
Abstract
Objective:
This study examined the effect of postpartum administration of depo medroxyprogesterone acetate (DMPA) on milk production, time to onset of secretory activation, lactation duration, and infant consumption of mother's own milk (MOM) in mothers of preterm very low-birth-weight (VLBW) infants.
Materials and Methods:
We conducted a secondary analysis of data from mothers who delivered infants weighing ≤1,500 g and at ≤32 weeks' gestation. The volume of milk produced was measured on days 1–7, 14, and 21 by weighing all expressed milk on an electronic scale. Time to secretory activation was determined through self-report of a feeling of breast fullness. Information on lactation duration and the percent of feeds consisting of MOM consumed by infants was obtained from the medical records.
Results:
Mothers who received postpartum DMPA were more likely to be African American (72.4% versus 31.4%; p = 0.0006), unemployed (65.5% versus 44.5%; p = 0.027), and Medicaid eligible (89.7% versus 67.2%; p = 0.019). There were no differences in daily milk production between mothers who received DMPA before hospital discharge (n = 29) compared with those who did not (n = 141). When mothers who reached secretory activation before receiving DMPA were removed from analysis, receiving DMPA was associated with a later onset of secretory activation (103.7 versus 88.6 hours; p = 0.028). There were no statistically significant differences between the study groups in lactation duration or infant MOM consumption.
Conclusions:
DMPA, when administered postpartum to mothers of preterm VLBW infants, delayed secretory activation, but had no detrimental effect on milk production or lactation duration. Clinical Trial Registration: ClinicalTrials.gov Identifier: NCT01892085.
Introduction
Providing mother's own milk (MOM) to very low-birth-weight (VLBW) preterm infants reduces the risk of prematurity-related complications.1,2 Unfortunately, mothers delivering prematurely often produce insufficient volumes of MOM, have delayed secretory activation, and experience a shorter lactation duration.3,4 When adequate MOM is not available, infants are often fed formula or donor human milk, and while donor human milk is far superior to formula, neither provides the unique components essential for optimal infant health found in MOM.5,6 Therefore, preservation of MOM supply is essential in this vulnerable population of women.
Because short intervals between pregnancies increase the risk of maternal morbidity and mortality, as well as preterm birth, infant mortality, and neonatal intensive care unit (NICU) admission, effective contraception beginning soon after delivery is essential. 7 Depo medroxyprogesterone acetate (DMPA) is a synthetic progestin-only contraceptive that is injected every 3 months to suppress ovulation. 8 Due to the negative health consequences associated with short intervals between pregnancies, potential barriers to postpartum follow-up, and sexual activity in the first few weeks after delivery, DMPA is often administered before the mother's discharge from the hospital.9,10
A decrease in progesterone following delivery is necessary for both secretory activation (transition of production of small amounts of colostrum to copious amounts of milk) and the increased prolactin levels required for establishment of lactation. 11 It is possible therefore that providing progestin-only contraceptives to mothers in the postpartum period may decrease lactation success.12,13 Because mothers of preterm VLBW infants are at high risk for lactation difficulties—including decreased milk production, delayed secretory activation, and a shorter lactation duration—the potential negative effect of DMPA on lactation success is particularly concerning.3,4 While small studies suggest that postpartum administration of progestin-only contraceptives does not negatively affect time to secretory activation or breastfeeding duration, these studies did not include mothers of preterm VLBW infants who must use a breast pump to obtain milk for their infants.14–16 Because MOM is vital for the health of these vulnerable infants and their mothers often produce insufficient amounts of milk, more research is needed to understand the consequences of prescribing progestin-only contraceptives in the postpartum period. Therefore, the objective of this secondary analysis of data was to examine the effect of postpartum DMPA administration (before hospital discharge) on lactation success among mothers of preterm VLBW infants. Specifically, we evaluated milk production during the first 3 weeks following delivery, time to onset of secretory activation, lactation duration, and infant consumption of MOM.
