
Abstract
Objective:
To examine the associations between human milk feeding method (at the breast versus bottle) and measures of child adiposity during the first 6 years of life.
Study Design:
Women 12 months' postpartum who delivered a singleton, liveborn infant at >24 weeks gestation completed a survey assessing infant feeding methods and sociodemographics. Mothers were recontacted when the child was 6 years old for a follow-up study assessing growth (N = 269). Children were categorized as ever or never having excess weight using weight-for-age z-scores (WAZ), weight-for-height z-scores (WHZ), and body mass index-for-age z-scores (BMIZ) from birth to 6 years. Modified Poisson regression estimated associations between the duration of each feeding method (exclusive and combined) with excess weight status. Mixed-effect models estimated associations between feeding methods and trajectories of the outcomes.
Results:
For all feeding practices, increasing duration (in months) was unassociated with the risk of ever having excess weight by age 6 years. Based on mixed models, longer duration of feeding human milk by any method was associated with lower BMIZ (adj β for 6–12 months versus 0–3 months = −0.50, 95% CI: −0.99 to −0.01) and also with the shape of the BMIZ trajectory curve. No other associations between feeding methods and excess weight outcomes were observed.
Conclusions:
Longer duration of feeding human milk was associated with lower average BMIZ in early childhood but feeding at the breast and feeding expressed milk were not clearly associated with the outcomes when considered separately. Larger studies would help clarify the associations between these specific feeding methods and outcomes. IRB17-00876.
Introduction
Numerous studies have reported that prolonged, exclusive breastfeeding (usually assumed to be feeding at the breast) is associated with slower growth during infancy and, therefore, lower long-term obesity risk.1,2 For example, as reported by the World Health Organization (WHO) European Childhood Obesity Surveillance Initiative, the odds of becoming obese were lower in children who were exclusively breastfed as compared with those who were never breastfed or only breastfed for a short period of time. 3 Likewise, data from a meta-analysis conducted by Victora et al. suggested that breastfeeding may have a protective effect against children becoming overweight later in life. 4 In contrast, the results of the Promotion of Breastfeeding Intervention Trial (PROBIT) trial, conducted by Kramer et al., found that assignment to a prolonged, exclusive breastfeeding intervention resulted in faster growth during infants' first several months of life. 5 Martin et al. extended these original findings by highlighting that longer duration and exclusivity of breastfeeding during infancy led to an increased prevalence of overweight/obesity by adolescence. 6
This prior evidence is heterogeneous and may not generalize to today's U.S. infants because the means by which they are fed has evolved. For infants fed human milk, feeding at the breast is gradually being replaced with pumping human milk and feeding it by bottle. 7 Although nationally representative data are scarce, the percentage of infants fed some amount of expressed (pumped) milk was 38% in an Australian study from the early 1990s versus 69–85% in the U.S. Infant Feeding Practices Study II (IFPS II) in the mid-2000s.8,9
Regardless of the substance (human milk or formula), bottle feeding has been associated with increased weight gain during infancy based on data from the IFPS II.10,11 Although the exact mechanisms are not entirely known, one possibility is that infants more passively participate in the bottle-feeding process compared with feeding at the breast, and infants may be urged to empty their bottles even when they are no longer hungry. This may override their internal signals to control their intake, with the potential for long-term disruption of satiety mechanisms and a resulting proneness to excess weight, as compared with infants who are fed at the breast.11,12 Whether feeding method has an independent effect on long-term adiposity remains unknown, but the IFPS II 6-year follow-up study reported that maternal encouragement of bottle emptying during infancy increased the probability of mothers pressuring their 6-year-old children to eat all their food at meals. 11
This study sought to address this gap in knowledge by examining the associations between different human milk feeding methods (at the breast versus bottle) and measures of child adiposity during the first 6 years of life.
Materials and Methods
Study population and data collection
The Moms2Moms (M2M) study included English-speaking women, who were at least 18 years of age and delivered a singleton, liveborn infant at >24 weeks' gestation at The Ohio State University Wexner Medical Center (Columbus, OH) in 2011. A total of 1244 mothers were potentially eligible. Women whose obstetric record indicated that they intended to exclusively “bottle” feed their infant (in this clinical unit at the time, this meant formula feed) (n = 303), had no valid contact information (n = 111), whose infants had died since hospital discharge (n = 6), or were incarcerated (n = 11) were excluded. Eligible women (n = 813) were mailed a questionnaire to gather sociodemographic information and assess maternal lactation and infant feeding practices at 12 months postpartum, and 497 participated. Obstetric and newborn medical records were abstracted. Further details about the M2M study methods have been previously reported.13,14
When the children were 6 years old, women were recontacted to invite participation in this follow-up study.
