
Abstract
Purpose:
Exclusive breastfeeding is an integral component of Kangaroo Mother Care (KMC). However, the practice of breastfeeding in KMC position is often suboptimal. Hence, a Quality Improvement (QI) initiative study was conducted to improve breastfeeding rates while providing KMC.
Materials and Methods:
Fish bone analysis was used to identify the potential barriers, which were targeted to bring improvement through Plan–Do–Study–Action (PDSA) cycles. Eligible mother–infant (≥34 weeks) dyad who were admitted in Neonatal intensive care unit during the study period were enrolled in the study (n = 45). QI was implemented through two PDSA cycles. In the first PDSA cycle, training and sensitization of health care providers was done. In the second PDSA cycle, mothers were educated and trained for breastfeeding in the KMC position. Data were collected using bed side nursing charts and interviewing the mothers. Data were analyzed using run charts and SPSS software. A p-value of <0.05 was considered to be significant.
Results:
Percentage of mothers practicing breastfeeding in KMC position increased to 50% after first PDSA cycle and to 100% after the second PDSA cycle from the baseline of <10%. Average duration of KMC increased significantly from baseline 6.09 to 10.9 hours (p = 0.003) in first cycle and 15.6 hours in second cycle (p < 0.001).
Conclusion:
QI measures increased the rates of breastfeeding in KMC position. The total duration of KMC per day was also significantly increased.
Introduction
Kangaroo Mother Care (KMC) refers to the practice of providing continuous skin-to-skin contact between mother and baby, exclusive breastfeeding, and early discharge from hospital. 1 KMC is an evidence-based cost-effective standard of care to reduce morbidity and mortality in stable low-birth-weight (LBW) infants. It improves maternal–infant bonding, promotes breastfeeding and growth, prevents hypothermia, reduces infection, thereby reducing the length of hospital stay and mortality in LBW infants.2,3
Breastfeeding is the integral component of KMC. The best nutrition in preterm LBW infants is mother's only milk. However, achieving successful breastfeeding is always a challenge in this population.
It is a common observation that KMC is interrupted frequently as the infants are taken out of the KMC for feeding with wati spoon or breastfeeding. This reduces the total duration of KMC. To ensure maximum possible skin-to-skin contact, babies should be breastfed in KMC position itself. A knowledge, attitude, and practice study on KMC done in our institute involving 59 mother–infant dyad showed that although nearly three fourth of mothers (38/59) had high overall knowledge and attitude (45/59) about KMC, 91.5% of the mothers lacked the knowledge that exclusive breastfeeding is a component of KMC. The study revealed that although 88% of mothers provided continuous skin-to-skin contact for 8–12 hours per day, only 6.8% (4/59) mothers were practicing breastfeeding in KMC position. 4 Another study similarly revealed that in spite of having knowledge regarding KMC, over one third of the mothers found it challenging and uncomfortable to feed their babies during KMC. 5 These studies point out the need to train and educate the mothers to breastfeed the infants in KMC position. Hence, we contemplated the need to provide supportive environment, targeted training, and counseling of mothers to breastfeed while providing KMC.
Quality Improvement (QI) initiative studies are one of the best tools available for knowledge translation that is, closing the knowledge–practice gap. Various QI studies done on KMC have shown to be effective in improving the KMC practices. 6 The Government of India has also introduced various initiatives to improve the quality of care in neonatal intensive care unit (NICU). 7 QI initiative consists of systemic and continuous action that leads to measurable improvement in health care services and health status of targeted patient group. 8 Hence, we planned a QI study to improve the breastfeeding rates in KMC position.
Materials and Methods
The aim of the study was to improve the rate of breastfeeding in KMC position from <10% to more than 50% in preterm infant with postmenstrual age ≥34 weeks within 8 weeks. Secondary aim was to observe the average duration of KMC practice before and after stepwise introduction of QI.
The study was conducted in a level IIIB NICU of a tertiary care hospital. Mother–infant dyad with KMC recipient with postmenstrual age gestational age ≥34 weeks admitted in the Transitional Care Unit during the study period were enrolled in the QI project. The study was done and reported as per the Standards for QUality Improvement Reporting Excellence (SQUIRE) guidelines for reporting the QI studies. Eligible neonates admitted during the month of October 2018 formed baseline cohort; those during November and December 2018 formed implementation cohort; and those admitted in January 2019 to March 2019 formed postintervention cohort. Sick neonates on assisted ventilation, neonates with major congenital anomalies, or neonates whose mothers were not available were excluded. The study was approved by the Institutional Review Board of our institute and informed written consent was obtained from mothers of each enrolled neonate.
According to POCQI (Point of Care Quality Improvement) module, a QI team (a team leader, one supervisor, an analyzer, a communicator, and two nursing staffs), including two faculty members was formed. 9
Baseline phase and root cause analysis
Two members of the QI team were commissioned as observer to note the breastfeeding practices in KMC. The doctors and the nursing staffs involved in management received no feedback about the same during collection of baseline rate. The QI team collected the baseline data on factors affecting breastfeeding in KMC position over a period of 4 weeks. The data were collected by interviewing mothers as per predesigned proforma and the bedside patient monitoring chart. Root cause analysis was done using the Fish Bone Analysis method (Fig. 1). The barriers encountered by health care professionals (HCP) while promoting breastfeeding in KMC position were analyzed using focused group discussions and brainstorming sessions.