Materials and Methods
This was a secondary analysis of data from a randomized controlled trial funded by the National Institute of Nursing Research. Conducted between November 2013 and August 2016, the study's primary objective was to determine the optimal time to initiate MOM expression in mothers of VLBW infants to enhance lactation success. Mothers who delivered an infant at ≤32 weeks' gestation with birth weight ≤1,500 g were recruited from a baby-friendly designated obstetrical unit in an academic tertiary care center, which is a referral hospital with a catchment area for predominately rural and semirural populations. The obstetric unit is associated with a 72-bed level four NICU.
Subjects were excluded if they were under 18 years old, had no intention to provide MOM to their infant, had documented illicit drug use, were human immunodeficiency virus positive, or had previous breast reduction or augmentation surgery. Study approval was obtained from the Institutional Review Board at the University of Florida. Mothers were approached in their hospital room before delivery by a member of the research team who explained the study, invited them to participate, and obtained informed consent.
A total of 180 women were enrolled in the study. Ten mothers whose infants died before 6 weeks of age were excluded from the final analysis. Twenty-nine mothers received 150 mg of DMPA before their hospital discharge and 141 did not (Fig. 1). The DMPA group received the DMPA a mean of 50 hours after birth (range: 18–111 hours). Because this was a secondary analysis of an existing dataset, an a priori power calculation was not performed. The total sample size of 170 participants provided 80% power to detect a Cohen's d of 0.6 between groups.
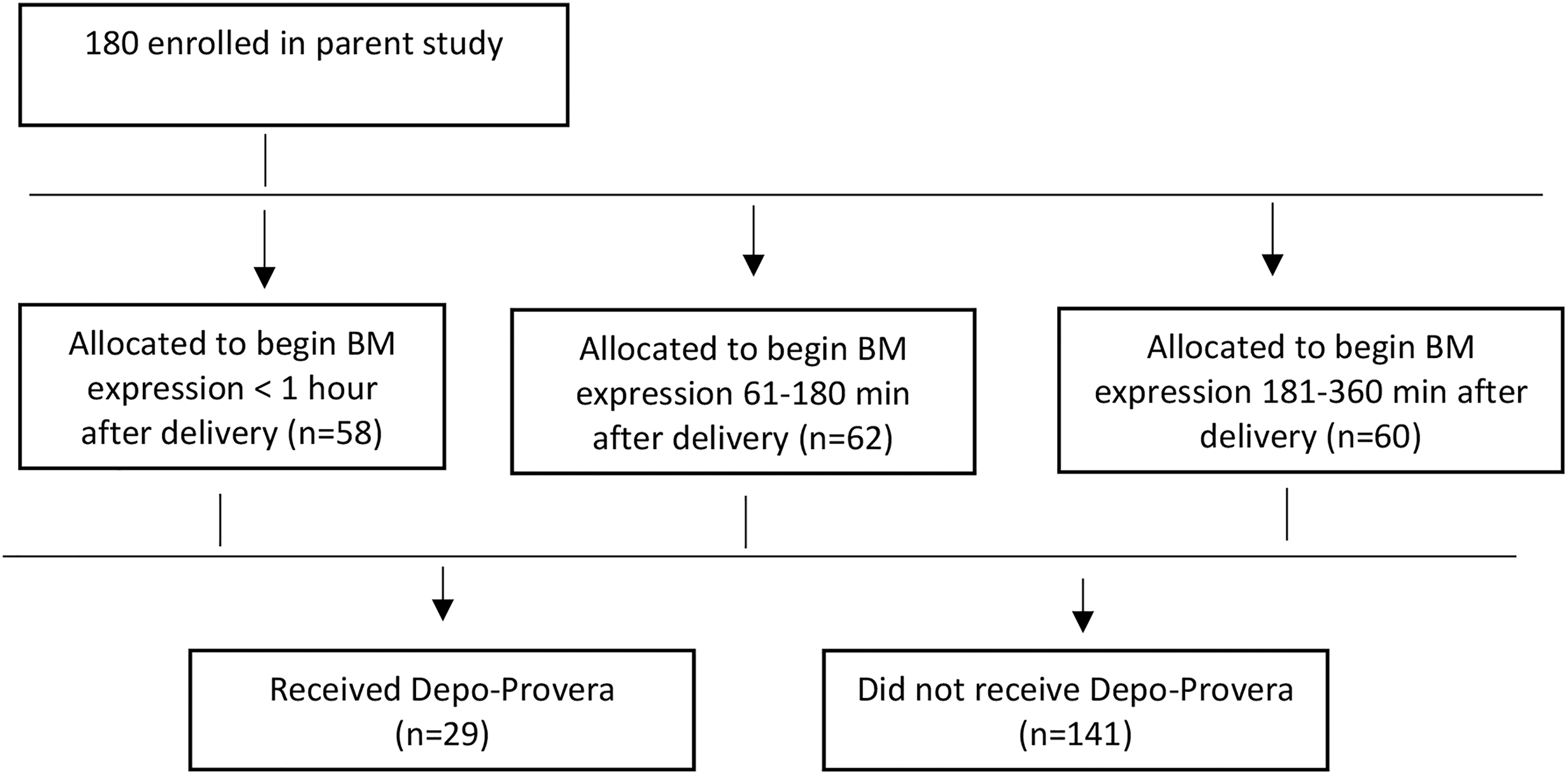
Enrollment diagram.
Study outcomes
Demographics
Information on maternal and infant demographics, episodes of lactation support, and hours of skin-to-skin care was collected from the medical records. Mothers were interviewed by the research team before their hospital discharge regarding when they had made the decision to provide MOM to their infant, and their anticipated lactation duration and lactation experience. Participants completed the Multiple Affect Adjective Checklist–Revised (MAACL-R) before hospital discharge (baseline) and then again on day 21. The MAACL-R is a standardized instrument with well-documented psychometric properties. 17 It uses anxiety, depression, hostility, positive affect, and sensation seeking subscale scores to assess maternal mood. Scores for anxiety, depression, and hostility are combined for a total dysphoric score, while the positive affect and sensation seeking scores are combined for a total positive affect and sensation seeking (PASS) score.