Data collection instruments included a sociodemographic questionnaire and a pediatric medical record release form to gather length/height and weight data collected during clinical care. If a child had more than one primary care physician, a second authorization was obtained. Follow-up participants whose child had at least one weight or height measurement were included in this analysis. Participants received a $10 incentive. This study was reviewed and approved by the Institutional Review Boards at The Ohio State University and Nationwide Children's Hospital. A waiver of documentation of consent was requested, and all components of consent were included in the introduction of the administered surveys. For both the original and follow-up studies, individuals were informed that participation was voluntary and that declining participation would not result in penalty or loss of benefits.
Study variables
Maternal and child characteristics
Information regarding maternal age at delivery, maternal parity (primiparous versus multiparous), child's sex (male, female), whether the child was delivered through cesarean section (yes, no), birth maturity (preterm birth [25–37 weeks] versus term birth), and birth weight (kg) were abstracted from the obstetric and newborn medical records. The following sociodemographic characteristics were gathered from the questionnaire administered at 12 months' postpartum—maternal race (White/Caucasian, Black/African American, other), maternal ethnicity (Hispanic, non-Hispanic), maternal education (high school/general educational development or less, some college/Associate's degree or less, bachelor's degree, postgraduate degree), marital status (married/living with partner, unmarried/not living with partner), smoking during pregnancy (yes, no), women, infants, and children (WIC) enrollment in pregnancy or infancy (yes, no), public or no health insurance (yes, no), perceived financial difficulty in pregnancy (great difficulty making ends meet, difficulty making ends meet, we just get by, easily able to make ends meet, very easily able to make ends meet), and age at which the child started daycare (never, started daycare early [age 1–90 days], started daycare later [day 91+ days]).
Infant feeding variables
At 12 months' postpartum, participants were asked for the age of their infant when they started and stopped feeding at the breast, feeding expressed milk, and feeding formula using the questions given in Supplementary Table S1. Using this information, three duration variables (in units of days) were created for human milk feeding (feeding at the breast and expressed milk feeding combined), feeding at the breast, and expressed milk feeding, by subtracting the infant's age when each behavior was started from the age when it stopped, including the first day of the behavior, and converting the units as needed. Infants who were still engaged in that specific feeding method at 12 months of age were assigned a stopping point of 365 days. Variables for the duration of exclusive human milk feeding and exclusive feeding at the breast were created using a two-step process. Using the infant's start and stop age, dummy variables for each feeding method were created for each day of the year (day 1–day 365). Infants received a “1” if they engaged in that particular feeding method that day and “0” if they did not engage in that feeding method that day. The number of days an infant exclusively engaged in that feeding method (when that feeding method equaled one and the dummy variables for other feeding methods equaled zero) were summed to create exclusive feeding duration variables. Categorical duration variables of 0–3, 3–6, and 6–12 months were created for human milk feeding, exclusive human milk feeding, feeding at the breast, exclusive feeding at the breast, and formula feeding. Exclusive expressed milk feeding was typically practiced for short periods of time by a small subsample of dyads and so was not studied further.
Anthropometrics
Trained research staff abstracted all weight and height (length for measurements taken at <24 months) measurements from medical records from birth to age 6 years. The child's age at the time of each measurement, weight and length/height were used to calculate weight-for-age z-scores (WAZ), weight-for-height z-scores (WHZ), and body mass index-for-age z-scores (BMIZ), using the WHO Child Growth Standards by implementing a WHO growth macro for SAS. 15 For children born preterm, z-scores were calculated using their age adjusted for prematurity for measurements taken before 24 months of age. WAZ, WHZ, and BMIZ were dichotomized to indicate if the child ever had an excess WAZ, WHZ, or BMIZ measurement (if any of the child's z-scores for that outcome were >1 SD above the mean; this cutoff was selected to be more sensitive as an early indicator of potential future overweight or obesity than 2 standard deviation (SD) that is often used in research given that adiposity can change rapidly in early childhood) or never had an excess weight measurement (all the child's z-scores for that outcome were ≤1 SD above the mean).
