
Abstract
Introduction:
Exclusive breastfeeding is recommended for an infant's first 6 months of life. If unable to breastfeed, expressed breast milk, including donor human milk (DHM), is recommended for optimal nutrition. Benefits of DHM in preterm infants have been established by extensive research. However, less is known about DHM use in other populations.
Objective:
To conduct a scoping review of the literature regarding DHM use in populations other than preterm infants.
Materials and Methods:
PubMed and Clinicaltrials.gov were used to search for articles and clinical trials published between January 1, 2000 and February 29, 2020. In total, 182 articles and reports were identified and screened by 2 independent reviewers.
Results:
Twenty-six articles met inclusion criteria and were reviewed. Studies were mostly observational in design and included infants born >35 weeks gestational age with health risks (9/26) and healthy infants (14/26). Most studies in infants with health risks (7/9) investigated clinical outcomes, with small, observational studies suggesting potential improvements in feeding tolerance and gastrointestinal health. Regarding healthy infants, no studies addressed growth, only one study measured clinical outcomes, and findings related to breastfeeding outcomes were conflicting. Over half of the studies reviewed (15/26) were not designed to establish a potential relationship between DHM use and relevant health-related outcomes.
Conclusion:
The current evidence of DHM use in populations other than preterm infants is limited by lack of direct health measures and infrequent use of randomized trials. More research is warranted to investigate clinical, growth, and breastfeeding outcomes.
Introduction
The American Academy of Pediatrics (AAP) and World Health Organization (WHO) recommend exclusive breastfeeding for an infant's first 6 months of life and continued breastfeeding for at least 1 year.1,2 These recommendations are backed by studies that have reported several benefits of breastfeeding for the infant, including reduced risk of respiratory tract infections, gastrointestinal tract infections, allergic disease, and infant mortality. 1
However, not all infants are able to be breastfed or receive their mother's expressed milk. Regardless of the mother's decision to breastfeed, preterm infants weighing <1,500 g are recommended to receive an exclusive human milk diet, either mother's own milk (MOM) and/or donor human milk (DHM). 3 These recommendations are supported by evidence of reduced necrotizing enterocolitis (NEC) in preterm infants receiving DHM compared to bovine formula.4,5 DHM use with preterm infants has rapidly increased in United States over the past 10 years with the majority of neonatal intensive care units (NICU) now utilizing DHM.6,7
For healthy term breastfed infants, the AAP and WHO also recommend feeding DHM if MOM is unavailable or inadequate, although the extent that this is practiced is not well understood.1,2 The WHO recommendations are part of the Baby-Friendly Hospital Initiative (BFHI) that was launched in 1991 to ensure mothers receive proper breastfeeding education and support in the first days postpartum. Step six of BFHI states that infants are not fed any fluids or foods other than breast milk, which promotes the use of DHM when infants are unable to receive MOM. 8 The number of BFHI hospitals in the United States increased from 60 in 2007 to more than 600 in 2019, with births in BFHI hospitals now accounting for almost 30% of U.S. births. 8
There is little known about the extent or impact of DHM use in populations other than the preterm infant. Therefore, the primary purpose of this scoping review was to describe the nature and findings of research using DHM in populations other than the preterm NICU infant and identify gaps in the existing literature.
Methods
We conducted a systematic scoping review of peer-reviewed research, conference abstracts, and registered clinical trials related to DHM use in populations other than premature infants in the NICU. 9 The Preferred Reporting Items for Systematic Reviews and Meta-Analyses checklist were utilized to guide the reporting process. Electronic sources used to identify articles were PubMed and Clinicaltrials.gov. Keywords and MeSH terms used in the electronic searches included the following: ((“donor milk” or “donor human milk”) NOT (preterm or VLBW or “very low” or review)) for PubMed, and (“donor human milk” or “donor milk”) for Clinicaltrials.gov. Additional studies were located through hand-review of references from the articles identified in the primary search and author familiarity.
