
Abstract
Objective:
African American (AA) women look to their mother and maternal grandmother for parenting information and support; this intergenerational communication may reinforce or hinder breastfeeding practices. Rooted in Black Feminist Thought, this study's objective was to use an asset-based approach to explore infant feeding information shared across at least two generations of AA female family members.
Materials and Methods:
Fifteen family triads/dyads (N = 35 women), residing in Southeastern United States, participated in semistructured interviews in 2019. Qualitative data were analyzed using thematic analysis.
Results:
Infant feeding information shared across generations was characterized into six themes: Guidance, Practical assistance, Reservations, Affirmations, Observational learning, and Perceived undermining. Typically, conversations occurred in one of four reproductive life stages (preconception, prenatal, birth, and post-birth) of the youngest adult generation and may have been influenced by each family's feeding history (“One generation breastfed,” “Two generations breastfed,” and “Three generations breastfed”). Notably, with each additional generation of breastfeeding experience, perceived undermining and reservation reporting decreased. In addition, families reclaimed and reconnected with ancestral breastfeeding practices.
Conclusions:
Findings suggest that every generation matters to breastfeeding behaviors in AA families. Therefore, nuanced, family-centered approaches should build on assets within AA families to support them in meeting their feeding goals. Practitioners should recognize the importance of oral tradition as a mode of transmitting infant feeding information among AAs and understand the influence of family feeding history in intergenerational infant feeding communication. When working with AAs, practitioners must be flexible, respectful, supportive, and actively learning about an individual's beliefs and culture, creating space to reframe, without judgment or paternalism.
Introduction
Breastfeeding is advantageous for infants, mothers, families, and society.1,2 Initiation and duration rates continue to rise in the United States with 84% of all women and 74% of Black1,* women initiating breastfeeding. 3 Rates differ by geographic location; the Southeastern region has the largest gap between Black women and other races/ethnicities. 3 To improve breastfeeding rates, the U.S. Surgeon General proposed family involvement in breastfeeding support as a critical strategy, 4 underscoring the importance of the family context, where older female family members may play a supportive role in influencing feeding behaviors by sharing their own feeding practices and beliefs. 5 However, many U.S. grandmothers lack breastfeeding knowledge and experience, which may influence the support and advice they can provide to new mothers. 6 Grandmothers who are uninformed or misinformed about current breastfeeding recommendations, or hold negative beliefs and attitudes about breastfeeding, may undermine a mother's breastfeeding confidence,2,7 breast milk supply, 5 and breastfeeding practices. 5 Grandmothers with breastfeeding experience may be able to provide practical breastfeeding knowledge, while grandmothers who lack breastfeeding experiences could potentially convey negative attitudes regarding breastfeeding and encourage formula feeding or supplementation with baby cereal or other solids.8,9
The collectivistic structure of African American (AA) families 10 facilitates understanding of intergenerational communication. Within the family structure, family members (blood relatives and fictive kin) share resources and flexible child rearing responsibilities across households and generations. 11 Elders are “entrusted keepers of communal knowledge and wisdom, informal family historians, and the wisest, most respected members of the family.”12(p117) Matriarchs play an important role in preserving and passing down cultural beliefs and family values, which are fundamental to intergenerational support in their flexible family system.12,13
While AAs experience persistent, disproportionate health disparities compared to whites, 14 the majority of family health communication scholarship (how families talk with each other about health information) predominantly sample white families.15–17 Moreover, few studies examine infant feeding communication, specifically among AAs.18–20 Also, lactation scholars urge future researchers to better understand women's infant feeding decisions.6,21–23 Grassley and Eschiti22(p140) suggested that researchers investigate breastfeeding behaviors among families, including an infant's mother, grandmother, and great grandmother, to “provide insight into the generational aspects of breastfeeding and enhance the understanding of family influences on women's infant feeding decisions.” To address these research needs, this study explored the content and context of infant feeding information shared across at least two generations of AA women.
