress, delayed initiation, improper technique and frequency of milk expression, lack of breastfeeding support by the NICU nurses, and absence of a lactation nurse in the NICU can all impact negatively on breast milk production.13–16 Hence, efforts should be made soon after birth to support mothers of premature babies with nonpharmacological measures to enhance and sustain lactation. 17 Nonetheless, despite support, some women do not respond to the nonpharmacological interventions and eventually require some pharmacological galactagogues. Domperidone, a dopamine receptor antagonist, acts by blocking the inhibition of dopamine-mediated prolactin secretion, thereby increasing breast milk production. In a recent systemic review and meta-analyses of 5 trials consisting of 194 women, use of domperidone resulted in a moderate increase in daily breast milk production when compared with placebo. 18 Currently, it is the most frequently used pharmacological galactagogue in the United Kingdom, Canada and Australia, with its use increasing over the last few years.19–21 However, the U.S. FDA has warned breastfeeding women against using domperidone because of its potential to prolong QT interval and increased risk of ventricular arrhythmia and sudden cardiac arrest among nonlactating adults. 22
Domperidone is also frequently used in Thailand to increase breast milk production. Our search for literature only revealed a single study published in Thailand that showed the effects of domperidone on augmentation of lactation. 23 However, in that study, domperidone was used following a cesarean delivery at full term and was given immediately after birth during the first 4 consecutive postpartum days.
The primary aim of our study was to determine the effect of domperidone on breast milk production in mothers with lactation failure (LF). The secondary aim was to study the effect of domperidone on serum prolactin levels and to study any adverse effects of domperidone that may be experienced by mothers. We also aimed to study the effect of domperidone on exclusive breastfeeding at discharge and 1 month after discharge from the hospital.
Materials and Methods
This was a randomized, double-blinded, placebo-controlled trial conducted in the neonatal unit of the Queen Sirikit National Institute of Child Health (QSNICH) between May 2012 and January 2015. The sample size (calculated using data from Campbell-Yeo et al. 24 ) of 60 women, 30 in each group, was obtained using the mean milk volume of study and control groups of 380.2 and 250.8 mL, respectively; standard deviation (SD) of 201.6 mL, power of 80%, and an α level of 0.05. Mothers of babies admitted to the neonatal unit and experiencing LF were eligible. LF was defined as expressed breast milk (EBM) less than 350 mL/day by 14 days postpartum or EBM not meeting the neonate's daily feeding requirements after 7 days of life. All eligible women were counseled on the advantages of HM feeding, instructed on proper HM management including correct milk expression techniques (manual or electrical pumps), frequency of expression (every 2–3 hours by day and at least once at night), and storage of HM. All the women were given a form to record the daily frequency and volume of milk expressed. These mothers were followed daily to verify correct HM management techniques and to clarify any queries that they might have. Finally, all the women who still had LF after having been counseled on HM management and pumping regularly as advised for 5 days were included in the study.
Once recruited and consented, the women were randomized using computer-generated blocks of 4 to receive either domperidone (10 mg: 2 tablets, three times daily) or placebo (identical to domperidone in size, color, and odor) for 14 days. Both domperidone and placebo were purchased from T. Man Pharma Co., Ltd. (Bangkok, Thailand). The tablets were placed in a sealed, numbered brown plastic pack by the pharmacists; the attending physician, investigators, and mothers were blinded to the content of the packet. Each subject was also provided with a personal hospital-grade electrical breast pump (Symphony breast pump with double pump collecting system by Medela, Equip Healthcare Co., Ltd.) and sterile collection bottles for the total duration of the study. Daily pumping frequency, milk volume, and any adverse effects were recorded by the mothers in the record forms provided. The mothers were met by the investigators daily or every other day for 14 days to review the data and any adverse effect that the mother may have been experiencing. If the mothers were unable to come to the hospital, they were contacted by phone and relevant information obtained. All babies admitted to our hospital follow the Spatz model of 10 Steps to successful breastfeeding for the sick and vulnerable baby, 25 which has been the breastfeeding protocol adopted in our unit since 2013. Once stable, all babies are put to breast, first for non-nutritive suckling and then after 34 weeks of gestational age, nutritive suckling. However, during the 14 days of the study intervention, to get the exact volume of milk production, the babies were only put to breast for non-nutritive suckling after the mother had fully expressed her milk. After completing 14 days of the intervention phase of the study, if any mothers were still experiencing LF, they were prescribed open-labeled domperidone 20 mg, three times a day.