Clinical reports, original research articles, conference abstracts, and registered clinical trials that were published or registered between January 1, 2000 and February 29, 2020 were included in this review. Two reviewers (S.M. and M.T.P.) independently assessed all registered trials and study abstracts for inclusion/exclusion criteria. Abstracts were excluded for the following reasons: intended DHM recipient was only premature infants <35 weeks gestational age; did not use DHM, including milk sharing only studies; review article or commentary; not written in English; or did not discuss intended recipients (milk only studies). Trials identified through the online Clinical Trials database were included if the protocol described providing DHM to nonpreterm infant populations. Publications from these trials were identified online at the Clinical Trials database and by individual searches using the investigator name. Trials without published results were included as pending studies. Trials that had been canceled were excluded from the review. Publications that passed abstract review were subject to a full review by two independent reviewers using the same exclusion criteria applied to abstract reviews.
Included studies were abstracted by two reviewers for the following information: intended DHM recipient, intended DHM use, study design, study population, study location, funding source, outcome measures, and results. Studies were categorized into five categories based on the DHM recipient: adult; child; infants born at least 35 weeks gestation with health risks; healthy infants born at least 35 weeks gestation; or postdischarge preterm infants. Six categories were created to organize outcome measures: DHM use patterns (e.g., percent of level 1 hospitals offering DHM, reasons for DHM use, volume of DHM used); knowledge and beliefs about DHM (e.g., perceived benefits and risks); clinical-related outcomes (e.g., length of hospital stay, days parenteral feeding); biomarkers (e.g., bacterial abundance, intestinal inflammation, thymic size); growth (e.g., length, weight, head circumference); and breastfeeding status at or after hospital discharge. Outcomes for each study were coded as positive outcomes (+), negative/detrimental outcomes (−), neutral ( = ), or present, with no longitudinal or control group comparison (P). All reviewer discrepancies were resolved through discussion. Considerations of bias were informed by the Agency for Healthcare Research Quality (AHRQ) methods guide on health care research reviews and included: poor and/or inadequate reporting bias (related to unclear or missing reporting of results and/or methods); study design bias (limitations and weaknesses of methods used); and directness of outcomes bias (research that does not link DHM to an infant health outcome). 10 Studies that only measured patterns of DHM use or knowledge/attitudes about DHM were considered to have not measured direct infant health outcomes. Potential sources of bias for each study were identified and discussed by two reviewers.
Results
An overview of the review process is detailed in Figure 1. The initial PubMed search yielded 151 articles, the Clinicaltrials.gov search yielded 16 studies, 7 articles were found through hand bibliography review of PubMed included articles, and 8 articles were identified from researchers' previous knowledge. After review of the abstracts and study descriptions, 144 articles were excluded leaving 33 articles and 5 clinical trials for full review. Twelve articles/trials were excluded after a full-text review leaving 26 included in this systematic scoping review of DHM use in populations other than the premature, NICU infant.11–36 Included studies were predominantly conducted in the United States in healthy term or late preterm infants (Table 1). Study methods were predominantly observational and descriptive, with only three studies using an experimental design. Study population, intended DHM use, outcome measures, and key findings are summarized in Table 2 by recipient type and intended use. Reasons for DHM use included cancer therapy in adults; pre- and postoperative feedings in infants and children; primary feeding of foster children; and supplementation for healthy breastfeeding infants in the hospital and at home. The frequency of studies by type of outcomes reported was as follows: patterns of use (n = 13), knowledge and beliefs (n = 6), clinical (n = 8), biomarkers (n = 3), growth (n = 4), and breastfeeding (n = 7). Over half of the studies (15/26) were not designed to establish a potential relationship with DHM use and health-related outcomes because they did not compare DHM use to an alternative feeding strategy, they combined DHM with MOM for analysis, or they did not measure infant health-related outcomes.