Milk volume
Mothers received standard milk expression instructions provided to all mothers expressing MOM for their infants in the NICU, including on expressing their breasts 8–12 times/day for 15 minutes or for 2 minutes after cessation of milk flow. Mothers were provided a hospital-grade, simultaneous, electric Symphony Plus breast pump (Medela, Inc., McHenry, IL) to use during their hospitalization and for home use while their infant remained in the NICU. Mothers labeled each vial of MOM with the date and time of expression. All vials were brought to the NICU where they were weighed on an electronic digital scale (Scout Balance; Ohaus, Parsippany, NJ) to the nearest 0.1 g by human milk technicians blinded to group assignment. The volume of MOM was measured on days 1–7 and on days 14 and 21. The 3-week study period was chosen because women may receive DMPA beginning 4 weeks after delivery. If an infant breastfed during the 24-hour measurement period, intake was measured by test weighing (weighing infants before and following breastfeeding), an accurate indicator of MOM consumption in preterm infants, and the volume consumed was added to the 24-hour total. 18 The number of times participants expressed milk per day was determined through examination of the date and time of expression sessions marked on the vials of expressed milk by participants.
Time to onset of secretory activation
Beginning 24 hours after delivery, mothers were asked by research coordinators to identify when they experienced a sudden feeling of breast fullness. This is a traditional method of determining secretory activation and correlates with the actual timing of onset.19,20 Mothers were not questioned regarding whether they experienced other potential indicators such as breast tingling or prickling. For mothers who never experienced breast fullness, secretory activation was determined by expression of ≥20 mL of MOM in two consecutive expression sessions. 21
Lactation duration
Research coordinators collected participant data on the number of days from delivery to cessation of lactation. Mothers were determined to have ceased lactation when they (1) stopped bringing vials of expressed milk to the NICU, (2) were not placing their infant to the breast for nutritive or non-nutritive sucking, and (3) stated that they were no longer lactating when questioned by nursing or research staff.
