
Abstract
Background:
Breast milk reduces morbidity and mortality in infants admitted to neonatal intensive care unit (NICU).
Objectives:
We determined predictors of procuring mother's own milk (MOM) among NICU-admitted newborn–mother dyads: (1) initiation of any milk expression; (2) initiation of milk expression within 6 hours of birth; (3) MOM as the first enteral feeding; (4) colostrum for oral care within 36 hours of birth if not yet orally fed; and (5) provision of MOM at 21 days of life or discharge, whichever occurred first.
Methods:
We performed a retrospective chart review of NICU-admitted newborn–mother dyads at an urban medical center from June 1, 2018–May 31, 2019. We excluded infants not directly admitted to the NICU, those never enterally fed, multiple gestations if not the first to be discharged, and infants discharged to a nonbiological caregiver. We used chi-square analysis to examine unadjusted associations between independent variables and MOM outcomes and then used logistic regression to determine the adjusted odds ratio and 95% confidence interval (AOR [95% CI]) for predictors of MOM outcomes.
Results:
There were 341 mother–infant dyads who met inclusion criteria and 71% of these mothers initiated milk expression. Smoking, multiparity, gestational diabetes, and Hepatitis C lowered the odds for at least one MOM outcome; whereas mothers who delivered at 28–32 weeks versus ≥33 weeks, and infants with birthweight <1,500 g versus 1,500–2,500 g had higher odds for at least one MOM outcome.
Conclusion:
Maternal/infant dyad characteristics may predict some, but not all NICU breastfeeding outcomes. This suggests that hospital practices may influence these outcomes and can inform future interventions.
Introduction
Mother's own milk (MOM) is widely recognized as the gold standard source of nutrition for all infants, especially those born prematurely, to achieve optimal growth, development, and long-term health. 1 Preterm birth (<37 weeks gestational age) affects 10% of all live born infants and remains one of the leading causes of child mortality and morbidity in the United States with preterm birth and very low birth weight accounting for 17% of infant deaths.2,3 Prematurity constitutes an overwhelming majority of neonatal intensive care unit (NICU) admissions each year and those admitted to the NICU are disproportionately disadvantaged to the provision of MOM.4–6
Breast milk provides infants with critical nutritional and immunologic protections and decreases the risk of several complications of prematurity, including sepsis 7 and necrotizing enterocolitis, 8 and is associated with improved neurodevelopmental outcomes. 9 Despite strong evidence that MOM is the optimal feeding choice, mothers whose infants are admitted to the NICU, particularly if they deliver prematurely, are vulnerable to several challenges in providing sufficient milk to meet the needs of their infants.
There are several factors reported to be associated with decreased provision of MOM feedings during the NICU stay. These factors include older maternal age, delivery at earlier gestational age, male infant, multiple gestations, maternal smoking, primiparity, and cesarean delivery.10–15 Most of these factors are predictive of the degree of provision of MOM at discharge from the NICU. While it is well established that the early provision of MOM is associated with an increased likelihood of MOM at discharge in infants admitted to the NICU,11,12,15,16 less is known about factors that influence early MOM outcomes. Thus, a better understanding of the factors associated with MOM outcomes occurring earlier upstream in the NICU hospitalization is critical for improving MOM at discharge.
Our objectives were to determine predictors of procurement of MOM among NICU-admitted newborn–mother dyads: (1) initiation of any milk expression, (2) initiation of milk expression within 6 hours of birth; (3) MOM as the first enteral feeding; (4) colostrum for oral care (COC) within 36 hours of birth if not yet orally fed; and (5) provision of MOM at 21 days of life or discharge, whichever occurred first. We chose these particular outcomes as they are quality improvement metrics in specific populations within our institution, including maintenance of Baby-Friendly designation and a necrotizing enterocolitis reduction initiative.17,18
Methods
This study was conducted in a 60-bed, level III NICU at the University of Cincinnati Medical Center (UCMC), a Baby-Friendly designated, urban, academic medical center with ∼600 inborn NICU admissions per year, and 3.8 full-time equivalent lactation consultants. Policies at UCMC which support the provision of MOM in the NICU include adherence to Baby-Friendly hospital guidelines, explicit contraindications to providing MOM, and the requirement of a written physician order for supplementation. 18 UCMC follows a standardized feeding protocol for very low birthweight (VLBW) infants (<1,500 g), which includes feeding within the first 48 hours of life (while awaiting MOM for up to 36 hours). In cases of separation of infant from mother, staff are encouraged to assist in milk expression as soon as possible after delivery, with a goal of within 6 hours. In addition, donor milk is routinely provided to VLBW infants in the absence of MOM. COC is provided (with a goal of within 36 hours of life) in infants who are not orally fed. Ongoing efforts to improve maternal milk expression and breastfeeding outcomes in the NICU occurred during our study period, including a larger interventional study involving nurse education on hand expression conducted by the lead author.