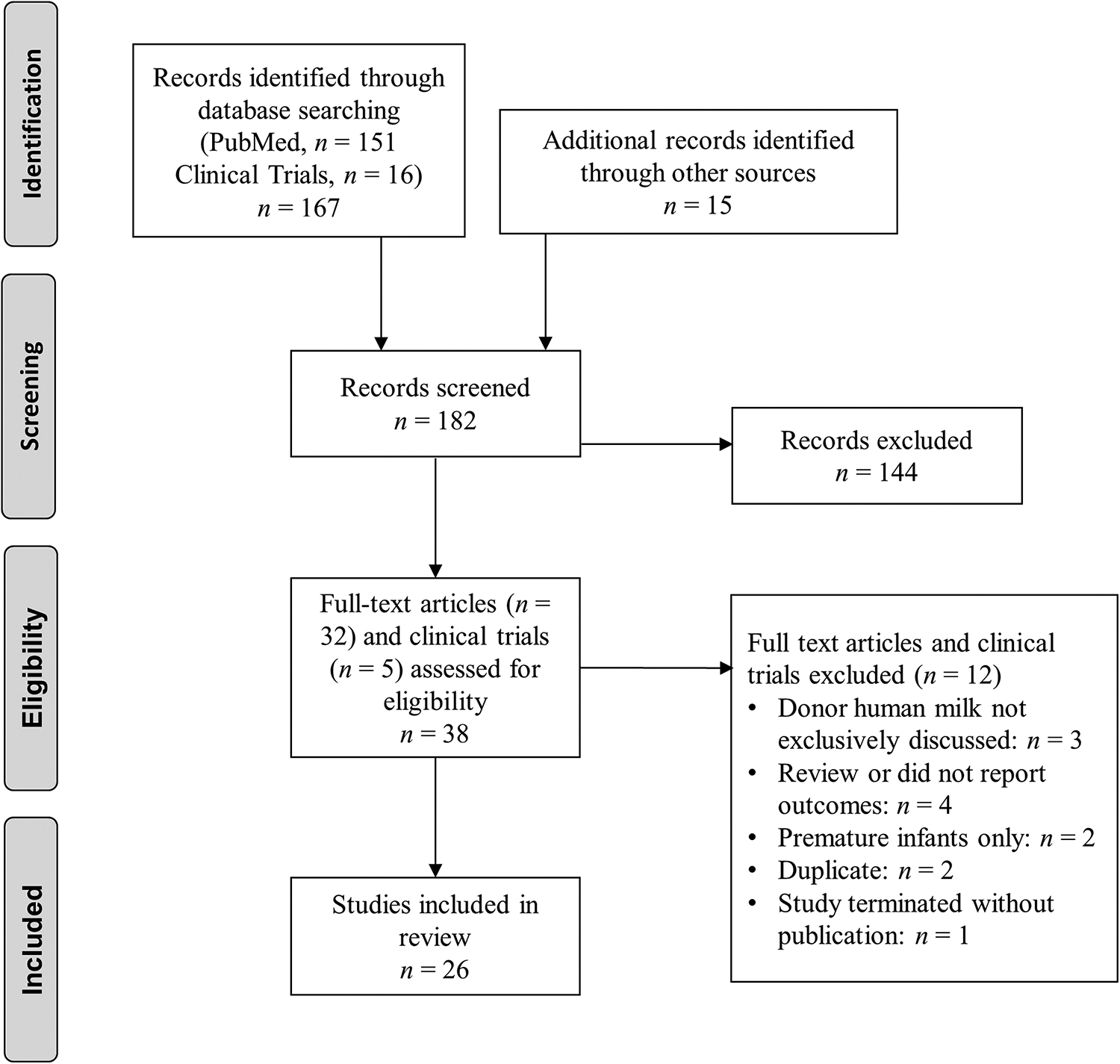
PRISMA flow diagram of the literature search process used to identify studies addressing the use of donor human milk in non-premature infant populations. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Summary of Studies Included in the Systematic Scoping Review of Donor Human Milk Use in Nonpremature Infant Populations
Registered clinical trial with no results published yet.
AGA, appropriate for gestational age; DHM, donor human milk; HIV, human immunodeficiency virus; NICU, neonatal intensive care unit.
Results of Studies Investigating Donor Human Milk for Nonpreterm Population by Intended Recipient and Use
Studies listed in
Adults
A study of 10 adult cancer patients or their proxies reported on DHM use patterns and beliefs. 12 A range of 3.5–16 oz. of DHM was used per day and the majority of participants reported perceived benefits from DHM use; however, no actual clinical outcomes were measured. 12
Children
A single randomized controlled trial (RCT) was conducted in children aged 0–5 undergoing bone marrow transplants. 30 Compared to the controls who received standard formula feeding (n = 14), those who received DHM (n = 18) or MOM (n = 6) had lower markers of intestinal inflammation and lower abundance of certain bacteria posttransplant.