Materials and Methods
Design
Qualitative research is unique because it examines stories, feelings, and thoughts that are often not accessible through other research methods. 24 Thus, this qualitative study used an asset-based approach and Black feminist research perspective to place AA women at the center of data collection and analysis. 25 Thus, Black Feminist Thought 26 (BFT) was the driving force of this study and encompasses core tenants associated with empowerment, overcoming oppression and changing the narrative of Black women. Semistructured interviews focused on resources and strengths present in AA families to identify solutions to aid continued improvements in breastfeeding rates. This study was approved by the University of South Florida Institutional Review Board.
Purposive followed by snowball sampling was used to recruit 15 family triads/dyads (N = 35 women). Each triad consisted of the youngest adult generation (youngest generation), her mother/mother figure (middle generation), and her maternal grandmother/grandmother figure (oldest generation). Each dyad consisted of the youngest and middle generations. Maternal grandmother and mother figures included grandmothers, aunts, older sisters, older cousins, and stepmothers who were responsible for raising the youngest generation.
Two interview guides were developed: one for the oldest and middle generations and one for the youngest generation. Interview questions were pilot tested with a unique group of six AA mothers who were not study participants. The first author conducted a single, face-to-face or telephone, audio-recorded interview with each participant.
Setting
AA women residing in Southeastern United States were interviewed in 2019.
Sample
Included participants were U.S.-born, English-speaking adult mothers who self-identified as AA, Black, Negro, or colored, belonged to a family with at least two generations of women willing to participate in the study, at least one generation resided in Southeastern United States, and were not estranged from each other. In addition, the youngest generation needed to have breastfed their child (aged 3 months to 5 years old) for a minimum of 3 months.
AA/Black/colored/Negro was defined as a non-Hispanic, U.S.-born person with African ancestry and shared American history. All participants stated to their knowledge that their parents and grandparents were also U.S.-born, reducing dissimilarity in traditions from cultures outside the United States. In addition, breastfed was defined as feeding a mother's own milk, at the breast or expressed, to her infant at least once daily. Women who fed human milk along with infant formula or with baby cereal were considered breastfeeding. Family referred to both biological and nonbiological members, reflecting the structural dynamics of AA multigenerational families and kin networks. 27
Data analysis
Analysis was iterative, starting with keeping field notes throughout data collection. Audio recordings were transcribed, and data were deidentified with pseudonyms. Transcripts and field notes were imported into MAXQDA (version 18.2.0; VERBI GmbH, Berlin, Germany). Two coders independently coded four interviews and resolved disagreements through five cycles of coding. 28 Thematic analysis 29 was used to deductively analyze interviews, while also using inductive coding 30 to identify emergent themes used to make sense of the data. Themes were grouped using thematic maps. 31 Using data collected from participant interviews and field notes, the first author established thick descriptions, 32 which enable other researchers to transfer the research findings to other study settings. Generalizability is often not the goal of primary qualitative research. Nuances within the family communication dynamic were explored resulting in four reproductive life stages of the youngest generation when conversations transpired: preconception [before the youngest generation was pregnant], prenatal [during the youngest generation's pregnancy], birth [the youngest generation's hospital stay], and postbirth [when the youngest generation returned home]. In addition, themes emerged based on each family's feeding history (how many generations breastfed).
Results
Participant characteristics
Thirty-five interviews were conducted with three generations of AA mothers (N = 5 oldest generation, N = 15 middle generation, and N = 15 youngest generation). Participants' age ranged from 24 to 80 years, 57% were married, and all had at least a high school education (Table 1). The youngest generation breastfed their child between 3 months and three and a half years, while 53% of the middle generation and 20% of the oldest generation breastfed at least one child for at least 3 months (Table 2).
Demographic Distribution of Three Generations of African American Families by Generational Membership
Maternal grandmother/grandmother figure.
N (%) of total sample (i.e., down the column).
Mother/mother figure.
Youngest adult generation.