Statistical analysis
Univariate statistics were applied to describe the sample. Modified Poisson regression was used to estimate associations between infant feeding durations (in units of months) and each binary excess weight variable and to address the overestimation of relative risk (RR) that comes with using logistic regression models for binary outcome data. 16 Models were adjusted for potential confounders that were hypothesized to have relationships to both infant feeding practices and early childhood growth based on prior literature (maternal age at delivery, maternal race, maternal ethnicity, maternal education, marital status, parity, smoking during pregnancy, WIC enrollment in pregnancy or infancy, public or no health insurance, perceived financial difficulty, child sex, cesarean section delivery, birth maturity, age started daycare, and birth weight).
To examine associations between infant feeding durations (categorized as 3–6 and 6–12 months versus 0–3 months) and early childhood growth, longitudinal trajectories of WAZ, WHZ, and BMIZ from birth to age 6 years were constructed using quadratic mixed-effects models. This approach was able to estimate both individual and group growth trajectories while simultaneously examining the feeding methods predictors of interest that may influence those growth patterns. 17 Furthermore, it permitted the modeling of nonlinear growth trajectories and accommodated unbalanced longitudinal data (unequal numbers of growth measurements among children) measured at varying ages. This approach also used maximum likelihood estimation to include children with missing growth measurements at various time points.
Separate models were constructed for each feeding method. Child age (in completed years) and a quadratic term for age at the time of measurement, and duration of the particular feeding method (categorical) were included in the models. The duration variable was included in the mixed model as a fixed effect to explore if growth trajectories differed across feeding duration groups (e.g., 3–6 versus 6–12 months). Random effects for age and age 2 were included within the mixed model to account for the correlation between repeated growth measurements from the same child. The interactions of age and infant feeding duration categories were tested, and only those associated with the outcome (p < 0.05) were retained in the model as fixed effects. Data analyses were performed using SAS version 9.4 (SAS Institute, Cary, NC).
Results
A total of 269 women completed the follow-up study and had growth data available for their child (Fig. 1). The majority were white (84%), between the ages of 31 and 40 years at the time of delivery and married or living with partner at 12 months' postpartum (91%). Over half of the study sample did not perceive financial difficulty at the start of pregnancy, and close to 90% of mothers had received education beyond high school. Less than 25% of mothers received WIC benefits (Table 1).
