
Abstract
Background:
Postpartum depression (PPD) is one of the most common birthing complications, and studies negatively associate PPD with breastfeeding initiation and continuation. However, little is known about either the breastfeeding experience of mothers with PPD or what resources mothers need for sustained breastfeeding from their perspectives. This study aimed to identify the antecedents, barriers, and facilitators to breastfeeding for mothers with PPD, understand the relationship between self-efficacy and emergent themes, and generate suggestions to inform supportive interventions.
Materials and Methods:
Birth mothers who screened positive for PPD and reported breastfeeding were recruited to participate in semistructured interviews. Interviews were transcribed verbatim, and inter-coder discrepancies from double coding were resolved through consensus. Thematic analysis was facilitated using immersion-crystallization methods.
Results:
Participants identified five antecedent themes that encourage initiation (professional support, infant health, mother's health, cost-effectiveness, and faith), four facilitator themes for sustained breastfeeding (infant connection, decreased stress, personal attributes, and logistical strategies), and seven barrier themes (physical pain, infant nutrition, negative feelings, latching difficulties, medical conditions, public breastfeeding, and sleep). Participants' suggestions fell into three primary themes: supportive services, managing expectations, and respecting self-determination.
Conclusion:
Antecedent and facilitator themes did not overlap, indicating that factors encouraging breastfeeding initiation differ from sustaining factors. Participant suggestions, barriers, and facilitators did not largely differ from mothers without PPD in other qualitative studies. Therefore, interventions should tailor support to specific breastfeeding phase and may not need to be markedly different for mothers with PPD, in addition to depression management.
Introduction
The positive benefits of breastfeeding on infant health are numerous, including protection from disease and infection; reduced risk of sudden unexpected infant death syndrome and childhood obesity; and physical, mental, and cognitive developmental advantages.1–3 As a result of supportive policies and interventions to promote breastfeeding, the rate of immediate postpartum breastfeeding in the United States has steadily grown over the last 25 years from 52% in 1990 to 83% in 2015.4,5 Despite progress, women who give birth continue to experience a variety of obstacles to breastfeeding, such as lack of parental education about feeding, inadequate social support, barriers to breastfeeding at the workplace, and physical lactation difficulties, all of which affect both immediate initiation as well as continued breastfeeding efforts.6,7
One of the primary, although poorly recognized, barriers to sustained breastfeeding is postpartum depression (PPD). Approximately 13% of postpartum mothers experience PPD in the United States, and this rate could be as high as 25% in some populations, such as women who have immigrated to the United States or who are American Indian.8–12 Women with histories of depression or partner violence also have been found to have higher rates of PPD at rates estimated to be at 29% and 33%, respectively. 12 PPD therefore constitutes one of the most frequent birthing complications. 13
Numerous studies have identified the correlation between not breastfeeding or breastfeeding cessation and PPD.14–17 In addition to psychosocial factors, biological mechanisms influence this relationship, primarily through the release of oxytocin during breastfeeding, which can help prevent and combat depressive symptoms. 18 Whether PPD contributes to breastfeeding cessation, whether breastfeeding cessation triggers PPD, PPD is partially dependent on length of time and “dose” of exclusive breastfeeding, or there is a bidirectional or time-varying relationship between the two factors continue to be debated.16,19–23 Regardless of the unclear direction of the relationship between breastfeeding and PPD, the need to provide breastfeeding support to women who have or who are at risk for PPD is evident. 16 Supportive interventions must also be aligned with the needs and priorities of these women. A qualitative approach can offer vital insight into the perspectives of individuals regarding a health phenomenon and can be instrumental in translating scientific findings into effective, person-centered services.24–27
A number of recent studies have employed qualitative methods ranging from in-depth interviews to focus groups to online diary entries to better understand the breastfeeding experience of women.28–33 Through these studies, women's needs for a continuum of emotional, instrumental, and informational support can be heard, especially when faced with social pressure, limited resources, and the emotional demands that complicate breastfeeding.28–33 Qualitative studies such as these lay the foundation for addressing the needs of mothers, but they have not specifically investigated the needs of mothers who experience PPD. In fact, very little qualitative research has been done with women experiencing PPD, and almost none has been done with a focus on breastfeeding, although PPD has at times surfaced as a theme in such qualitative studies. 34