Once enrolled in the study, a blood sample for baseline serum prolactin level was obtained from each participant before starting the medication. Another blood sample was obtained on day 7 of treatment. The blood specimens were transferred to the laboratory where the serum was separated and then stored at −70°C. All the specimens were stored together, and prolactin levels were tested at the end of the study by the electrochemiluminescent immunoassay method using the Cobas E 501 automated analyzer, Roach® Diagnostic USA. On the day of discharge from the hospital, the breast milk feeding status was recorded for each neonate and the 1-month postdischarge breast milk feeding status was also obtained by way of phone interview with the mothers.
Excluded from the study were women who had any contraindications for breastfeeding, mothers who had already received domperidone at any time postnatally before recruitment in the study, and infant demise during the study.
Data analysis was performed using the SPSS version 16.0 program. The demographic data were summarized as percentage, mean ± SD, and median. Comparison of the increments of milk from start to day 7 and day 14 within the group and between the groups was analyzed using repeated-measured analysis of variance and independent t-test, respectively. p-Value <0.05 was considered statistically significant. The study was approved by the institution's ethics committee IRB00007346, FWA00002250.
Results
The study was conducted in the neonatal unit of QSNICH from July 2012 to January 2015. A total of 166 women with LF were eligible for the study. After being counseled on the advantages of HM feeding and proper HM management, only 47 (28.3%) mothers were finally recruited; 24 in the domperidone group (DG) and 23 in the placebo group (PG). However, as shown in Figure 1, due to infants' demise and missing milk volume data, milk production was available