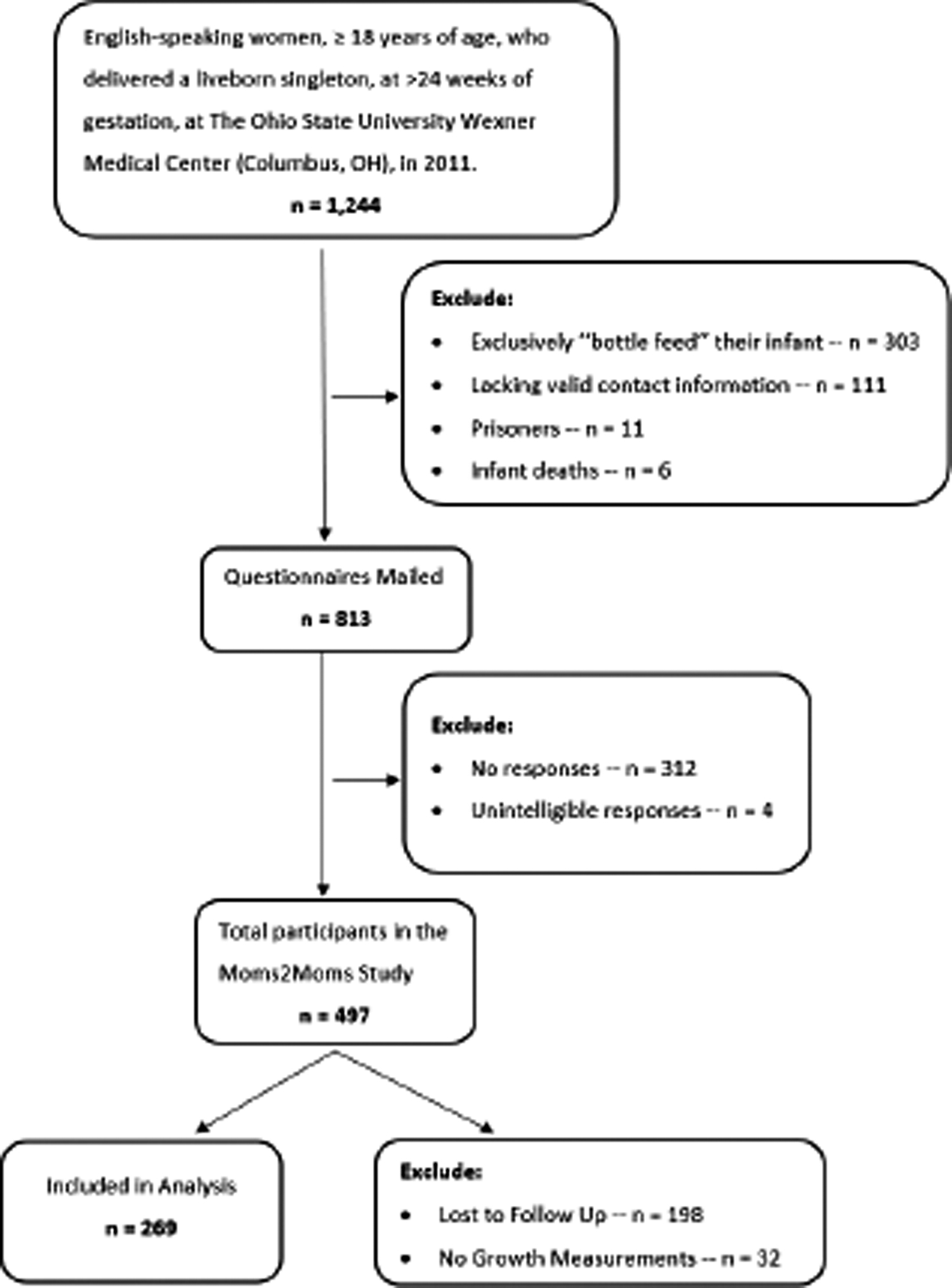
Flow chart of the Moms2Moms study and follow-up (N = 269).
Maternal and Child Characteristics at Baseline, Moms2Moms Follow-Up Study (N = 269)
Thirteen missing for maternal age at delivery.
GED, general educational development; SD, standard deviation; WIC, women, infants, and children.
The median human milk feeding duration for the sample was 240 days (interquartile range [IQR] = 90–365) (Table 2). Infants were fed at the breast for a median 180 days (IQR = 42–365) and fed expressed milk for a median of 150 days (IQR = 49–275). Table 2 provides the association between each infant feeding method and the risk of having excess weight anytime during the first 6 years of life. At least once from birth to age 6 years, 43% (n = 117) of children were considered to have excess weight based on WAZ, 42% (n = 113) of children based on WHZ, and 32% (n = 86) based on BMIZ. However, no infant feeding method was associated with an increased risk of excess WAZ, WHZ, and BMIZ, as all RRs from both unadjusted and adjusted models were close to 1.00 and confidence intervals included the null.
Associations Between Feeding Methods and the Risk of Excess Weight Moms2Moms Follow-Up Study (2017)
Children who were considered to have excess weight if they ever had a WAZ, WHZ, and/or BMIZ >1 standard deviation above the mean.
RRs represent the risk for each additional month of feeding for a particular feeding method.
Adjusted for all characteristics in Table 1.
BMIZ, body mass index-for-age z-score; IQR, interquartile range; RR, relative risk; WAZ, weight-for-age z-score; WHZ, weight-for-height z-score.
Average WAZ and WHZ trajectories did not substantially differ by human milk feeding method as indicated by effect estimates for all the exposure variables being not statistically significant in the mixed models after adjusting for confounders (Table 3, estimates for interactions with age where p > 0.05 not shown). The only possible exceptions were the lower average WHZ with expressed milk feeding for 3–6 months compared with 0–3 months (β = −0.28, 95% CI: −0.59 to 0.03) and the higher average WHZ with exclusive human milk feeding for 3–6 months compared with 0–3 months (β = 0.37, 95% CI: −0.08 to 0.83), which were farther from the null, but confidence intervals for these also included 0. The average BMIZ of children who were fed human milk by any method for 3–6 or 6–12 months was lower by −0.70 (95% CI: −1.36 to −0.04) or −0.50 (95% CI: −0.99 to −0.01) compared with children who were fed human milk for only 0–3 months. The BMIZ trajectory curve also differed by human milk feeding duration as evidenced by the statistically significant interaction with age (β = 0.13, 95% CI: 0.02 to 0.24). Estimates for feeding at the breast were of similar magnitude but estimates for expressed milk feeding were closer to the null for models for BMIZ, although none of these were statistically significant.
