
Abstract
Background:
For extremely low-birth-weight infants (ELBWIs), mechanical ventilation and total parenteral nutrition are generally required in the early stages and lose the protective effect of early gastrointestinal nutrition of colostrum. We conducted a prospective randomized controlled trial to explore the effectiveness of early colostrum oropharyngeal administration on the feeding status of ELBWIs on mechanical ventilation.
Materials and Methods:
We randomly divided mechanically ventilated ELBWIs into an intervention group and a control group. In the intervention group, we provided oropharyngeal administration of colostrum during mechanical ventilation. The first colostrum oropharyngeal administration ended within 24 hours of birth. In the control group, we gave colostrum only for gastrointestinal nutrition, and other interventions were the same as for the intervention group. We collected the 1st and 6th day of life airway secretions and urine specimens from both groups. We recorded feeding status, including corrected gestational age at onset of enteral nutrition, corrected gestational age of no gastric retention during feeding, corrected gestational age of full enteral nutrition, corrected gestational age of sucking began, and corrected gestational age of per oral feeding. We also recorded growth of body mass, the incidence of feeding intolerance, and necrotizing enterocolitis (NEC).
Results:
On the 6th day of life, concentrations of secretory immunoglobulin A, and lactoferrin in airway secretions and urine of the intervention group were significantly higher than those of the control group (p < 0.05). The intervention group showed younger corrected gestational age of no gastric retention during feeding, corrected gestational age of full enteral nutrition, the corrected gestational age of sucking began and per oral feeding than those in the control group (p < 0.05). The day of recovery to birth weight was earlier than those in the control group (p < 0.05). The rate of feeding intolerance and NEC incidence in the intervention group was significantly lower than in the control group (p < 0.05).
Conclusions:
Early oropharyngeal administration of colostrum improves immune function of the gastrointestinal tract and the systemic anti-infective capability in ELBWI on mechanical ventilation, promoting the maturity of gastrointestinal function, improving feeding condition, and reducing the risk of feeding intolerance and NEC.
Introduction
Extremely low-birth-weight infants (ELBWIs) are premature infants with birth weights of <1,000 g and gestational age generally <28 weeks. All organs tend to be extremely underdeveloped, especially the gastrointestinal and immune systems. ELBWIs generally require mechanical ventilation in the early stages of life, and they are susceptible to feeding intolerance and necrotizing enterocolitis (NEC). These phenomena not only affect the success rate of rescue ELBWIs, but they also lead to lifelong disabilities or death in severe cases. 1
Colostrum is critical for the treatment of ELBWIs. 2 Colostrum is rich in immune-active substances and nutrients that promote gastrointestinal maturation, interfere with bacterial proliferation, and promote immune response, thereby reducing the incidence of feeding intolerance and NEC and establishing full enteral nutrition as soon as possible. 3 Nevertheless, ELBWIs need mechanical ventilation and total parenteral nutrition in the early stages, during which they cannot tolerate enteral feeding and lose the protective effect of early gastrointestinal nutrition of colostrum.
We hypothesized that oropharyngeal microdosing of their mother's colostrum to ELBWIs on mechanical ventilation would improve immune function, promote gastrointestinal maturation, and prevent feeding-related adverse events. We tested our hypothesis by measuring concentrations of secretory immunoglobulin A (sIgA) and lactoferrin in airway secretions and urine, indicators of feeding status, and the incidence of feeding intolerance and NEC.
Materials and Methods
Design and sample
We conducted a prospective randomized controlled trial. The hospital ethics committee reviewed and approved the trial. We recruited participants among premature infants hospitalized in a 70-bed neonatal intensive care unit (NICU) and mothers hospitalized in a 180-bed obstetric ward of level III hospital in China. We collected data from July 1, 2017 to March 31, 2019. Inclusion criteria were as follows: (1) birth weight <1,000 g, gestational age <28 weeks, and appropriate for gestational age infants; (2) after birth, direct transfer to the neonatal department of our hospital; (3) invasive mechanical ventilation or noninvasive mechanical ventilation; (4) mother's intention to exclusively breastfeed, all milk from the ELBWs of own mother. Exclusion criteria were as follows: (1) congenital malformations, metabolic disease, congenital heart disease, or other difficulties with intestinal feeding; (2) no colostrum in mothers within 24 hours after birth. Withdrew criteria were as follows: (1) mother's colostrum is not available for five consecutive days; (2) no exclusive breastfeeding; (3) no further treatment (due to unsuccessful treatment, death, or family members request termination of treatment).