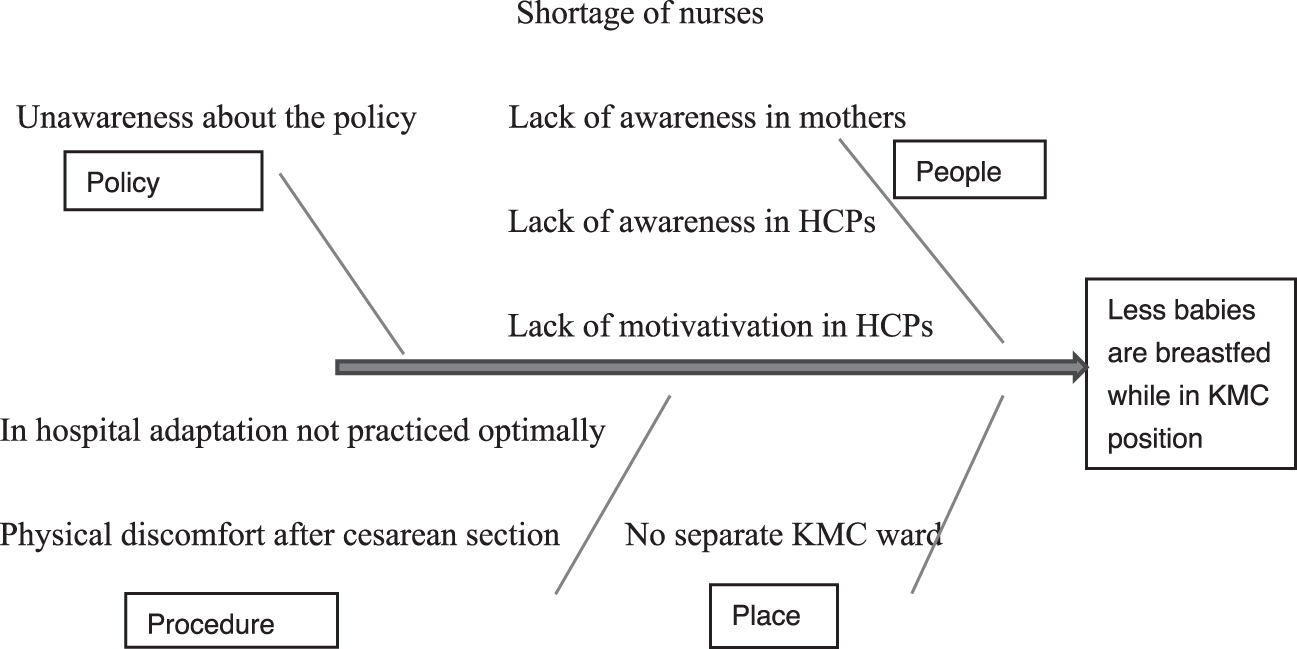
Fish bone analysis. KMC, Kangaroo Mother Care; HCP, health care professionals.
Implementation phase
Depending upon the results of baseline data, we planned two Plan–Do–Study–Action (PDSA) cycles of 4 weeks each.
During first PDSA cycle all HCP, including nursing staff and doctors were counseled, trained, and motivated to support mothers for breastfeeding in KMC position. We emphasized the benefits of KMC, breastfeeding, and why and how to practice breastfeeding while in the KMC position. Various teaching methods used were audiovisual presentations, posters, pictures, and role play. Training was performed in different timed sessions so that all HCPs working in different shifts were trained every week. HCPs were educated in multiple sessions to reinforce the training. Combined meeting of team members and HCPs was held every week during the implementation phase, and mutual interactive sessions were conducted to identify ongoing issues. Implementation of intervention was studied every week and changes were made in the training program as required and feedback was given to all HCPs.
During second PDSA cycle, mothers were counseled, trained, and motivated to practice breastfeeding in KMC position. Mothers were counseled and trained individually about breastfeeding in KMC position by the team members through one-to-one interactive counseling sessions at in-hospital adaptation sessions of KMC. Mothers were educated through lectures in their local language and also through posters, photographs, role play, and practical demonstration. HCPs were continuously encouraged to provide support to mothers. Special timed hour was allotted every day for counseling and training of mothers. In addition, resident doctors and staff nurses on duty trained and retrained the mothers on daily basis as a group activity. To emphasize the importance of breastfeeding in KMC, records were made in the patient-monitoring chart, which included breastfeeding in KMC position as a separate heading. Mothers who were successful in learning the art and technique of providing breastfeeding in KMC were identified by the team members. They were also involved to interact and support other eligible mothers for breastfeeding in the KMC position. Implementation of intervention was studied every week. During the initial 2 weeks, the breastfeeding rate in KMC remained static. So, in the subsequent weeks, four nursing staffs working in the NICU in different shifts were identified as KMC facilitator and were involved in helping mothers for breastfeeding in the KMC position.