A retrospective chart review was performed on inborn NICU admissions at UCMC from June 1, 2018–May 31, 2019. Infants of all gestational ages and birthweights were included. Admission data were obtained using a manual log book maintained by the NICU Health Unit Coordinator. Infants were included if born at UCMC during the study period, directly admitted to the NICU after birth, received at least one enteral feeding during their hospital stay, and were discharged home with their biologic mother. Only single mother–infant dyads were included. Infants were excluded if admitted from an outside hospital or born at home, admitted to the NICU after receiving nonintensive level of care (i.e., well newborn care in-room with mother or transitional care nursery), never enterally fed during hospitalization, duplicate admission due to readmission, multiple gestation if not the first to be discharged home, or discharged to a nonmaternal (biological) caregiver (i.e., cases of adoption, foster care, safety plan, surrogacy, and so on). Because we linked the mother and infant in this study, we elected to include only one infant in the case of multiple gestations so that the mother would not be included more than once. We chose to include the first multiple to be discharged home to assume the “best case scenario.” Specific eligibility criteria for each outcome are summarized in Figure 1.
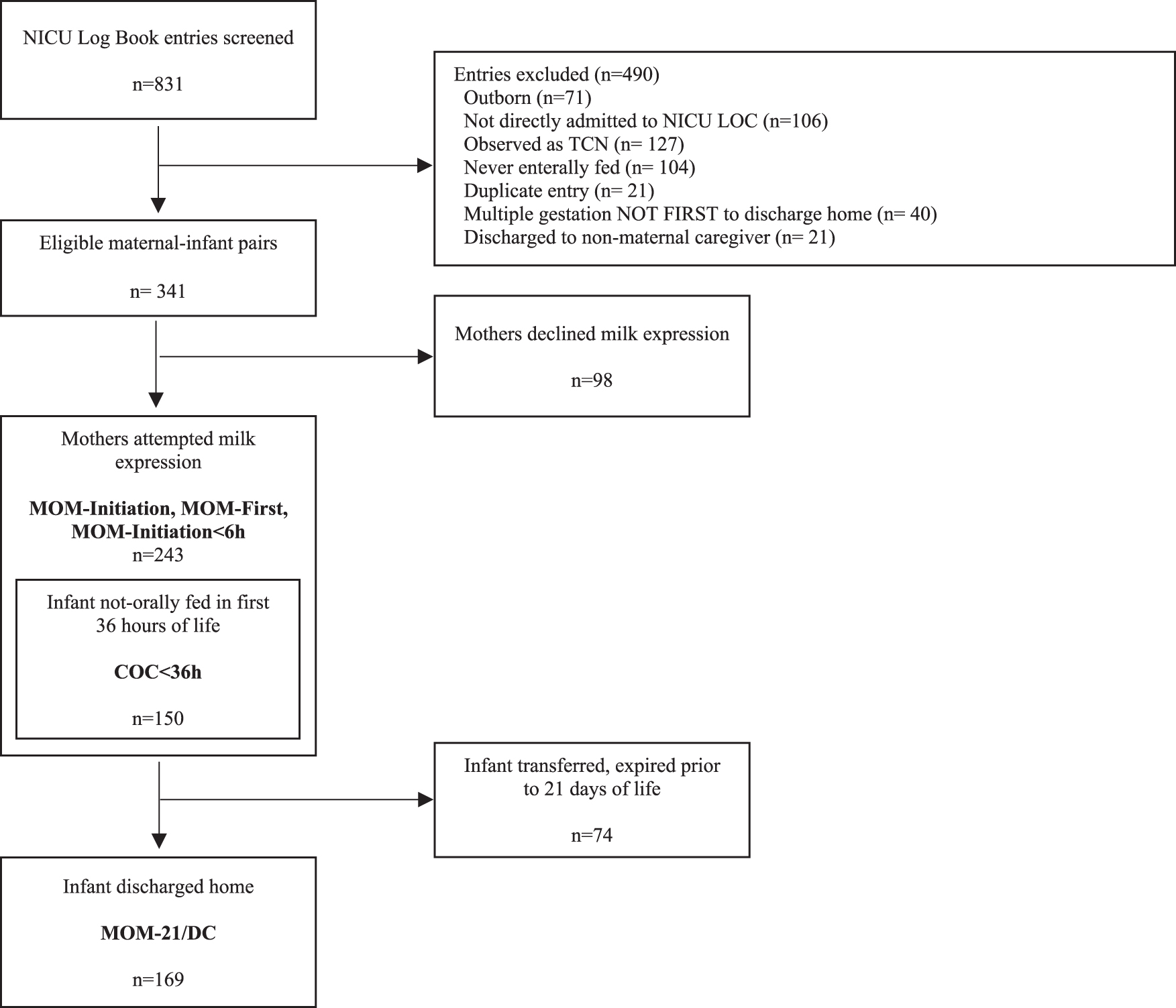
Inclusion flow diagram.