Self-efficacy theory (SET) is often used to explore health behaviors, such as breastfeeding, and can provide a helpful framework through which to understand the most relevant factors that lead to a behavior.35,36 SET, a component of Social Cognitive Theory developed by Albert Bandura, suggests that a person's belief in their own ability to carry out a task or action (i.e., self-efficacy) comprises three constructs: (1) expectations of the behavior (includes prior performance accomplishments; vicarious experiences of the behavior; verbal persuasion from others; and the physiological and affective state of individual); (2) influence of the individual's self-efficacy on the behavior (includes effort expenditure and persistence; thought patterns and schemas; and emotional reactions to the behavior); and (3) behavioral expectations related to the eventual outcome of the behavior.35,37 Using this theoretical framework and a qualitative approach, this study aims to better understand the experience of breastfeeding of mothers with PPD; identify the relationship between self-efficacy and emergent themes using SET constructs; and learn what supports mothers with PPD need for sustained breastfeeding from their perspectives.
Methods and Materials
Study participants
Participants were referred to the research team from a pilot randomized controlled trial (RCT) investigating the use of social media as a parenting intervention for birth mothers with PPD symptoms living in a large Mid-Atlantic city. 38 Birth mothers were eligible to participate in this qualitative study if they were at least 18 years of age, reported initiating breastfeeding at least once with their infant, and had screened positive for PPD symptoms at the 2-month well-child visit. The Edinburgh Postnatal Depression Scale (EPDS) was used to screen women for PPD. EPDS has demonstrated strong validity and reliability for measuring perinatal depression, and is frequently used as a screening tool for PPD.39,40
Study design
This study consisted of one-time, semistructured interviews. The interview guide was developed with input from experts in PPD, breastfeeding, and qualitative methods. The interview guide was organized around three primary domains: (1) expectations of breastfeeding; (2) contributors and challenges to initiation and sustained breastfeeding; and (3) mood since birth of child. This study was approved by the institutional review boards of University of Pennsylvania and Children's Hospital of Philadelphia.
Data collection
Interviews were conducted by a trained qualitative interviewer with familiarity with the health care system and neighborhood from which participants were recruited. Interviews were conducted in private administrative health care offices to ensure privacy and were conducted at a time that was convenient for participants. Participants were accompanied by their infants and occasionally other children younger than 3 years. Interviews ranged from 30 to 50 minutes in length, and all interviews were audio-recorded, transcribed verbatim, and checked for accuracy against the original recording. Participants were recruited and interviewed until inductive thematic saturation was reached (that is later interviews did not generate new themes). 41
Data analysis and theoretical framework
Transcripts of interviews were entered into NVivo 10 (QSR International Pty Ltd.), a software that facilitates qualitative analysis. Members of the research team independently coded the first three transcripts, utilizing open-coding strategies. 42 The research team then employed a directed content analysis approach and generated a codebook comprising a priori codes based on the constructs of SET35,37 and codes generated from the open coding process. 43 Each transcript was coded independently by two members of the research team and inter-coder reliability (ICR) was assessed to identify coding inconsistencies. ICR was calculated in NVivo by using the Kappa statistic. When Kappa was less than 0.5 for any code within a transcript, the team met to resolve coding discrepancies. The final mean kappa across all codes was 0.93 (range: 0.53–1.0), demonstrating near perfect coding agreement. 44 The research team then organized codes to identify themes and subthemes using an immersion-crystallization approach. 45 While the thematic analysis methods were primarily inductive, the final step in the analysis was to deductively compare the study's themes to the constructs of SET, such as prior performance accomplishments; vicarious experiences of the behavior; verbal persuasion from others; physiological and affective state of individual; effort expenditure and persistence; thought patterns and schemas; emotional reactions to the behavior; and behavioral expectations related to the outcome of the behavior.35,37 SET constructs were used to categorize emergent themes to identify the elements of self-efficacy that had the greatest influence on participants.