Table. 2. Participant Pseudonyms and Feeding Characteristics
Participants were grouped by generations instead of by family unit to maintain participant confidentiality. This table was organized by generation, then by breastfeeding behavior, then by family feeding history to extract patterns and trends within and across families.
Breastfed is defined as feeding mother's own milk to at least one child for 3 months or more.
1-GB: One Generation Breastfed; Only the youngest generation breastfed in this family feeding group.
2-GB: Two Generations Breastfed; Either the oldest and youngest generation or the middle and youngest generation breastfed in this family feeding group.
3-GB: Three Generations Breastfed; all three generations breastfed in this family feeding group (Note: The oldest generation was not interviewed in 3-GB families, but the middle and youngest generation reported that the oldest generation breastfed).
Themes
Families discussed components of shared infant feeding information across the following themes: Guidance, Practical assistance, Reservations, Affirmation, Observational learning, and Perceived undermining (Table 3). Family feeding history, (One Generation Breastfed [1-GB], Two Generations Breastfed [2-GB], and Three Generations Breastfed [3-GB]), may have influenced specific content and context of conversations. In 1-GB (N = 4 families), only the youngest generation breastfed. In 2-GB (N = 9 families), either the oldest and youngest generation or the middle and youngest generation breastfed. In 3-GB (N = 2 families), all the three generations breastfed. While the middle and youngest generations were in each feeding group, no oldest generation participants were interviewed in 3-GB. In both 3-GB families, the middle and youngest generations reported that the oldest generation breastfed more than 3 months, which is why they are categorized in this group. Although themes aligned across feeding groups, notable differences existed regarding when conversations occurred (i.e., preconception, prenatal, birth, and postbirth). Figure 1 depicts how themes, family feeding history, and reproductive life stages have been conceptualized.
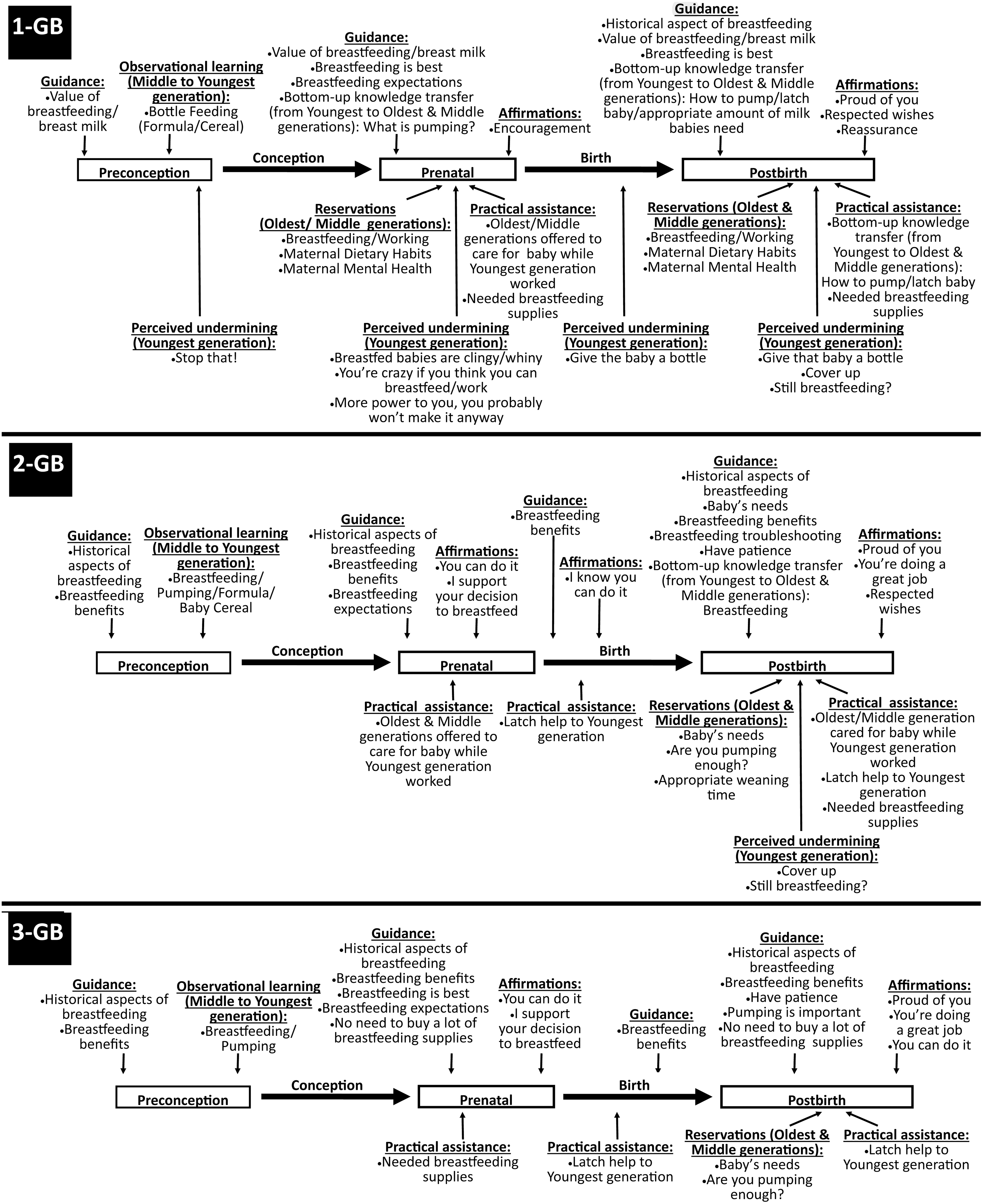
Intergenerational infant feeding information shared in 1-GB, 2-GB, and 3-GB families. GB, Generation Breastfed.
Emergent Themes, Definitions, and Examples
Guidance