Comprehensive sociodemographic, maternal, infant, and hospital variables were extracted from the chart to determine potential predictors of MOM outcomes. These outcomes included (1) the proportion of mothers who initiated breast milk expression (MOM-initiation), (2) the proportion of mothers who attempted milk expression within the first 6 hours after delivery (MOM-initiation <6 hours), (3) the proportion of infants that received MOM as their first enteral feeding (MOM-first), (4) the proportion of nonorally fed infants that received maternal COC within the first 36 hours of life COC <36 hours), and (5) the proportion of infants receiving any MOM at 21 days of life or within 24 hours prior discharge, whichever came first (MOM-21/DC). This combined measure was chosen as an intermediate marker for breast milk sustainability.
Existing quality improvement records for VLBW infant feeding practices and early colostrum practices for all nonorally fed infants (regardless of birthweight) were utilized. Measures of maternal milk expression for all infants and infant feeding practices for infants where birthweight was >1,500 g were manually extracted via chart review. The primary author audited 10% of charts where manual extraction was used to ensure reliability.
An analytic database was created by linking independent variables from maternal and infant medical records and merging these records to the “MOM outcomes” database as well as the existing VLBW infant feeding practices records and early colostrum practices records to create a single mother–infant dyad analytic database. Bioinformatics staff at the University of Cincinnati College of Medicine and Cincinnati Children's Hospital Perinatal Institute facilitated database assembly. We protected participants' anonymity and confidentiality by excluding any identifying information in the final analytic database. The overall study was approved and overseen by Cincinnati Children's Hospital Institutional review board.
All data were imported into SAS for analysis. Contingency tables and chi-square analysis were used to examine unadjusted associations between independent variables and MOM outcomes. Independent variables were organized into four dimensions: (1) maternal sociodemographic characteristics, (2) maternal preexisting health conditions, (3) maternal obstetric variables, and (4) infant characteristics. After examining bivariate associations, we used logistic regression analysis to estimate the odds ratio (OR) and 95% confidence interval (CI) in multiple variable models. We built our models in steps, starting with the variables with p-values <0.10 in chi-square analysis in each of the four dimensions. Thus, Model 1 was adjusted for maternal sociodemographic characteristics (dimension 1 variables) with p-values <0.10 in chi-square analysis. Dimension 1 variables that were significant at p < 0.05 in the Model 1 logistic regression model were carried over to Model 2, to which we added maternal preexisting health conditions (dimension 2 variables that were significant at p < 0.10 in chi-square analysis). Variables that remained significant (p < 0.05) in the adjusted logistic regression Model 2 were carried forward to Model 3 and so on. In all logistic regression models, we included adjustment for delivery occurring before or after the nurse education intervention on hand expression that was described in the Introduction.
We estimated that at least 200 inborn NICU admissions would meet study selection criteria within the study time frame. For a two-tailed large sample Z-test with significance level of p < 0.05, n = 200 will achieve power of 0.80 to identify approximately twofold difference in prevalence of significant predictors for each outcome, assuming that about 50% achieve each outcome. Using the general rule-of-thumb that acceptable CI coverage can be achieved using 10 events per covariate, we were able to include up to 20 significant covariates in each logistic regression model.
Results
Overall, 341 mother–infant dyads met inclusion criteria, Figure 1. Of these, 243 (71.3%) mothers attempted breast milk expression; 136 (56%) initiated expression within 6 hours of birth, and 105 (43.2%) of their infants received MOM as the first feeding. Of the 243 mother–infant pairs who attempted breast milk expression, 150 of the infants were not being fed orally at 36 hours of life and 85 (56.7%) of these infants received COC within 36 hours of life. Of 169 infants discharged home before 21 days of life, or still at UCMC at 21 days of life, 143 (84.6%) were receiving any amount of MOM at this time.