Results
Participant characteristics
Of the 43 women who had given birth, screened positive for PPD, and were recruited for the RCT, 34 reported breastfeeding and met the criteria to participate in a semistructured interview about breastfeeding. Of these women, 17 women agreed to be interviewed, and 12 women ultimately completed interviews about their breastfeeding experience (Fig. 1). Participants ranged in age from 18 to 39 with a mean age of 28 and had on average 2 children. Eight participants identified as Black/African American, one participant identified as Hispanic/Latina, and three participants reported more than one race. All participants identified as female (Table 1).
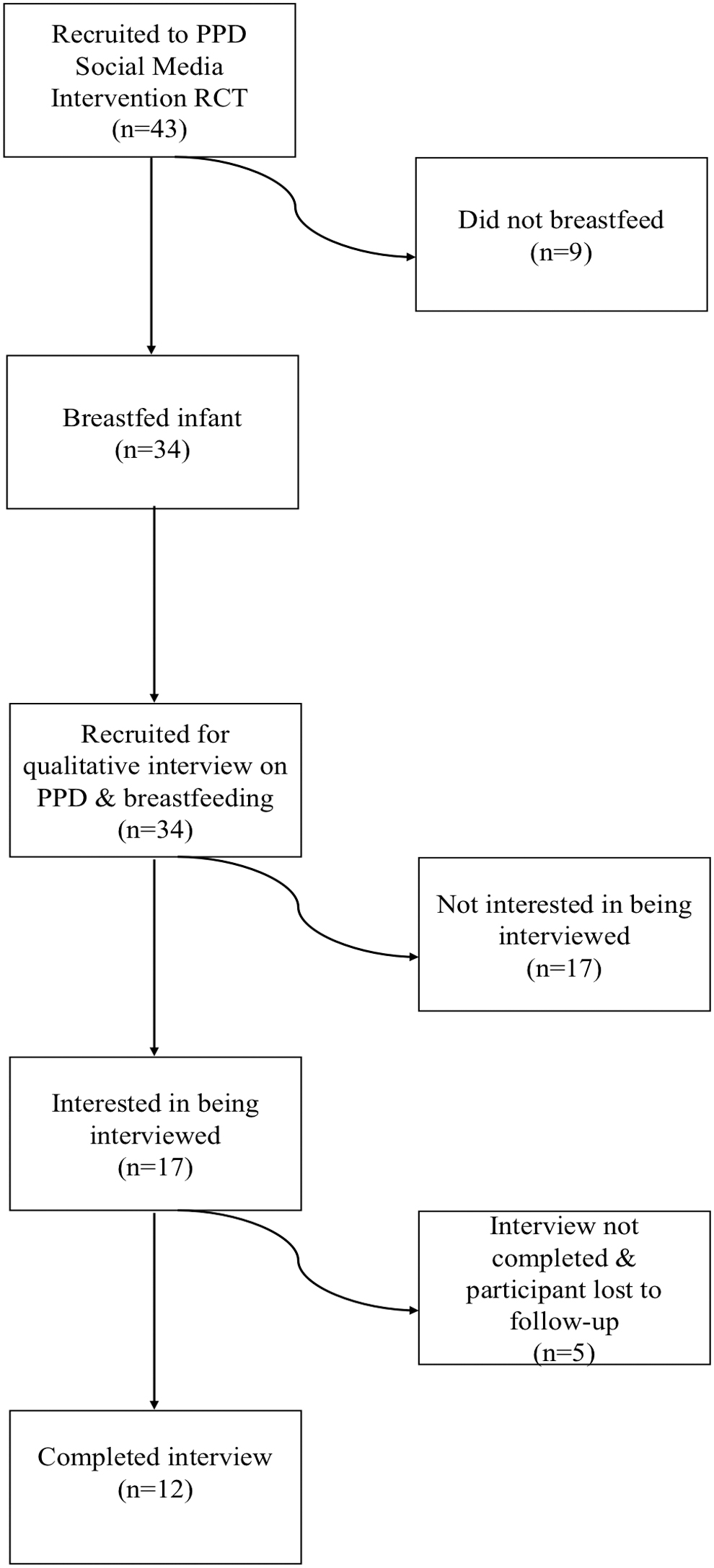
Recruitment method.