On the 1st day of admission of all premature infants, neonatal nurses went to the maternity ward and provided health education on breastfeeding for mothers and their families. This education included techniques for collecting, storing, and feeding. For mothers with difficulty obtaining postpartum colostrum secretion, the obstetrical lactation division intervened. A total of 141 ELBWs qualified for the study. According to inclusion and exclusion criteria, there were 130 subjects eligible for the study. According to the admission orders, we numerically encoded enrolled premature infants and randomized them into the intervention or control groups using the random number table method, with 65 patients per group (Fig. 1). The guardians provided informed written consent.

Randomization process. ELBWIs, extremely low-birth-weight infants.
Measurements
After admission, we obtained informed consent from the family. We collected the urine specimen and the first airway secretion specimen before administration pulmonary surfactant. We collected airway secretions and urine samples again on the 6th day of life. Airway secretion collection occurred with the infant having empty stomachs (i.e., before feeding). We froze all specimens immediately at −20°C. We measured concentrations of sIgA and lactoferrin in airway secretions and urine using an enzyme-linked immunosorbent assay. We purchased specimen detection reagents for lactoferrin and human secretory immunoglobulin kits from Shanghai Enzyme Biotechnology Limited Company. If the concentrations of sIgA and lactoferrin in airway secretions increased, we defined local immunity as improved. If the concentrations of sIgA and lactoferrin in urine increased, we defined systemic anti-infective ability as improved. 4
Comparison of feeding status indicators between groups included the following: corrected gestational age at onset of enteral nutrition, corrected gestational age of no gastric retention during feeding, and corrected gestational age of full enteral nutrition [total gastrointestinal nutrition was up to 140 mL/(kg·d)]. We also recorded the corrected gestational age when sucking began and the corrected gestational age of per oral feeding (defined as the first time the infant took >5 mL from a bottle). We recorded daily weights.
We recorded the incidence of feeding intolerance and NEC in both groups. The attending physician evaluated feeding intolerance and NEC's diagnostic criteria as per the fifth edition of Chinese Practical Neonatology. 5
Procedures
We sent the collected colostrum to the neonatal ward immediately and administered it as soon as possible. If not given immediately, we temporarily stored the colostrum in a medical refrigerator at 4°C for a maximum of 24 hours. If the amount of colostrum was large, we stored the excess at −18°C for up to 3 months. Scientific researchers carried out all procedures.
Both groups received normal saline daily oral care. If there were many oral secretions, we performed oral care after sputum aspiration. The intervention group received colostrum oropharyngeal microdosing after oral care with normal saline. During the study period, the control and intervention groups received the same enteral nutrition, parenteral nutrition, and the start of per oral feeding therapeutic schedule determined by the physician according to the clinical situation and the Chinese Practical Neonatology of premature infants standardized nutrition protocol. 6
Oropharyngeal administration of colostrum procedures was as follows: (1) We used disposable sterile 1-mL syringes (marked with 0.01 mL as a grid-scale) to extract a 0.2 mL colostrum leave it at room temperature for 5 minutes. (2) We placed the nipple end of the syringe into the infant's mouth (medial oral mucosa of the cheek) at the corner of one side of the mouth, with the head end pointing to the oropharynx, and instilled the colostrum at a uniform speed of 0.02 mL per infusion. We included a pause of 15–20 seconds for each injection to absorb colostrum by the oral mucosa. Dosing lasted for about 2 minutes. (3) We removed the sterile liquid dropper to the contralateral side and dripped the remaining 0.1 mL colostrum in the same manner. (4) A nurse performed the procedure, which we double-checked. We performed all operations in strict accordance with the sterile procedure, and the operator wore sterile gloves. (5) If there was vomiting, apnea, decreased oxygen saturation, bradycardia, or other adverse reactions, we immediately suspended the intervention and resumed it only after vital signs stabilized. (6) We provided colostrum oropharyngeal microdosing as early as possible. Our study started colostrum administration within 24 hours for all patients in the intervention group, once every 4 hours for 5 days, each time with a 0.2 mL colostrum. The frequency and duration of oral colostrum administration were the same as those of the Seigel study. 7
Data analysis
We performed statistical analyses using Stata version 11. We expressed normally distributed data as mean ± standard deviation and non-normal data as medians. We expressed count data as raw data and percentages. We compared the concentrations of sIgA or lactoferrin on the 1st and 6th day of life between the groups using repeated-measures analysis of variance and Student's t tests or chi-square test methods for the other data. We defined statistical significance as p < 0.05. The study was reviewed and approved by the Ethics Committee of the Second Affiliated Hospital & Yuying Children's Hospital of Wenzhou Medical University (NO. 67) and written informed consent from the patients was not required because this study did not directly intervene in the diagnosis and treatment of individual patients.