for only a total of 41 mothers during the first 7 days of the study and 34 mothers for the full 14 days of study. The proportions lost to follow-up in this study were 21% and 35% in the intervention and control groups, respectively. The demographic data (Table 1) were not significantly different between the groups with regard to maternal age, education, previous experience in breastfeeding, neonatal birth weight, and the postpartum day the medication was started.
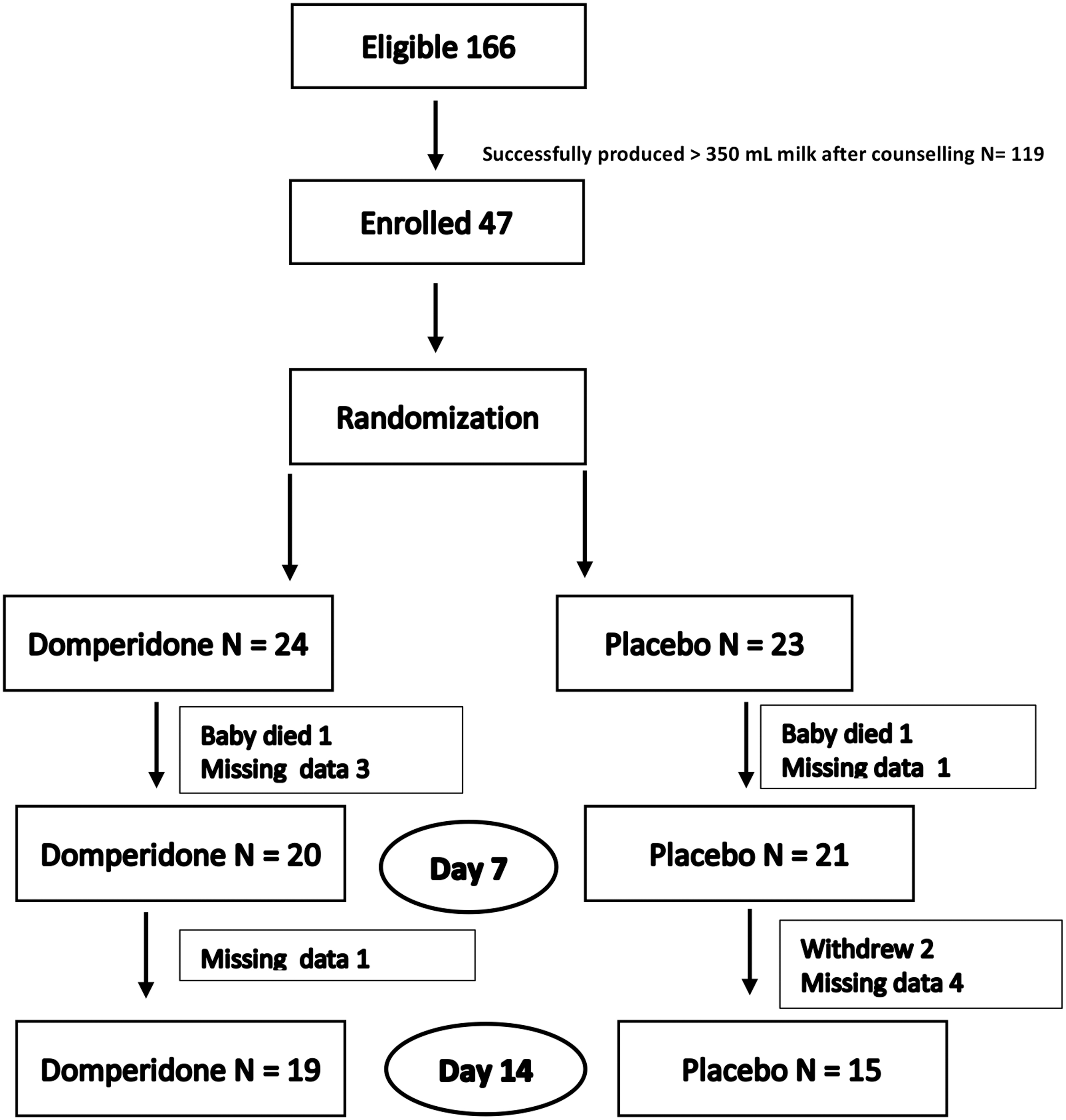
CONSORT diagram. CONSORT, Consolidated Standards of Reporting Trials.
Demographic Data
Chi-square test.
The mean daily breast milk production at the start of study (baseline) was similar in both groups, 150.6 ± 139.8 mL in the DG, while it was 164.7 ± 131.7 mL in the PG. At day 7, the volume of milk increased to 324.8 ± 178.7 mL in the DG and 193.3 ± 178.7 mL in the PG (p = 0.001). This was an increment of 115.7% from baseline in the DG and 17.4% in the PG (p < 0.01). In DG mothers, who had a recorded milk volume for 14 days (N = 19), the daily breast milk production increased from a baseline of 156 ± 141.1 to 400.9 ± 239.2 mL, while it increased from a baseline of 175.8 ± 150.7 to 260.5 ± 237.5 mL after 14 days in the PG (N = 15), p < 0.01 as shown in Figure 2. This was a total increment of 156.3% in the DG compared with an increment of 48.2% in the PG (p < 0.01).
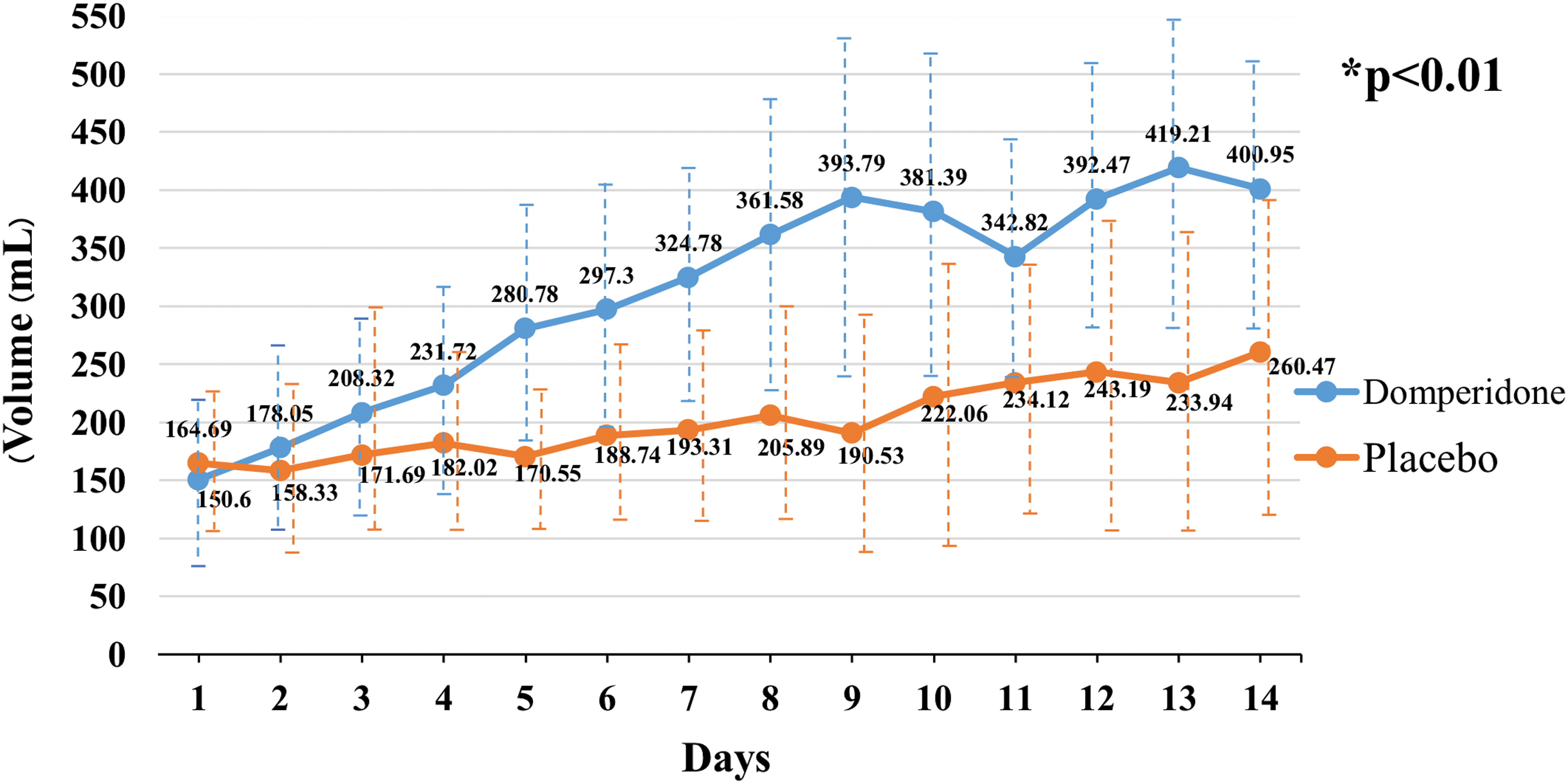
Milk production in 14 days. Data in mean, *repeated-measures analysis of variance, and dotted lines represent 95% confidence interval. Color images are available online.
The median prolactin levels at baseline were not statistically different between the DG (N = 20) and PG (N = 21; 72.85 [22.2–167.15] and 42.33 [14.02–93.54] ng/mL, respectively) p = 0.348. By the 7th day of treatment, the prolactin level had significantly increased in the DG to 223.4 (49.79–280.2) ng/mL (p = 