Guidance was the shared infant feeding information that included advice and suggestions between generations. All feeding groups discussed historical aspects of breastfeeding from a pro-breastfeeding context (Fig. 1). Louise explained, “I tell [my granddaughter] all the time, this is not our first-time breastfeeding. We did it for white people, so we have to know it's good enough for our children too. We deserve to do this too…again.” And, Valerie recalled,
“[I remember] teaching [my daughter] about the history of enslaved women wet nursing for their white slave owner's children. Breastfeeding should not be something that is taboo in our communities because we were the first to do it. I told her, ‘We fed their [white] babies, so why don't we think we should feed our own?’ I don't know why we ever stopped breastfeeding. I know we may have wanted to distance ourselves from the idea of wet nursing, but that also meant that we wasn't giving our own the very best.”
In addition, all groups provided guidance in the prenatal period on experiencing pain and being uncomfortable. Dominique remembered:
“[My mom and grandma] said it was going to hurt and everything and how their nipples were blistery… when the ducts get blocked and all that. I was like, ‘Ewww.’ But I was still gonna do it anyway. I was like, ‘That is not gonna happen to me.’”
Breastfeeding is best was a topic shared among 1-GB families (prenatal and post-birth) and 3-GB families (post-birth). Sabrina said:
“Oh, we talked about it way before she had [her son]. … I've been trying to coerce her to breastfeed and let her know that I think that's the best thing to do and she was very dedicated to it, and I love her for that…”
Among 2-GB and 3-GB families, physical, psychological, emotional, and financial breastfeeding benefits (all reproductive stages) and the need to have patience (postbirth) were shared. Jennifer stated:
“I was telling her how healthy the babies were… the antibodies and what not. You know, and even when it comes to the weight loss… And not only that…I think emotionally, being more connected with the child. So psychological, physical, you know healthier…I also told her what I did.”
Notable differences between the groups were the value of breastfeeding and breast milk discussed in 1-GB families (preconception, prenatal, and postbirth), troubleshooting breastfeeding in 2-GB families (postbirth), and the importance of pumping and not buying too many supplies in 3-GB families (postbirth).