Outcome measures
The percentage of eligible mothers who were able to breastfeed their babies in KMC position were selected as the primary outcome measure. The secondary outcome was total duration of KMC before and after stepwise QI introduction. Our unit practices three hourly feeding routine for infants, which makes eight feeds per day. In our unit, fathers practice kangaroo father care during the night hours. So out of the 8 feeds, two feeding times during kangaroo father care were not considered for data collection. Hence, we considered successful intervention if the infant received breastfeeding in KMC four out of remaining six feeds (>60%) on fifth day of enrolment in the study. The initial 2 days of each cycle were kept for any changes in intervention as per need. We assumed that the mothers could be trained after two to three sessions of counseling; hence we selected the data on day 5 for statistical analysis.
Data analysis
Data were collected using predesigned proforma. Data were collected from the day of enrolment until the day of discharge. Analysis was done using run chart using windows XL. Statistical analysis was done by using SPSS for Windows version 16 software. Chi square test was done to compare basic details of participant in baseline and implementation phase, p-value was used as a test of significance. A p-value of <0.05 was considered to be significant.
Results
A total of 45 patients were enrolled (15 in baseline phase, 30 in implementation phase) in this study. The demographic characteristics of enrolled mother–infant dyad were similar in baseline and intervention phase (Table 1). During baseline phase, the rate of breastfeeding in KMC position was found to be 6.6%.
Demographic Data of Study Population
SD, standard deviation.
First PDSA cycle
The rate of breastfeeding in KMC increased to 50% at the end of first PDSA cycle. The average duration of KMC increased from 6.06 to 10.2 hours (p = 0.003).
Second PDSA cycle
The breastfeeding rate in KMC increased to 100% at the end of second PDSA cycle (Fig. 2). The average duration of KMC increased to 14.6 hours (p < 0.001) (Fig. 3).

Run chart depicting the percentage of mothers breastfeeding while employing KMC during each study phase.

Bar diagram depicting average duration of KMC. KMC, Kangaroo Mother Care.
The run chart showed increase in the breastfeeding rate in KMC to 50% at the end of the first cycle and to 100% at the end of the second PDSA cycle (Fig. 2).
Discussion
This QI study has tried to improve the breastfeeding rates during KMC as well as the total duration of KMC. To our knowledge, this is the first study which has tried to improve the breastfeeding rates in KMC position. By targeting breastfeeding in KMC, we could find that both breastfeeding and KMC practices were improved. This may have future implications in growth and development in a preterm infant as we know KMC has various long-term benefits.
The lack of knowledge of mothers, inadequate support received by mothers for feeding in KMC position and absence of formal counseling on feeding practice in KMC position by health care team were the important barriers identified. One-to-one discussion with HCP revealed lack of knowledge and motivation among them. Other factors affecting breastfeeding in KMC were shortage of nurses and discomfort to mothers on prolonged sitting after cesarean section. The results in our study showed improvement in the practice of breastfeeding in KMC after implementing training of HCPs and mothers by the QI team members.
Ideal KMC practices can be scaled up by increasing staff support and implementing temporary project staff. However, the effect may be transient and decreases with withdrawal of support. A unique effort in our study was the utilization of existing resources for strengthening breastfeeding practices during KMC. Audit-and-feedback is considered as one of the backbones of QI initiative for changing health worker behavior as well as an ongoing policy, which formed an important milestone in our study.
Joshi et al. conducted a QI project to increase the total duration of KMC. They showed that by simple QI measures, the duration of KMC increased from average of 3–6 hours in the postimplementation phase. 6 Another QI initiative study done by Sethi et al. showed that introduction of comprehensive postnatal breastfeeding counseling (CPNC) through QI package improved the proportion of neonates receiving mother's own milk from the baseline of 12.5–80% on day 7 of implementation of CPNC. 10
One of the limitations of the present study was that it was not multicentric. The data on continuation of breastfeeding in KMC after discharge for each baby was not prospectively collected, and this was another limitation.
Breastfeeding in KMC is a standard care practice. Our study showed that by training and education, it is possible to improve this with existing staff support. This finding can be generalized to other set up caring for LBW babies.
Conclusion
We demonstrated feasibility of a simple QI approach for increasing breastfeeding rates in KMC position.
What Is Already Known?
Exclusive breastfeeding is an integral component of KMC. However, the practice of breastfeeding in KMC position is suboptimal.
What This Study Adds?
A QI initiative of training and education of HCPs and mothers have potential to improve breastfeeding rates in KMC position.
Footnotes
Authors' Contributions
N.M.: preparation of article and execution of study, data collection, and analysis. R.N.: study design and supervision and critical review of article. S.D.: critically reviewed the article and statistical analysis.
Disclosure Statement
The authors have no conflicts of interest relevant to this article to disclose.
Funding Information
No external funding was procured for this research.