0.005), while it was not statistically significant in the PG 60.08 (14.31–132.14) ng/mL (p = 0.232), as shown in Table 2. There was no statistically significant correlation between the increase in serum prolactin on day 7 of treatment and the serum prolactin level at baseline in both the DG (p = 0.82) and the PG (p = 0.986).
Prolactin Hormone Levels
Median (P25–P75).
Mann–Whitney U test.
Wilcoxon signed-rank test.
None of the women experienced any adverse effects throughout the duration of study. Nineteen of the 20 (95%) babies in the DG received exclusive breast milk feeds (EBM in bottle or direct breastfeeding) on discharge from the hospital, compared with 11 of the 21 (52.4%) in the PG (p = 0.008). However, at 1-month postdischarge, 14 of 20 (70%) were still receiving exclusive breast milk in the DG compared with 9 out of 15 (42.9%) in the PG, which was not statistically significant (Table 3).
Exclusive Breastfeeding at Discharge and 1 Month After Discharge
Fisher's exact test.
Discussion
The use of HM in low birth weight (LBW) and extremely low birth weight (ELBW) babies during their hospitalization is a very important aspect in the care of these vulnerable babies, as evidence shows a definite improvement in outcomes.2–9 However, LF is common in this group of mothers due to a variety of reasons previously mentioned. Supporting breastfeeding should be an essential part of the care plan in the NICU, with each hospital having its own written policy and protocol to ensure the best possible outcomes for the babies.
During this study, a total of 166 women were eligible for the study. However, after being counseled on the advantages of HM feeding and proper HM management, 119 (71.7%) mothers were able to increase their breast milk production without any pharmacological treatment. This emphasizes the importance of maternal support by health personnel in improving breast milk production.