Participant Characteristics
Thematic overview
Primary themes of what contributed to breastfeeding initiation (antecedents), what supported sustained breastfeeding (facilitators), and what prevented sustained breastfeeding (barriers) emerged through analysis of the transcripts. Further analysis identified subthemes within antecedents to breastfeeding, which did not overlap with breastfeeding facilitators. All themes, subthemes, mapping to SET constructs, and illustrative quotes can be found in Tables 2 and 3.
Antecedents to Breastfeeding
Facilitators and Barriers to Breastfeeding
Antecedents to breastfeeding
Many of the women began their interviews by describing the factors that had contributed to their first efforts to breastfeed their newborn. These antecedents fell into five primary themes: support from health professionals, health of the infant, health of the mother, cost-effectiveness, and faith background (Table 2). Of these five themes, how the health of the infant could be improved through breastfeeding was often described more thoroughly by participants. One participant described her abstract comfort with breast milk as “natural” and safe for infants, sharing “Now you're able to give that baby continued life from natural food… hasn't been altered in any way whatsoever. And it's a protection for that baby…” Another participant noted how her older children who had been breastfed appeared healthier than her formula-fed children, stating, “Most of my kids who I have had the experience of breastfeeding for a while weren't sickly kids… I didn't have a lot of doctor visits with my children.” Support from health professionals also emerged frequently as an antecedent. Participants described how informational support, such as hospital classes, pamphlets, or talking with a medical provider as well as physical assistance with latching, encouraged breastfeeding initiation. One participant described how a nurse “gave me basically a step-by-step because I had never [breastfed] before,” and she attributed this physical assistance to successful initiation. When the antecedent themes were categorized according to SET elements, all the themes fell into one of two elements: verbal persuasions or outcome expectations.
Facilitators and barriers to breastfeeding
Participants described a variety of aspects of their lives, breastfeeding experience, and personal and emotional characteristics that they identified as contributing to continued breastfeeding. These facilitators fell into five primary themes: feeling connected to the infant; decrease in stress and unhappy feelings; particular personal attributes, such as perseverance; and specific strategies that made breastfeeding easier (Table 3). At times these facilitators overlapped, as when one participant shared how both her connection with her baby and stress mitigation could be achieved through breastfeeding, saying, “When I'm nursing her, I'm able to just hold her. And that just alleviates any worries, any stress that I've had through the day, just knowing that she needs me, that she's finding comfort in me, that I'm able to comfort her. She's comforting me at the same time.” Facilitator themes corresponded to a variety of SET elements, including emotional reaction, thought patterns, effort expenditure and persistence, and verbal persuasion.
Descriptions of breastfeeding facilitators were often closely followed by descriptions of barriers and these often outweighed the facilitators, contributing to breastfeeding cessation among many participants. References to barriers fell into eight primary themes: physical pain; concerns about infant getting enough milk; feelings of overwhelm, frustration, and anxiety with breastfeeding difficulties; competing demands and time constraints with more than one child; medical conditions that made breastfeeding difficult or unhealthy for the infant; discomfort or restrictions with public breastfeeding; infant's difficulty latching; and having to sacrifice sleep to breastfeed (Table 3). These themes coincided with three SET elements: effort expenditure and persistence, emotional reactions, and thought patterns, the majority of which were categorized at effort expenditure and persistence.