Infant MOM consumption
The percentage of infant feedings that consisted of MOM was obtained from the medical records.
Statistical analysis
All data were analyzed using SAS software (version 9.4, SAS Institute, Inc., Cary, NC). Demographic and clinical features were characterized using appropriate descriptive statistics. The DMPA and non-DMPA study groups were compared using Wilcoxon rank-sum tests for continuous variables and chi-squared tests for categorical variables. The milk volume at days 1–7, 14, and 21, adjusted for gestational age, number of expression sessions, maternal race, being employed (yes/no), and being on Medicaid (yes/no), was compared (individually) between the groups using a general linear model approach. Because the milk volume is often zero for mothers of VLBW infants and thus data contain a disproportionate number of zeros, violating assumptions of normal distribution, longitudinal, marginalized two-part models were used to further investigate the relationship of milk volume with DMPA use. 22 Marginalized two-part (MTP) models were adjusted as described above. Due to the exploratory nature of this analysis, results were not adjusted for multiple comparisons.
Results
The mean age of the mothers was 26.9 years. Almost 50% (n = 81) were White; 60% (n = 103) were single; 51% (n = 86) were employed; and 51% (n = 86) were primiparous. Fifteen mothers in the non-DMPA group had a prescription written for a progestin-only oral contraceptive to begin following hospital discharge. There was a significant difference between women who received DMPA and those who did not in terms of self-identified race. Among mothers who received DMPA, 72.4% (n = 21) were African American, while among women who did not receive it, only 31.4% (n = 43) were African American (p = 0.0006). Mothers who received DMPA were also more likely to be unemployed (p = 0.027) and Medicaid eligible (p = 0.019) (Table 1). There were no differences in lactation factors or maternal mood between groups. However, mothers who did not receive DMPA expressed milk more frequently on day 14, were more likely to receive a lactation consult, and engaged in more skin-to-skin care (Table 2).
Demographic and Clinical Features by Group (Received Depo Medroxyprogesterone Acetate Versus Did Not Receive Depo Medroxyprogesterone Acetate Before Hospital Discharge)
Data are represented as mean ± SD for continuous variables and number (%) for categorical variables.
Discrepancies in frequencies due to missing data for some participants.
p-Value obtained from the Wilcoxon rank-sum test or chi-squared test.
DMPA, depo medroxyprogesterone acetate; SD, standard deviation.
Lactation Factors and Maternal Mood by Group (Received Depo Medroxyprogesterone Acetate Versus Did Not Receive Depo Medroxyprogesterone Acetate Before Hospital Discharge)
Data are represented as mean ± SD for continuous variables and number (%) for categorical variables.
Discrepancies in frequencies due to missing data for some participants.
p-Value obtained from the Wilcoxon rank-sum test or chi-squared test.
DMPA, depo medroxyprogesterone acetate; MAACL-R, Multiple Affect Adjective Checklist–Revised; PASS, positive affect and sensation seeking; SD, standard deviation.
Milk volume
There were no differences in daily milk production between groups for the first 7 days after delivery or on day 14 or 21. After controlling for gestational age at birth, number of daily expression sessions, maternal race, employment status, and Medicaid eligibility, the general linear model analysis indicated no differences in milk production at day 1–7, 14, or 21 (Table 3). MTP model results confirmed this lack of difference in milk production between the groups (results not shown).