In this study, a higher dose of 60 mg/day of domperidone was used, compared with most other studies that used 30 mg daily dose of domperidone. 26 Our literature search revealed two other studies that also used 60 mg/day dose. One was a small, double-blinded, randomized crossover trial of 6 preterm mothers who received 30 and 60 mg domperidone dose in a three-phase trial compared with a placebo. Even though there was an increase in milk production in both doses compared with placebo in 4 mothers whose milk production was studied, the small size of the study precluded detection of any difference in milk production between the 2 doses. 27 The second study randomized the mothers to receive either 30 or 60 mg domperidone daily. Even though there was a clinical difference between the doses, it was not statistically significant. 28
The mean milk production significantly increased by an increment of 115% in the DG after 7 days of treatment compared with an increment of only 17.4% in the PG. After 14 days, milk production increased further by 156% from baseline in the DG compared with 48% from baseline in the PG, which was also statistically significant. This is similar to the systematic review and meta-analysis where the pooled analysis of 5 trials consisting of 194 women demonstrated a moderate increase in daily milk production after domperidone. 26
Prolactin is critical for lactation, with levels rising during pregnancy to ∼200 μg/L at term and baseline levels remaining elevated in postpartum nursing women. However, as lactation progresses, despite a decrease in suckling-induced mean and peak prolactin levels, there is continued milk production. At the start of this study, the baseline prolactin was similar in both the groups, with levels that were below the term equivalents. However, by the 7th day of treatment, there was a significant difference in prolactin level from baseline in the DG, as well as between both groups.
Surprisingly, despite a higher daily domperidone dose of 60 mg, there was not a single adverse reaction reported during the study period. Speculated reasons for this include cultural inhibitions in presenting adverse reactions, and/or a fear that any complaints could lead to medication being discontinued (despite repeated reassurances to the contrary by the team). Nonetheless, in a systemic review of five trials, there were no differences in the maternal adverse events between the domperidone and PG. The major concern with the use of domperidone is with regard to its cardiac complications. There was no report of prolonged Qtc syndrome or sudden cardiac death in the meta-analysis of five trials. 18 We did not perform electrocardiograms on any mothers during our study to assess for cardiac complications. A large Canadian study on 225,532 women after delivering 320,351 live births identified 21 cases with ventricular arrhythmia, 6 out of 45,518 women exposed to domperidone and 15 in nonexposed women. However, 16 of the 21 women had a history of ventricular arrhythmia, including all 6 women in the DG. 29 From this study, Grzeskowiak and Smithers summarized that the use of domperidone in women with a history of ventricular arrhythmia should be cautioned and only undertaken under careful supervision. 30
An additional, but not surprising, aspect of this study was that when followed, 95% of babies in the DG were exclusively feeding HM at discharge, which was significantly different from ∼52% in the PG. Even 1 month after discharge, although not significant, the DG trended higher toward exclusive HM feeding compared with the PG. However, the difference in exclusive breastfeeding rates between the DG and PG could have been influenced by the open-label domperidone prescription after the original intervention phase. Therefore, the true effect of domperidone may have been underestimated. Hence, earlier support and attention to milk production given to the mothers in an NICU setting may be able to facilitate an increase in exclusive breastfeeding rates in the population.
The study was limited by its small size. Due to financial and time constraints, we were unable to recruit the total number of patients calculated in the sample size. The main reasons for study attrition consisted of refusal to take medication without explicit explanation in 2 mothers in the placebo arm who eventually withdrew from the study, and the failure of the mothers to record breast milk volume in four cases in intervention and five cases in the control arm. In this study, an intention-to-treat analysis was not done, only a “per protocol” analysis of subjects who completed the entire study was performed. Consequently, the results could overstate the effectiveness of domperidone.
Conclusion
The use of HM in LBW and ELBW babies during their hospitalization is a very important aspect in the care of these vulnerable babies. Insufficient milk production in mothers of preterm infants may compromise their care. In cases where there is no response to the nonpharmacological measures to enhance milk production, domperidone treatment can result in an increase in breast milk production with no adverse effects. Increase in maternal milk production during the early postpartum period can result in an increase in the exclusive HM feeding at discharge.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was partially supported by the Perinatal Society of Thailand.