Associations Between the Duration of Each Feeding Method and WAZ, WHZ, and BMIZ Trajectories to Age 6 Years, Moms2Moms Follow-Up Study (2017)
The reference group for each model was the “0–3 months” duration group.
Results of the interaction term for age × feeding method category is reported only if at least one of the interaction terms had a statistically were significant p-value (p < 0.05).
Models were adjusted for maternal age at delivery, maternal race, maternal ethnicity, maternal education, marital status, parity, smoking during pregnancy, WIC enrollment in pregnancy or infancy, public or no health insurance, perceived financial difficulty, child sex, cesarean section delivery, birth maturity, age started daycare, and birthweight.
BMIZ, body mass index-for-age z-score; WAZ, weight-for-age z-score; WHZ, weight-for-height z-score; WIC, women, infants, and children.
Discussion
In this longitudinal study focused on contemporary infant feeding methods and long-term weight-related outcomes, 43.5% of the children ever had a measured weight that was considered to be excess for age or length/height by age 6 years. However, specific infant feeding methods were not consistently associated with the risk of having excess weight. Mixed models indicated a reduced risk of excess BMIZ with longer total human milk feeding (feeding at the breast and feeding expressed milk combined), but results did not identify feeding at the breast and feeding expressed milk as having their own estimated effects on outcomes.
The results are comparable with those of a pilot study (n = 37) by Bartok, which examined the association between delivery method of human milk (directly at the breast versus bottlefed) and child growth during the first 6 months of life. They found no major differences in growth between infants predominately fed at the breast (n = 19) and those fed human milk using a bottle (n = 18), including WAZ, WHZ, and BMIZ. However, the ability to detect differences may have been hampered by the small sample size, and the outcome was measured in infancy only. 18
In contrast, other studies point toward a relationship between particular methods of feeding and child weight gain, with feeding directly at the breast and bottle feeding associated with decreased and increased short-term obesity risk, respectively.10,12,19 Li et al. surveyed mothers of ∼2,000 infants to assess the association between feeding method (directly at the breast or via bottle), substance given (human or nonhuman milk), and weight gain over the first 12 months of life. Compared with bottle feeding of human milk, feeding directly at the breast was associated with slower monthly weight gain.2,11 Because this study examined growth during infancy only, it is difficult to directly compare their results with this study, which extend to age 6 years.
Although other studies did not distinguish between specific feeding methods, several reported a reduced risk of obesity with longer breastfeeding duration (likely primarily at the breast given the age of prior studies). Harder et al. performed a meta-analysis examining the relationship between breastfeeding and risk for being overweight later in life. Study populations in the meta-analysis primarily included children ranging in age from 0 to 6 years; however, one included study examined obesity risk at age 33 years. Overall, longer durations of breastfeeding were associated with a decreased risk of overweight status. 1 Wallby et al. found that longer breastfeeding duration decreased the risk of childhood obesity outcomes at 4 years of age. 19 Similar results have also been reported in adolescents. For example, Gillman et al. found that breastfeeding duration, alongside other maternal health factors, was related to obesity outcomes, with increased duration of breastfeeding predicting a lower risk for overweight status at age 12 years old. 20
Whereas select literature supported the relationship between longer breastfeeding duration and lower obesity risk, other studies did not. Burdette et al. found that adiposity at age 5 years did not significantly differ by breastfeeding duration, nor did it differ between children ever or never breastfed. 21 Furthermore, in the PROBIT, Kramer et al. found that measures of adiposity, such as body mass index (BMI), at age 6.5 years did not differ by duration of exclusive breastfeeding. 22 Of interest, in a follow-up study of the PROBIT trial, Martin et al. found that longer duration and exclusivity of breastfeeding resulted in a greater rate of change in BMI between 2.5 and 8.5 years of age, leading to an overall higher prevalence of overweight/obesity at 16 years of age. 6
Although the results of this M2M follow-up study were imprecise, some results suggested that longer duration of human milk feeding was associated with a decreased risk of excess BMI across early childhood. The literature suggests that mothers who breastfeed their children are more responsive to infant hunger and satiety cues and are less likely to develop controlling or restrictive feeding styles that are associated with child weight gain and poor eating habits. 11 In general, past literature remains unclear concerning the overall association between breastfeeding and risk for obesity later in childhood after the infant feeding practice has stopped. However, in a meta-analysis conducted by Horta et al., breastfeeding was negatively associated with overweight and obese status. 23 Their meta-analysis, comprised 113 studies with outcome age ranges spanning from childhood to adulthood, showed that breastfeeding led to a 26% reduction in the risk of becoming overweight or obese.4,23 This study adds to the literature through comparisons of feeding method, durations of those methods, and measures of excess weight.