Infants born >35 weeks gestational age with health risks
Patterns of use
Three studies reported DHM use patterns among infants with health risks.22,31,33 In a case study of South African foster children with human immunodeficiency virus (HIV) or malnutrition, DHM was used as a primary source of feeding for 2 weeks to 2 years. 22 In a study of term infants admitted to the NICU (n = 17), Lehman et al. reported that infants were supplemented an average of 900 mL DHM for 4.4 days. 31 Meeks et al. assessed supplementation among term infants admitted to the NICU and found that they received DHM for an average of 5–6 days. 33
Clinical outcomes
Six observational studies measured clinical outcomes in infants with a variety of illnesses and reported a combination of neutral and positive effects with DHM use. Hoban et al. found that infants supplemented with DHM undergoing gastrointestinal surgery (n = 70) did not differ in hospital length of stay, NEC and/or sepsis risk, parenteral nutrition days, or central lines days compared to infants supplemented with formula (n = 70); however, in a subanalysis, including only small bowel atresia and gastroschisis surgeries, infants receiving DHM (n = 58) had significantly shorter hospital stays and central line days than those who received formula (n = 47). 35 Cognata et al. studied infants undergoing cardiac surgery (n = 546) and found that an exclusive unfortified human milk diet (n = 198), including MOM and DHM, was associated with a significantly lower incidence of NEC. 24 Alexander et al. reported that fewer infants with neonatal abstinence syndrome (NAS) fed DHM (n = 9) had Finnegan gastrointestinal subscores above 2 compared to those fed formula (n = 9), but overall Finnegan scores were not different. 16 Mannel and Bennett 32 and Reimers et al. 22 investigated foster infants (n = 1–7) receiving DHM and reported improved feeding tolerance, reduced eczema, and lower infection incidence. Jeppesen et al. reported that HIV-exposed uninfected infants receiving DHM (n = 18) had fewer infections at 8–12 months compared to HIV-unexposed infants receiving formula (n = 47). 14
Biomarkers outcomes
Two studies reported thymic size in HIV-exposed uninfected infants.11,14 Infant's thymic size was greater in HIV-exposed uninfected infants who received DHM (n = 12) at 4 months of age compared to HIV-unexposed infants fed formula (n = 47). 11 However, a later study found no difference in thymic size at 8 and 12 months of age. 14
Growth outcomes
Four observational studies reported mixed findings related to growth.16,22,32,35 Among infants undergoing gastrointestinal surgery, there was no difference in weight or head circumference between infants supplemented postoperatively with DHM (n = 70) and formula (n = 70). 35 In a case study of seven foster infants, Reimers et al. reported improved weight gain after introduction of DHM as their primary feeding. 22 In contrast, a case study of a foster infant whose birth weight dropped from the 56th percentile to the 1st percentile due to formula intolerance reported that the infant's weight remained below the 5th percentile after being fed DHM for over 200 days. 32 In a case–control study of hospitalized infants with NAS, head circumference gains were lower in infants fed DHM (n = 9) compared to infants fed formula (n = 9). 16
Healthy infants born >35 weeks gestational age
Patterns of use
Two studies reported patterns of DHM supplementation for hypoglycemia among healthy infants.15,27 A case study of two infants reported that a range of 45–147 mL of DHM was utilized for supplementation. 15 Ferrarello et al. found that among 83 mother-infant dyads, 76% of parents chose DHM as a supplement for hypoglycemia over formula. 27
Six studies investigated DHM patterns of use for other supplementation reasons among healthy infants.18,19,21,23,25,28 In a 2018 regional survey of 71 maternity hospitals, 32% of hospitals reported that they were using DHM for healthy infants. 18 Sen et al. investigated supplementation patterns at a single U.S. hospital from 2013 to 2016 and found that the percentage of healthy infants receiving DHM increased from 0.04% to 4.7%, with common indications for use, including excessive weight loss, late preterm birth, poor latch, and delayed lactogenesis. 23 Lewis et al. investigated indications for DHM in a level 1 mother baby unit and reported that the three most common reasons for supplementation among healthy infants were excessive weight loss, mother-infant separation, and small for gestational age. 19 Rabinowitz et al. surveyed breastfeeding mothers of healthy infants (n = 24) and reported that 58% preferred DHM supplementation over formula. 21 Regarding hospital policies, Drouin et al. surveyed level 1 maternity hospitals in the Northeast using DHM (n = 15) and found that 87% had policies that stated criteria for DHM, 27% stated DHM was preferred, and all required consent. 25 Kair et al. investigated maternal characteristics by supplemental feeding type and found that dyads that received formula supplementation (n = 376) were more likely to be nonwhite, publicly insured, and/or non-English speaking than dyads who received DHM supplementation (n = 306), raising concerns about health care inequities in DHM access. 28