While participants rarely directly referenced feelings or symptoms of depression in the interviews, maternal overwhelm, frustration, and stress emerged in both descriptions of facilitators and in barriers. One participant shared that she avoided thinking about producing enough milk even though she was trying to breastfeed her infant, because she feared this would generate feelings of depression:
Struggling not to go into the postpartum depression part because of the milk thing. I think that's the only thing that would have triggered me in that area with just not being able to completely concentrate on her in giving the milk that she needs. So that's what it is, struggling for me emotionally, that I just try to stay clear from that area because I do get emotional over it knowing that I don't have a choice in a lot of the things.
Another participant shared how she felt anxious as she prepared to go back to work: “I remember when my first breakdown moment was. As I got closer to going back to work, and I wanted her to nurse more so that I can build up my supply, and she wasn't doing it as much as I wanted her to do. I'm trying to build up my supply and just having that separation anxiety.”
Participant suggestions
All participants stated that they would encourage every mother to try to breastfeed. However, participants also recognized that breastfeeding may not work for every mother and child, as one participant suggested, “Do it once … everything isn't for everybody … they always have to do what works for them.”
Many of the participants listed strategies and resource tips, such as the availability of a free pump through Supplement Nutrition Program for Women, Infants, and Children (WIC), considering have a small store of breast milk available in the refrigerator, and experimenting with different bottles to find the right fit for the infant if the mother chooses to pump. In addition to tangible suggestions, many of the participants focused on the need to help mothers manage expectations around breastfeeding and help them find information and emotional support to encourage their own decision making and self-determination. Participants noted the importance of preparing mothers for the possibility of physical discomfort and effort that may accompany breastfeeding and to encourage them to reach out for assistance if they experience any emotional or physical discomfort, stress, or strain. One participant emphasized the importance of coming to one's own conclusion about breastfeeding, stating, “Don't just listen to all of the good things. And don't just listen to all of the bad things … Do your own research as well and find out.”
Discussion
To improve support for mothers who want to breastfeed and who experience PPD, it is critical to better understand breastfeeding experiences from their perspectives. Qualitative interviews proved particularly effective in this study to elucidate and differentiate the factors that contributed to participants' decisions to initiate breastfeeding, encouraged them to continue, and impeded sustained breastfeeding.
It can be tempting to conflate factors that may encourage a mother to initiate breastfeeding with the facilitators of sustained, multi-month breastfeeding. As can be seen from the antecedent and facilitator themes in this study, these factors were different and did not overlap for mothers. In fact, many of the antecedent themes focused on receiving information or external factors such as the health of the infant or cost-effectiveness of breast milk, whereas facilitator themes often centered on internal processes for mothers, such as feeling connected to the infant and alleviating stress. Familiarization with the factors that support mothers to initiate breastfeeding and how they may differ from factors that encourage mothers to continue to breastfeed despite obstacles may help practitioners tailor their approach to supporting mothers who choose to breastfeed.
Many of the participants in this study reported having stopped breastfeeding, and this appears to correspond to the observation that participants identified many more barriers to breastfeeding than facilitators. While some of these barriers were, like the facilitators, related to the internal processes of mothers, such as personal concerns about the infant getting enough nutrition and feelings of overwhelm, many more of the barriers were rooted in factors outside the mother's control, such as competing demands with multiple children and maternal medical conditions. It may be impossible to fully eliminate all barriers for mothers, but by helping mothers identify personal facilitators to breastfeeding, practitioners may be able to help mothers “tip the balance” toward continued breastfeeding.
While participants' self-efficacy was woven throughout their experience, SET constructs appear to vary according to the antecedent, barrier, or facilitator theme (Fig. 2). When participants first initiated breastfeeding, their self-efficacy seems to have been heavily influenced by verbal persuasion, primarily by health professionals, as well as outcome expectations related to maternal-child health and opportunities to save money. Later, the elements of self-efficacy that surfaced were more diverse, and included emotional reaction, thought patterns, effort expenditure and persistence, and verbal persuasion. Thus, the elements that facilitate a mother's positive breastfeeding self-efficacy once she has already initiated breastfeeding are much more varied, and the experience may be more individualized. In contrast, the majority of barriers that the mothers described coincided with the element of effort expenditure and persistence. Many of these barriers were outside the mother's control, and therefore required increased persistence and effort. As a note of caution, while breastfeeding frequently requires substantial persistence, focusing too much on this without recognizing the systematic and institutional barriers to sustain breastfeeding could potentially have a “victim blaming” effect, since it could internalize feelings of deficiency.