Results
A total of 14 patients in the intervention group and 12 in the control group withdrew. A total of 104 patients completed the study. The two groups of the treatment plan and enteral nutrition protocol remained consistent. There were no significant differences in gender, mode of delivery, gestational age at birth, age, or birth weight between the groups (Table 1).
Sample Characteristics
Values are means ± standard deviation or n (%).
There were no significant differences in the concentrations of sIgA or lactoferrin in the baseline airway secretions and urine in the intervention group and those of the control group (p > 0.05). There was a decrease in the concentration of sIgA and lactoferrin in the secretions and urine on the 6th day of life in the control group; however, the difference was not significant. On the 6th day of life, the concentrations of sIgA and lactoferrin in airway secretions and urine in the intervention group were significantly higher than those of the control group (p < 0.05; Figs. 2 and 3).
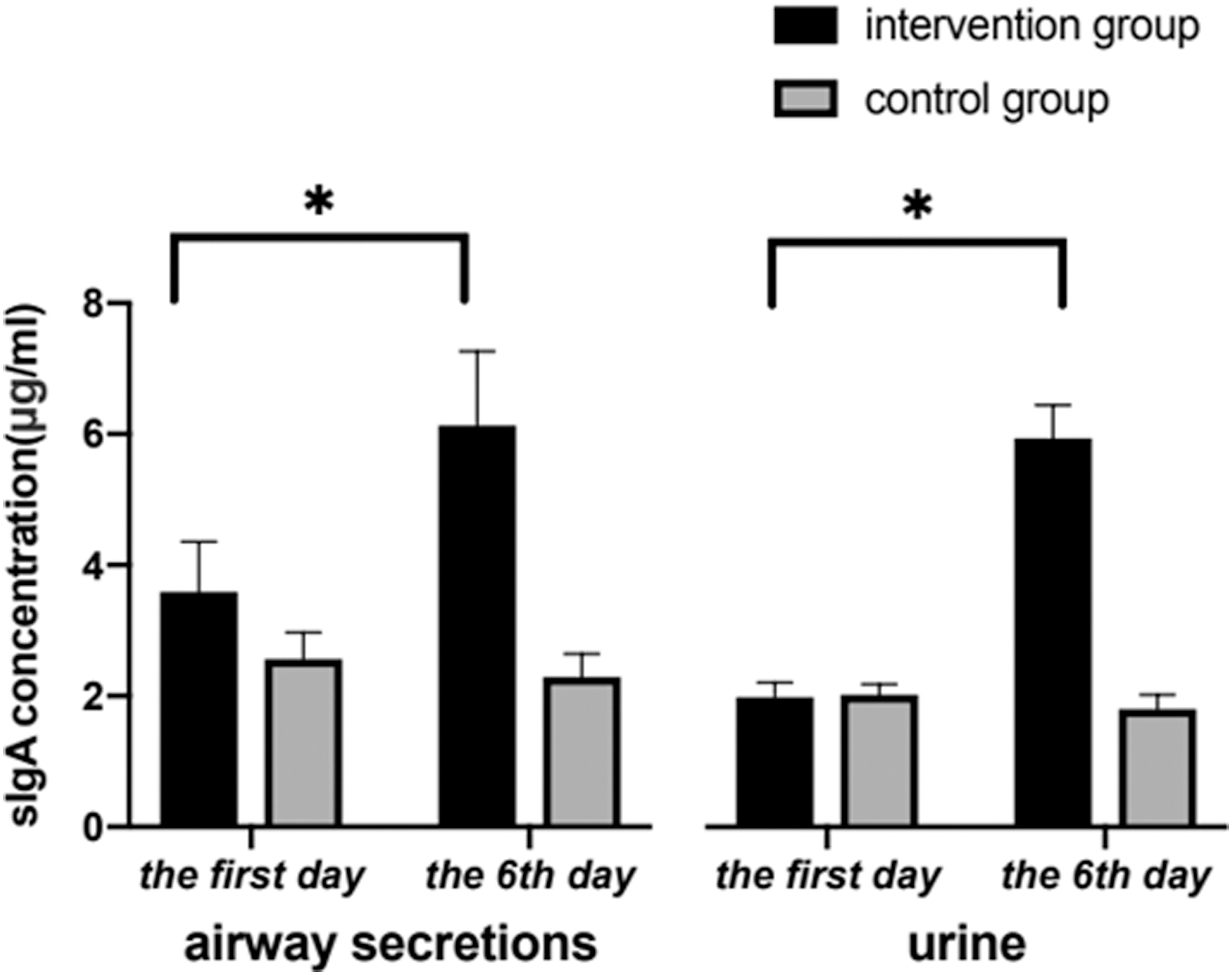
Comparison sIgA concentration of airway secretions and urine. *Represents p < 0.05 from statistical analysis. sIgA, secretory immunoglobulin A.