Unadjusted bivariate associations between the study independent variables and our MOM outcome measures are shown in Table 1. In bivariate analysis, MOM-initiation was significantly associated with health insurance status, smoking status, Hepatitis C positive status, parity, prepartum length of stay, rupture of membrane status, infant gestational age, and birthweight. There were no significant differences in MOM-initiation <6 hours based on maternal or infant characteristics. MOM-first was significantly associated with maternal diabetes status (any or gestational) and infant birthweight. Among infants not initially fed orally, COC <36 hours was significantly associated with race and diabetes status (any or gestational). MOM-21/DC was significantly associated with infant gestational age, birthweight, and perinatal Hepatitis C status.
Mother's Own Milk Outcomes Stratified by Maternal and Infant Characteristics
The square boxes indicate p values that are statistically significant.
Number (percent) in the category who achieved the outcome; ∼0 initiated breast expression out of 5 with positive substance abuse screen.
COC, colostrum for oral care; MOM, mother's own milk; MOM-21/DC, proportion of infants receiving any maternal breast milk at 21 days of life or discharge, whichever occurred first.
After adjustment in multiple variable logistic regression analysis, smoking status, parity, prepartum length of stay, and infant gestational age were all significantly associated with MOM-initiation, Table 2. Infants whose mothers had gestational diabetes were less likely to receive MOM-first, Table 2. Black or African American race and gestational diabetes were significantly independent predictors of infant not receiving COC <36 hours. Infants with Hepatitis C positive mothers were less likely to receive MOM-21/DC, whereas infants with birthweight <1,500 g, compared to 1,501–2,500 g, were more likely to receive MOM-21/DC, Table 2.
Fully Adjusted Logistic Regression Models Predicting Positive Breast Milk Outcomes
The bold highlights in the adjusted odds ratios represents the statistically significant values.
All models are adjusted for whether birth occurred before or after implementation of nurse training on hand expression; otherwise, only significant variables (p < 0.05) were carried forward to the final model.
None of the variables showed statistical significance in predicting mother initiating milk expression within 6 hours of birth.
MOM, mother's own milk; MOM-21/DC, proportion of infants receiving any maternal breast milk at 21 days of life or discharge, whichever occurred first.
Discussion
The results of this study indicate that while there are maternal sociodemographic characteristics, maternal preexisting health conditions, maternal obstetric characteristics, and infant characteristics that are predictive of MOM-initiation, and the provision of MOM at discharge, not all of these factors were consistently associated with the earlier MOM outcomes. This suggests that hospital practices, rather than dyad-specific characteristics, may influence these outcomes. We found that maternal insurance type was not significant after adjustment in logistic regression. This differs from other studies that found that maternal insurance was independently associated with infant feeding type, with infants born to mothers with private insurance more likely to receive exclusive human milk feeding (p < 0.01). 11 We found no significant predictors of early initiation of milk expression (MOM-initiation <6 hours), indicating that this outcome may be mostly influenced by the individual health care provider who is assisting the mother. Previous research found mothers who initiated breast milk expression within the first 6 hours of birth produced significantly higher milk volumes in the early postpartum weeks compared to mothers who initiated expression later.11,15,19 The optimal timing of initiation of milk expression within those first 6 hours is less clear. In a small pilot study, Parker et al. found that initiation of milk expression within the first hour of delivery was associated with increased MOM production. 20 However, these authors recently published results from a larger randomized controlled trial that did not confirm their initial findings. Rather, they demonstrate higher milk volumes in mothers who initiated expression between 3 and 6 hours, compared to <3 hours after delivery. 21
Of the five MOM outcomes, black/African American race was only a significant negative predictor of COC <36 hours. Since we did not observe similar differences in the outcomes for MOM-initiation and MOM-first, the disparity in the outcome for COC <36 hours warrants further examination of potential biases in the workflow between mothers expressing colostrum and their infants receiving it. Previous research has not demonstrated this difference specifically, but has found that infants born to black/African American mothers received less human milk during hospitalization and were less likely to receive any human milk at NICU discharge.13,14,22–26
In our analysis, women who never smoked had sixfold greater odds of initiating milk expression compared to active smokers, and mothers without Hepatitis C had fourfold greater odds of providing MOM at discharge or day of life 21. The CDC does not recognize either of these conditions as a contraindication to providing breast milk to the infant. 26 These results could be explained by hidden confounding factors in mothers who smoke or have a positive Hepatitis C diagnosis or a lack of provider awareness and/or support of the recommendations for providing breast milk under these circumstances. A study by Craighead and Elswick found that maternal smoking and maternal medical risk factors were predictors of noninitiation of milk expression, and that smoking was associated with a shorter duration of provision of breast milk. 14