One limitation of this study was that it relied on retrospective maternal reporting of feeding history at 12 months postpartum. However, the recall period in this study is significantly shorter than in previous studies, which have reported strong recall accuracy up to 6 years after delivery.24,25 Second, the ability to generate precise estimates was limited by the sample size. Like many studies in the breastfeeding field, the sample participants were commonly white, married/partnered, had private insurance, and many children had excess weight at some point by age 6 years. Therefore, the results of this study may not be generalizable to the general population. 26 Pediatric medical records were the source of the outcome data, not research-trained anthropometrists. Anthropometric measurements were collected at Nationwide Children's Hospital and at the children's pediatric care providers across the region as part of routine care. Although precise methods of measurement may have differed slightly between care providers, there is no reason to expect that measurement techniques would differ by breastfeeding method, duration of that method, or the child's weight status. Although this could be considered a source of measurement error, past studies have shown clinical weight and height measurements to be suitable for most research purposes, and there is no reason to believe that this would differ jointly by exposure and outcome.27,28 Furthermore, as shown in work by Kramer and Kramer et al., there is some evidence for reverse causality: infant growth predicts maternal feeding behavior. Mothers may subsequently adjust feeding method in response to their child's growth over the first 6 months of life.29,30 Finally, residual confounding by maternal BMI and other variables is a possibility in this study because those data were not available to include in the models. Some studies have reported positive associations between maternal prepregnancy BMI and gestational weight gain with childhood BMI.31,32
This study had several strengths. First, the sample was from a large academic medical center followed from birth to age 6 years. Second, the infant feeding data were detailed enough to enable examination of distinct categories (human milk feeding, feeding at breast, expressed milk feeding, exclusive human milk feeding, exclusive feeding at breast) to better understand the impact of exclusivity of a particular method on future weight status. Finally, the longitudinal nature of this study and statistical methods allowed for childhood weight-related outcomes to be analyzed with repeated measures over a 6-year time span while not omitting children because of missing data at any particular individual time point.
Conclusions
This study found no clear associations between infant feeding methods like feeding at the breast and feeding expressed milk and the risk for excess weight from 0 to 6 years of age, although human milk feeding in general was associated with lower average BMIZ from birth to age 6 years. Larger studies with similar objectives would help clarify the associations between these contemporary infant feeding methods and the risk of excess childhood weight gain.
Footnotes
Acknowledgments
The authors thank the women who participated in the Moms2Moms and Follow-up Study and Katie Smith, Taniqua Ingol, Chelsea Dillon, Kendra Heck, Rachel Ronau, Hanna Schlaack, Erin Shafer, Thalia Cronin, Justin Jackson, and Kamma Smith (Nationwide Children's Hospital).
Disclosure Statement
The authors have no relevant financial interests, activities, relationships or affiliations that pose a conflict of interest. The authors have no consultantships, honoraria, stock ownership, equity interests, arrangements regarding patents, other vested interests related to this research to report. J.M.M. wrote the first draft of the article and no honorarium, grant, or other form of payment was given to anyone to produce the article. There are no reprints.
Funding Information
The project described was supported by the Grant 1R03SH000048 from the Centers for Disease Control and Prevention and Award Number Grant UL1TR002733 from the National Center for Advancing Translational Sciences. The content is solely the responsibility of the authors and does not necessarily represent the official views of the Centers for Disease Control and Prevention, the National Center for Advancing Translational Sciences, the National Institutes of Health, or the Department of Health and Human Services. The funders had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review or approval of the article; and decision to submit the article for publication.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.