Guidance and knowledge transfer were typically shared from older to younger generation, but among 1-GB and 2-GB families, bottom-up transfer occurred where the youngest generation shared their knowledge about milk composition, latching, and pumping with the oldest and middle generations. To illustrate, Katrina remembered conversations with her mother about how much expressed milk she needed to leave for the baby once she returned to work: “[Mom would say], ‘You're not leaving enough milk. She's hungry…she needs more milk.’ I'm like, ‘No, she's breastfed…trust me. Milk changes to fit her needs…’ We went back and forth…like literally every day.”
Practical assistance
Practical assistance included infant feeding information involving the provision of help or material resources to the youngest generation. All groups reported conversations about buying breastfeeding supplies. Sharon remembered: “I offered to get her the [pillow]…so she could put him on there and breastfeed…And then…I had ordered a pump for her, too. I told her that way she could, you know, pump milk, too….” In addition, among 1-GB and 2-GB families, older generations offered to care for the baby, while the youngest generation went to work or school (prenatal and postbirth). Sandra remembered, “She was gonna pump the milk in the bottles and bring it over there to me because I was gonna watch him while she worked.” Among 2-GB and 3-GB families, older generations provided latch help to the youngest generation (birth and postbirth). Sabrina recalled, “[M]om was very helpful when it came to getting [my son] to latch on my boobs. At first, I wasn't sure how to do it, but in the hospital, she helped me out…”
Reservations
Reservations included infant feeding information involving worry, fears, or uneasiness from older generations. Among 1-GB families, older generations discussed the following reservations (prenatal and postbirth): working and breastfeeding, having a backup plan, and maternal dietary needs and mental health. Shirley said, “She told me, ‘Momma I'm breastfeeding.’ [And I said], ‘Oh, OK.’ I did ask her how she was gonna be able to breastfeed and work.” Older generations in 2-GB and 3-GB families were concerned if the baby received enough breast milk, and if the youngest generation pumped enough milk (post-birth). Pamela said,
“And when a situation came up and she needed me to watch the kids, I was like, “So what I'mma feed them? They can't drink out of my tits.’ She was like, ‘I'll pump.’ I'm like, ‘Yeah, you need to. You need to pump ‘cause anything can happen.’ It's nothing worse than having a kid that don't want no milk…that don't want that cow's milk or that manmade milk ‘cause they are not used to it. And I said, ‘Even with breastfeeding, you need to get them used to a bottle.’”
In addition, older generations in 2-GB families were uneasy with how long the youngest generation breastfed their child. Barbara said, “[My granddaughter] does it until her kids are big kids…I'm talking about somebody that's over a year old…I told her that that's too long. Her baby is almost 2 and this child is still trying to nurse.”
Affirmations
Affirmations included older generations sharing comfort, assurance, or encouragement with the youngest generation. In all groups, older generations told the youngest generation “I'm proud of you” (postbirth). Amber said, “[M]y mom would tell me she's proud of me. She would also say ‘if that baby want that boob, you give the baby that boob.’” Among 2-GB and 3-GB families, older generations said, “You can do it,” “I support your decision” and “You're doing a great job” (prenatal and post-birth). Pamela expressed: “And I push [my daughter] because I'm like, ‘You can do it.’ I gotta give [her] that little bit of hope. ‘You can do this. You can do this.’” Among 1-GB families, reassurance and encouragement was communicated to the youngest generation. Yolanda revealed, “[My daughter] was really down on herself when she couldn't continue to breastfeed and I was like, ‘You know what, it's okay. The first couple of months is when you get most of the good stuff anyway.’ So, I just like reassured her that it was okay when she couldn't continue to breastfeed….”