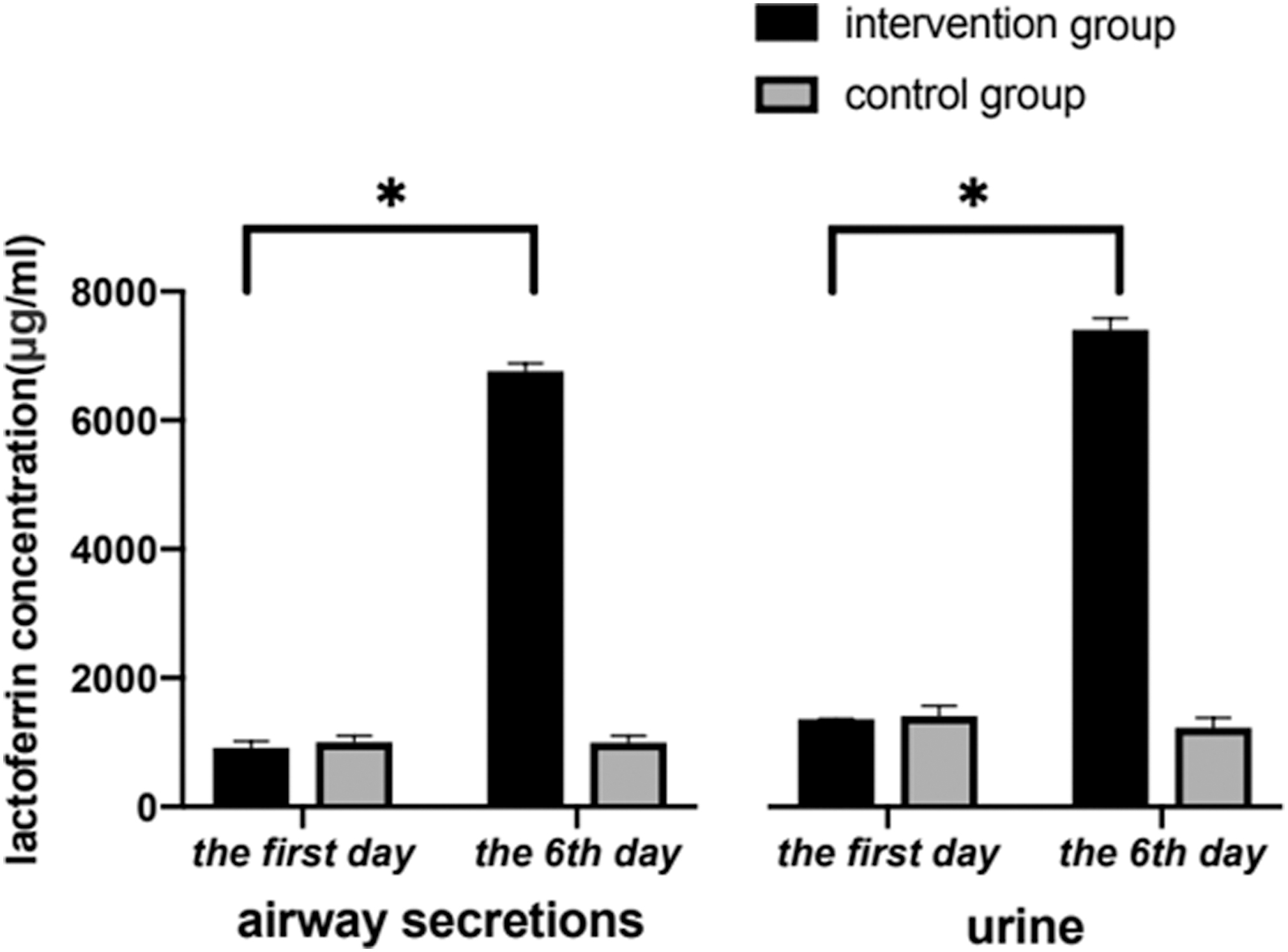
Comparison of lactoferrin concentration of airway secretions and urine. *Represents p < 0.05 from statistical analysis.