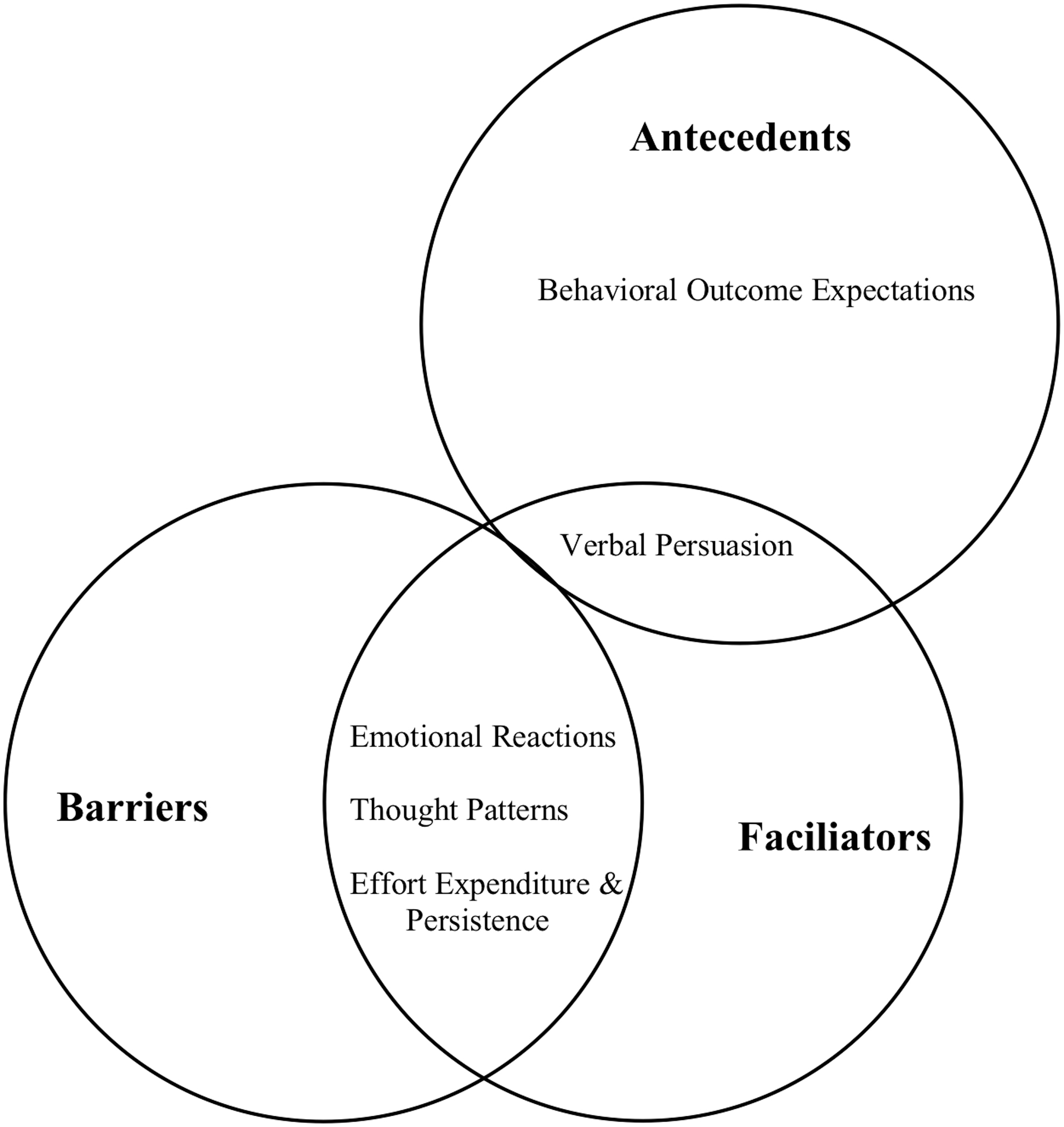
Self-efficacy theory elements according to thematic category.