Observational learning
Observational learning was infant feeding information shared between the middle and youngest generations through observation. Regardless of feeding history, families reported the youngest generation observed the middle generation's feeding behaviors. Women in 1-GB and 2-GB families recalled the youngest generation observing the middle generation's use of infant formula and/or baby cereal to feed younger siblings. Sherry said, “We didn't necessarily have conversations [when my daughter was growing up], but she learned how to take care of and bottle feed babies by watching us and then she started babysitting other people's children.” Women in 2-GB and 3-GB families remembered the youngest generations observing the middle generation breastfeeding and/or pumping. Valerie said, “…I nursed all of mine. And that's what she grew up seeing. Yeah, it was normal for her.” Asia remembered, “As a kid, I saw [my mom] breastfeed my sister. I knew I wanted to do it too…”
Perceived undermining
Perceived undermining was infant feeding information that the youngest generation perceived lessened their confidence or hindered their overall breastfeeding success. Perceived undermining was reported among the youngest generation in 1-GB families (all reproductive life stages) and 2-GB families (post-birth), but not in 3-GB families. Katrina remembered visiting a cousin in the hospital as a 6-year-old and seeing breastfeeding for the first time. She remembered her mother telling someone on the phone, “Yeah, she breastfed in front of [Katrina].” Once they got home, Katrina “breastfed” her dolls. Her mom angrily yelled, “Why are you doing that? Stop doing that.” According to Katrina, “…[T]hat was the end of it.” In addition, Lashonda said, “With each child, my momma and grandma would ask me all the time how long I planned to nurse for. They thought going past 1 year was too long.”
Discussion
Findings provide evidence to support a multifaceted, family-focused approach to support breastfeeding in AA families because every generation matters to a woman's breastfeeding experience. Data suggest that family feeding history (1-GB, 2-GB, and 3-GB) influenced the content and context of shared infant feeding information within AA families, and provide timely insights into the social support dynamics present within each feeding group. Six themes emerged embodying infant feeding information shared within families: Guidance, Practical assistance, Reservations, Affirmations, Observational learning, and Perceived undermining. Identifying different themes emphasized the value of narratives embedded within grandmother-mother-daughter relationships. Moreover, improved understanding of shared infant feeding information has far-reaching implications for practitioners and researchers who recognize oral tradition as an important mode of transmitting infant feeding information among AAs and understand how it influences infant feeding decision-making. Novel findings include the following: (1) Families used historical aspects of breastfeeding for empowerment; (2) Possible miscommunication occurred within families; and (3) With each additional generation of breastfeeding experience, reporting of Perceived undermining and Reservations decreased.
Historically, AA women's maternal experiences have been negatively affected by practices such as wet-nursing, involuntary breeding, and maternal vilification during chattel slavery and the effects are still ongoing.33–35 Previous studies found this cultural memory and the enduring legacy of slavery and wet-nursing continued to be passed down in AA families and negatively affect their breastfeeding behaviors.35,36 However, this study found that families used this historical knowledge to empower the youngest generation to change the breastfeeding narrative within their family. As a result, these families reclaimed and reconnected with ancestral breastfeeding knowledge and practices, which relates to the BFT tenant of Black women using activism to resist oppression. 26 BFT not only challenges the belief that all women share the same lived experiences, but also examines these differing intersectional experiences of women based on race, class, gender, sexual orientation, religion, nationality, and so on. 26 AA women, in America, share a collective experience of living in a society that systematically oppresses them.34,35 Future studies should use BFT to investigate other cultural knowledge AA women use for empowerment.
All families reported positive infant feeding information shared between generations, yet, the youngest generation reported a negative component—Perceived undermining. Therefore, miscommunication may have occurred between generations; when referencing the same situations, older generations reported expressing reservations, while the youngest generation perceived undermining. For instance, older generations reported worrying about the youngest generation's ability to work and breastfeed, have a backup plan and the necessity to pump breast milk. However, the youngest generation reported hearing, “You're crazy if you think you can work and breastfeed,” “More power to you, you probably won't make it anyway” and “Give that baby the bottle” when the baby is whiny or if the youngest generation “needed” to cover up. Older generations may have been unaware that their words mattered to the youngest generation and may not have intentionally tried to sabotage the youngest generation's breastfeeding practices. They may have unknowingly sent messages to the youngest generation, particularly those who may have been more vulnerable due to being the first generation in their family to breastfeed in multiple generations. The oldest and middle generation, especially those in 1-GB and 2-GB families, may have expressed reservations as a way of passing along anticipatory fears about breastfeeding. People behave avoidantly because of expected fear and anticipatory fear influences avoidance behavior.37,38 Those who work with families (e.g., physicians, lactation consultants, nurses, WIC counselors) should leverage the positive communication between these generations of women while also finding where the touch points are to help these families learn how to curb the perception of undermining.