Knowledge of DHM
Four studies investigated clinician and family knowledge and opinions about DHM supplementation for healthy infants.17,18,21,26 Rabinowitz et al. interviewed postpartum mothers (n = 24) and reported maternal concerns related to safety of DHM and a lack of information. 21 In another study that interviewed postpartum mothers (n = 30), Kair and Flaherman identified four themes, including that formula is familiar and DHM is not, DHM is costly and logistically challenging, DHM is temporary and formula is ongoing, and DHM is “healthier.” 17 Ferrarello et al. reported that nurses (n = 20) lacked knowledge of DHM and presented logistical concerns for implementing a DHM policy in a well-baby nursery. 26 In a survey of clinicians at maternity hospitals in the northeastern United States (n = 71), 78% believed that studies showed benefits of using DHM in healthy term infants, and 94% believed that DHM improved exclusive breastfeeding rates. 18
Clinical outcomes
One study reported clinical outcomes for infants receiving level 1 care. 20 Mannel and Peck found that hospital length of stay did not differ in late preterm infants (n = 183) by feeding type (MOM, DHM, and formula). 20 Thoene is currently investigating DHM supplementation among term infants experiencing hypoglycemia in an RCT that is registered to report blood glucose outcomes. 36
Breastfeeding outcomes
Six studies reported on how DHM use influenced breastfeeding outcomes in healthy infants with conflicting findings between observational studies and a single RCT.15,18,20,27,29,34 Ferrarello et al. reported that among infants supplemented with DHM for hypoglycemia (n = 63), 52% were exclusively breastfeeding at discharge compared to 0% of infants supplemented with formula (n = 20). 26 Belfort et al. found that hospitals who reported using DHM to supplement healthy infants had higher rates of exclusive breastfeeding at discharge compared to those who did not (77% versus 56%, p = 0.02). 18 Mannel and Peck found that the risk ratio of breastfeeding at discharge was 0.84 for infants who received any formula supplementation (n = 93) compared to infants who received expressed human milk (n = 20; 95% confidence interval [CI] 0.77–0.92). 20 Merjaneh et al. found that breastfed infants supplemented with DHM (n = 33) had five times greater odds of exclusive breastfeeding at 6 months compared to infants supplemented with formula (n = 39; 95% CI 1.37–19.23; p = 0.015). 34 Conversely, Kair et al. conducted an RCT of healthy infants with >4.5% weight loss in first 36 hours of life and found that infants randomized to receive early, limited-volume DHM supplementation (n = 30) were not more likely to be breast milk feeding at 3 months than the control group who was instructed to exclusive breastfeed unless otherwise advised by a health care provider (n = 30). 29
Postdischarge preterm infants
Szucs et al. studied supplementation of DHM among postdischarge preterm quintuplets and reported that they received ∼420 oz. DHM per week in addition to mother's milk and were developing normally at 6 months. 13
Discussion
In this systematic scoping review of research using DHM in populations other than hospitalized preterm infants, we found that the majority of studies were conducted in healthy infants (14/26), or infants >35 weeks gestation with health complications (9/26). More than half of the studies (15/26) were not intended to establish a potential relationship between DHM use and health-related outcomes, which suggests a high level of directness of outcome bias in the existing literature.
DHM use in noninfant populations
Research into DHM use in noninfant populations is scarce, with only a single study identified in adult cancer patients that was influenced by selection bias (all participants had independently sought DHM). In addition, no clinical outcomes were directly measured, so potential efficacy of DHM as an adult cancer therapy could not be evaluated. Studies are also limited regarding DHM use in children, with only one RCT investigating DHM use during bone marrow transplants. While the study reported positive outcomes related to intestinal inflammation and bacterial abundance, interpretation is limited by reporting bias due to combining infants who received DHM with those who received MOM when reporting findings.