While the mothers in this study reported PPD symptoms as part of participation criteria, few of these participants identified these symptoms as influencing their breastfeeding experience during interviews. Several of the participants noted feeling frustrated, overwhelmed, or stressed, which could be related to depression. One participant specifically noted that she avoided thinking about breastfeeding for fear this might “trigger” depression symptoms. While the stigma surrounding mental health challenges could lead participants to avoid the topic, that depression rarely emerged as a distinct topic in the interviews is notable. While the association between PPD and breastfeeding has been found in many studies,15–17,19,20 mothers with PPD in this study do not primarily identify these symptoms as central to their breastfeeding experience. In fact, when comparing the facilitator and barrier themes of mothers with PPD symptoms in this study with those of breastfeeding mothers without PPD in other qualitative studies, the themes do not appear to substantially differ.28–33 Thus, supporting mothers with PPD to breastfeed may require a similar approach to mothers without PPD and may not require different supportive breastfeeding interventions, in addition to depression management.
This conclusion is substantiated by a closer look at the suggestions that participants in this study provided to other mothers. Many of the suggestions focused on encouraging mothers to seek out the materials and resources that help with breastfeeding, such as breast pumps, experimenting with bottles, and accessing services through WIC. Other participants offered advice about managing expectations about the ease and pain associated with breastfeeding and emphasizing a mother's self-determination to decide whether or not breastfeeding was the right decision for her. These participant-initiated suggestions closely match the needs discussed by participants in other qualitative breastfeeding studies.28,29,32 That said, further research directly comparing the breastfeeding needs of mothers with PPD symptoms and those without is necessary to confirm this observation.
Strengths and limitations
It is important to note several strengths and limitations of this study. Of the 34 participants of the parent RCT who were eligible to participate in this qualitative study, only about a third completed an interview. It is therefore possible that participants who were interviewed differed from other mothers who experience PPD symptoms. To date, most PPD and/or breastfeeding research participants identify as White women, and participants in this study identified as either non-White or of multiple racial identities.17,27,46 The social environment—including experiences of discrimination, resource access, and cultural norms—substantially informs breastfeeding and depression experiences. Therefore, this study additionally contributes to the breastfeeding literature by giving voice to the experience of mothers who are often not included in breastfeeding and PPD research.
It should be noted that during the interview, participants' infants and very young children were sometimes present. While these children were too young to understand the conversation, their presence may have influenced their mothers' responses or mildly distracted them during the interview. Since this was a homogeneous sample and the interview guide had a narrow focus, we reached inductive thematic saturation for the majority of the themes highlighted here. 41 However, had the research team been able to recruit additional participants from the parent RCT, further purposeful exploration of some of the subthemes may have elicited even greater nuance and understanding of the breastfeeding experience of mothers with PPD.
Conclusion
Mothers who experience PPD symptoms are known to struggle with breastfeeding, and without hearing directly from these individuals, it is impossible to determine the best methods to support sustained breastfeeding. According to the mothers in this study, the factors that encourage breastfeeding initiation and the factors that encouraged sustained breastfeeding are different, yet closely match the participant-identified factors of breastfeeding mothers without PPD from previous qualitative studies. While mothers with and without PPD may not require markedly different interventions to encourage sustained breastfeeding, a general need for supportive services is apparent.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported, in part, by grants from the Maternal Child Health Bureau (R40MC11267), American Academy of Pediatrics CATCH award, and National Cancer Institute of the National Institutes of Health (R25CA057711 and 2T32CA057711-26). The funding organizations had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the article; or decision to submit the article for publication.