We acknowledge the unequal-sized feeding groups and that no oldest generation participants were interviewed in 3-GB families, but it is worth noting that perceived undermining (youngest generation's perspective) and reservations (older generation's perspective) decreased with increasing generations of breastfeeding experience. With 3-GB families, neither of the youngest generation reported feelings of undermining from older generations. Although this may not be the lived experiences of all AA families, this finding highlights that grandmothers' experiential knowledge may influence maternal breastfeeding confidence.2,6,21 Considering the influential role AA grandmothers play in infant feeding behaviors, 6 it is wise for clinicians to leverage this influence by including them in infant feeding conversations whenever possible. Face-to-face interactions with grandmothers may not always be possible, due to time, distance, or disability, but engaging them virtually is feasible. 39 As such, practitioners should provide accurate educational breastfeeding information to expel myths or misinformation that either generation may have learned from inaccurate educational channels (e.g., mass media, family members, or friends). In addition, confronting worries—about the practicality of breastfeeding and working, having a feeding back-up plan, and the need to give babies bottles—could serve to dispel fears that older generations may have internalized. Practitioners should explore ways to integrate past family feeding experiences into the assessment of a patient's recorded family medical history to offer tailored breastfeeding support.
This study adds complexity and nuance to lactation literature concerning AA women. Findings suggest areas for assessment that could yield important information about how families communicate infant feeding information. Because infant feeding information was shared (both knowingly and unknowingly) at four reproductive life stages, culturally sensitive breastfeeding interventions should be implemented at different time points to support, promote, and renormalize breastfeeding in AA communities. Within all 15 families, infant feeding information consisted of guidance, practical assistance, reservations, and affirmation, which align with the major subtypes of social support—informational, instrumental, emotional, and appraisal. 40 Although the expression of social support may have been influenced by family feeding history, positive social support existed in all families. Therefore, through an asset-based approach, public health professionals can identify and utilize an AA family's assets (i.e., female family members) as a method of developing solutions for breastfeeding practices.
Limitations
Potential study limitations include issues of generalizability, recall, and social desirability. Participants' geographic location and study sample size preclude generalizability of the conclusions. Therefore, study context was included along with member checking and thick descriptions to describe findings. To limit recall bias, the age of the youngest generation's child was set to younger than 5 years. Finally, the interviewer was from the same racial background as participants and open to listen to each woman's experiences without judgment, thereby minimizing social desirability bias.
Conclusions
Exploring infant feeding information exchanges within AA families emphasize how experiential knowledge, drawn from shared family narratives, provide new insights into the nuanced social support provided. Thus, health care providers who aim to support and promote breastfeeding in this community should be flexible, respectful, supportive, and actively learning about their beliefs and culture, creating space to reframe, without judgment or paternalism.
Footnotes
Authors' Contributions
The authors confirm contribution to the article as follows: study conception and design, data collection, analysis and interpretation of results, and draft article preparation: A.L.W.B. Table and figure design: A.L.W.B., E.J.S., and E.M.M. Critical revisions of the article and approved the final version to be published: A.L.W.B., E.J.S., E.M.M., J.L.S., and S.M.C.
Acknowledgments
This study was based on a doctoral dissertation conducted by the first author. A special thanks to the dissertation committee members at University of South Florida for their contributions to the study. We acknowledge and thank all study participants and the second coder for making this project successful.
Disclosure Statement
No competing financial interests exist.
Funding Information
Funding for the research reported in this article was provided by the University of South Florida.