DHM use in infants born >35 weeks gestational age with health risks
The majority of studies in infants with health risks (7/9) measured health-related outcomes, including clinical findings, biomarkers, and/or growth; however, due to high heterogeneity between populations studied (including infants with NAS, feeding intolerances, HIV-exposure, and cardiac and gastrointestinal anomalies), there was limited ability to synthesize findings across studies. In small case studies of infants experiencing failure-to-thrive, there was consensus of improved feeding tolerance.22,32 In studies measuring growth outcomes, there were inconsistent results, with 2/4 studies reporting inferior growth with DHM feedings.16,22,32,35 Findings of slower growth is in agreement with studies among preterm infants that have reported slower growth with DHM feedings compared to preterm formula,4,37–39 suggesting that future studies should investigate growth outcomes and also measure the macronutrient content of the DHM, as this was not addressed in any of the growth studies included in this review. Future research is also needed in how DHM use among ill infants influences breastfeeding outcomes as limited studies have considered this.
Limitations of research in infants with health risks include the use of study designs that were predominantly observational, cross-sectional, and contained <20 participants who received DHM. Moreover, three studies compared infant groups from two eras separated by multiple years.11,14,35 Due to the time difference, changes in standard of care may have confounded study findings. Of final note is the reporting bias present in two studies that grouped MOM and DHM feedings together when reporting results, which inhibits any conclusions specific to DHM.14,24
DHM use in healthy infants born >35 weeks gestational age
Fourteen studies were conducted in the last 6 years using DHM in healthy infant populations, suggesting that this is a growing topic of interest. A 2018 regional study of 71 maternity hospitals reported that 32% of hospitals were using DHM for healthy infants, although whether these patterns hold nationally remains to be established. 18 Reported uses of DHM included hypoglycemia and/or hyperbilirubinemia, excessive weight loss, delayed lactogenesis, small for gestational age, and maternal-infant separation.19,23,25 Differential patient access to DHM was reported in one study that found nonwhite, publicly insured, and/or non-English speaking mothers received DHM as a supplement less often, raising concerns about health care inequities. 28
The most common health-related outcome studied among infants in level 1 care receiving DHM was the impact on breastfeeding, with conflicting findings reported.15,18,20,26,29,34 Four observational studies reported a positive impact on breastfeeding outcomes at hospital discharge or up to 6 months postpartum. In observational studies, reverse-causation may have been present when DHM use is counted toward definitions of exclusive breastfeeding at discharge, thus confounding findings. Conversely, one RCT showed that no improvement in breastfeeding rates at 3 months postpartum in infants receiving early, limited-volume DHM supplementation for excessive weight loss. 29 Recent RCTs have found that early, limited-volume formula supplementation in the hospital did not impact breastfeeding status at 1 and 6 months among healthy, term infants, which aligns with the findings of the RCT in this review.40,41 Collectively, these RCTs suggest that limited-volume supplementation in hospital, regardless of whether it is formula or DHM, may have minimal impact on breastfeeding outcomes.
Only a single study considered clinical outcomes (length of hospital stay) among healthy infants receiving DHM, 19 and no studies investigated growth outcomes. Directness of outcomes bias is prevalent in the current body of research, with the majority of studies in healthy infants not designed to establish a relationship between DHM use and health-related outcomes. Future research should include randomized trials to investigate the impact of DHM versus formula supplementation on health-related outcomes, including breastfeeding status, clinical outcomes, and growth.
Conclusion
The studies presented in this scoping review identify that DHM is increasingly being used in infant populations other than the preterm, NICU infant. Overall, studies are limited due to directness of outcomes bias, with 15/26 studies not designed to establish a relationship with DHM use and health-related outcomes. More research is warranted regarding DHM use in nonpreterm infants and should include randomized trials investigating clinical, growth, and breastfeeding outcomes. The fact that 80% of the studies in this review were conducted in the last 3 years suggests that DHM use beyond the preterm NICU infant is a rapidly evolving practice and warrants regular reviews of the literature.
Footnotes
Authors' Contributions
S.M. and M.T.P. contributed to study conception, study design, data collection, and data interpretation. S.M. had primary responsibility for writing the article. Both authors reviewed, edited, read, and approved the article.
Disclosure Statement
M.T.P. serves on the Board of Directors for the Human Milk Banking Association of North America in an unpaid capacity. S.M. has no conflicts of interest to report.
Funding Information
The authors report no funding was received for this project.