There were no significant differences in corrected gestational age at onset of enteral nutrition between the two groups (p > 0.05). After early colostrum oropharyngeal microdosing. The intervention group showed younger corrected gestational age of no gastric retention during feeding and corrected gestational age of full enteral nutrition than those in the control group (p < 0.05); the corrected gestational age of sucking began and per oral feeding were also younger than those in the control group (p < 0.05). The day of recovery to birth weight was earlier than those in the control group (p < 0.05; Table 2).
Comparison of Feeding Status Between the Two Groups
In the intervention group, the rate of feeding intolerance (29.41%) was significantly lower than that of the control group (54.72%; χ 2 = 4.034, p = 0.045). NEC incidence significantly decreased from 20.75% to 5.88% after oral colostrum administration (Table 3).
Comparison of Feeding-Related Adverse Events in the Two Groups
NEC, necrotizing enterocolitis.
Discussion
ELBWIs are extremely vulnerable to iatrogenic infections due to low local and systemic immune functions that cause NEC. 8 Colostrum is the most effective natural immune promoter for premature infants. 9 In our study, oropharyngeal administration of microdosed colostrum started within 24 hours of birth in ELBWIs on mechanical ventilation. We found that concentrations of sIgA and lactoferrin in the airway secretions and urine of the intervention group were significantly higher than those in the control group and were significantly different from those of the baseline airway secretions and urine of the intervention group. This finding suggests that early oropharyngeal administration of microdosed colostrum to ELBWIs can transmit immune substances and improved local and systemic immune functions. However, the difference in administration method, dose, and treatment times may account for the different results.10,11 In our study, we administered the colostrum for five consecutive days. Ideally, one should start the first colostrum oral administration within 24 hours of birth, as in the Seigel study. 7
Early oropharyngeal administration of microdosed colostrum promotes the oral feeding process of ELBWIs. Gastric retention as a primary index of feeding intolerance is a significant problem of ELBWIs. 12 We found that the corrected gestational age of no gastric retention during feeding and full enteral feeding were younger in the colostrum group than in the control group. This finding may occur because various cytokines in the colostrum during oral administration directly enter through the oropharyngeal mucosa, thereby promoting secretion of motilin and gastrin, and promoting intestinal movement and adhesion functions. 13 This process can prevent the retention of gastric contents and shorten the time to reach full enteral feeding. Generally, the regulation of sucking, swallowing, and breathing in premature infants does not mature until 34 weeks of gestational age. 14 Simpson et al. found that preterm infants younger than 30 weeks of gestational age achieved safe and effective early oral feeding ability by taking effective intervention measures before gestational age at 33 weeks. 15 Our results suggest that early colostrum administration improves sucking, swallowing, breathing, and co-ordination, promoting digestive system maturation. So as early as possible to achieve per oral feeding and recovery to birth weight.
Their immature development of the gastrointestinal system, coupled with poor immune defense and intestinal barrier function feeding intolerance and NEC, often occurs in ELBWIs. The incidence of NEC ranges from 20% to 40%. 16 Studies showed that slgA antibody, intestinal trophic factors, oligosaccharides, lactoferrin, and other protective cytokines contained in colostrum absorb into the intestine through the oral mucosa, maintaining the stability of the intestinal environment and improving the immune function of the gastrointestinal tract, thereby preventing feeding intolerance and NEC. 17 In our study, the incidence of feeding intolerance and NEC in the intervention group was significantly lower than that of the control group; the incidence of NEC decreased from 20.75% to 5.88%. This finding suggests that colostrum administration reduces the adverse events associated with feeding in the early stages of life for ELBWIs, consistent with the findings of Rodriguez and Caplan. 18 However, many factors combine to make ELBWIs a high-risk group for feeding intolerance and NEC. Advanced neonatal medical technology level, improved medical environments, and improved breastfeeding compliance among family members are also important factors contributing to the decrease of feeding intolerance and NEC incidence in ELBWIs in recent years. Large clinical samples and multicenter further research are required to determine the extent to which early oropharyngeal administration of microdosed colostrum affects feeding intolerance and NEC.
Conclusions
Colostrum promotes the maturation of gastrointestinal function in ELBWIs, improving their feeding status, and reducing the risk of feeding intolerance and NEC.
Footnotes
Authors' Contributions
All authors contributed to the conceptualization and development of the study and interpretation of data. They all reviewed and edited the article and approved the final draft.
Disclosure Statement
The authors declare that they have no conflict of interests for this work.
Funding Information
This research derives from the Medical Health Science and Technology Project of Zhejiang Provincial Health Commission in China (Item Number: 2018KY528).