Similar to other studies, we found that primiparous mothers had about twofold greater odds of attempting breast milk expression. One study found that multiparity was one of the greatest risk factors for mothers not providing milk for their infants in the NICU. 26 Pineda et al. observed more parental presence in the NICU when the family had fewer children, which could facilitate the provision of MOM. 27 Multiparous mothers may have previously experienced breastfeeding difficulties, which could render them disinclined to provide milk. Mothers with a previous NICU experience were found to be at risk for later milk expression in other studies. It is commonly thought that this finding might be attributed to inadequate counseling and reliance on mother's previous experience by the health care staff. 15
A longer maternal antepartum hospital stay (≥2 days) was associated with an increased likelihood of milk expression by more than twofold. While previous studies revealed a higher likelihood of breastfeeding noninitiation in the NICU when there were limited prenatal visits (≤5), 26 a longer antepartum hospital stay could result in greater opportunity for staff counseling and education on the benefits of MOM, which could motivate mothers to attempt milk expression.
We found that mothers who delivered at 28–32 weeks gestation were significantly more likely to provide milk than mothers who delivered at 33 weeks gestation or later. This could be due to hospital policies and practices that place greater emphasis on assisting mothers of the most vulnerable infants with breast expression, which may inadvertently result in the perception that mothers of bigger and more mature NICU infants require less lactation support. Similarly, infants with a lower birth weight (≤1,500 g) had almost eightfold greater odds of receiving any MOM at 21 days of life or discharge compared to infants born at 1,501–2,500 g. This finding is inconsistent with other research that has found increased human milk feeding at discharge to be more associated with older gestational age and greater birthweight. 22 One other study found that infants with birth weight 1,400–1,499 g were more likely to be discharged on breast milk feeding. 13
Infants of mothers with gestational diabetes had threefold greater odds of not receiving MOM as the first feeding or COC <36 hours. Mothers with gestational diabetes are at risk for delayed lactogenesis and a low milk supply. 28 Furthermore, women with low milk supply are more likely to have had diabetes in pregnancy compared with women diagnosed with latch problems. 29 This suggests that gestational diabetes may impact the early provision of MOM to NICU infants. Further study is needed in this population to target interventions to improve lactation outcomes.
Limitations
As a single-center study, with site-specific policies and procedures, our results may not be generalizable to other institutions. A multicenter study is warranted to better understand the influences of hospital-based practices on provision of MOM in the NICU. In addition, we were limited by the variables available in the medical records of the mother and infant. For example, maternal body mass index (BMI) was a variable of interest, as maternal obesity is a known risk factor for breastfeeding difficulties. 30 However, BMI was not consistently documented in the hospital medical record. Furthermore, maternal education is associated with breastfeeding rates, and we did not include this factor in our analysis. However, there is strong covariance between maternal education and insurance status, 31 which we did include in this study, and could serve as a proxy for the former variable.
Strengths
Strengths of this study include the link between mother–infant records and specifically examining the association of variables with MOM outcomes across the continuum of the NICU stay, particularly in the earlier timepoints in the hospitalization. In addition, we had a larger sample size that included NICU-admitted infants of all gestational age and birth weight categories, allowing for detection of meaningful differences in outcomes across categories of independent variables.
Conclusion
In the context of a NICU setting, we identified characteristics of mothers and infants at risk for poor breastfeeding outcomes at certain points of the hospitalization, but not at others. This suggests that hospital practices may influence some of these outcomes. While many NICUs have policies to ensure strong counseling regarding the benefits of MOM for VLBW infants, our analysis suggests lactation support should also be prioritized for more mature infants in the NICU. Race did not have an effect on most MOM outcomes; however, black/African American infants were significantly less likely to receive COC <36 hours than white infants. This difference requires further investigation to ensure that the disparity is eliminated. In addition, mothers with gestational diabetes or Hepatitis C could benefit from targeted support ensuring best lactation practices should their infants require NICU admission.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.