Least Squares Means (±Standard Errors) with 95% Confidence Intervals from General Linear Models for Outcome Measures by Group (Received Medroxyprogesterone Versus Did Not Receive Medroxyprogesterone Before Hospital Discharge), Adjusted for Gestational Age, Number of Expression Sessions, Maternal Race, Being Employed (Yes/No), Being on Medicaid (Yes/No), and Timing of Initiation of Milk Expression Following Delivery (Randomized Group)
Odds ratio with 95% confidence interval obtained from logistic regression.
DMPA, depo medroxyprogesterone acetate; MOM, mother's own milk.
Time to onset of secretory activation
Data analysis revealed no statistically significant differences between study groups in mean time to secretory activation even after controlling for gestational age, maternal race, employment status, Medicaid eligibility, milk expression frequency, and time to initial expression following delivery. However, when five mothers who reached secretory activation before receiving DMPA were removed from the analysis, mothers who did not receive postpartum DMPA reached secretory activation earlier (88.6 versus 103.7 hours; p = 0.028) (Table 3). Four mothers (one in the DMPA group and three in the non-DMPA group) who reached secretory activation more than 250 hours after delivery were defined as having lactation failure and were not included in the analysis.
Lactation duration and infant MOM consumption
Overall lactation duration did not differ between the DMPA and non-DMPA groups, including whether mothers continued lactating until infant discharge and days of lactation if they ceased lactating before their infant's discharge. Furthermore, there was no difference in the percentage of feeds consisting of MOM consumed by their infants on days 7, 14, and 21 (Table 3).
Discussion
Limited data exist regarding the effect of postpartum DMPA administration (before hospital discharge) on lactation success in mothers delivering preterm VLBW infants. We found that postpartum administration before hospital discharge did not negatively affect milk production in this population. Although we found no previous research investigating the effect of postpartum DMPA injections on measured volume of milk produced, a prospective case–control study of 250 breastfeeding mothers of healthy term infants by Singhal et al. reported that administration of DMPA before hospital discharge did not decrease maternal perceptions of adequate milk production compared with women not using hormonal contraceptives at 6 weeks, 3 months, and 6 months after discharge. 16
While there were no statistically significant differences in lactation duration between groups, those who did not receive postpartum DMPA were more likely to be lactating at infant discharge from the NICU (47.5% versus 37.5%) and lactated longer (38.8 versus 32.3 days), which may be clinically important. Prior research on the effects of postpartum DMPA use on lactation duration has focused exclusively on breastfeeding mothers of term infants and the applicability of findings to mothers of VLBW infants is unclear. 15 Consistent with our results, a 16-week cohort study of 95 women by Hannon et al. found no difference in breastfeeding duration—defined as continuing to provide at least one breastfeeding session per day—or exclusive breastfeeding when DMPA was administered before hospital discharge compared with mothers who received nonhormonal contraceptives. 23 Conversely, an observational study of 117 mothers by Matias et al. found that those who received DMPA within 72 hours of delivery were less likely to be exclusively breastfeeding at 3 months postdischarge compared with those who received DMPA after 72 hours postpartum or who never received it. 24 Finally, an observational study of 183 women found that while postpartum administration of DMPA did not significantly affect whether mothers were breastfeeding at 6 weeks postpartum, those who received DMPA were 14% more likely to have discontinued. 25 However previous research has not included pump-dependent mothers of VLBW infants, women who are at high risk for early lactation cessation.
We found that postpartum DMPA administration delayed onset of secretory activation. Previous research investigating the effect of postpartum administered progestin-only contraception on time to onset of secretory activation did not include only DMPA. No difference in time to onset of secretory activation or lactation failure—defined as onset of secretory activation more than 120 hours following delivery—was found among 69 mothers of term infants allocated into two groups: those who received etonogestrel implants 1–3 days following delivery and those who received it 4–8 weeks postpartum. 26 Similarly, 96 mothers of healthy infants in Uganda randomized to receive a levonorgestrel implant either within 5 days of delivery or 6–8 weeks postpartum exhibited no difference in time to onset of secretory activation. 27 However, the initial doses and systemic absorption of these contraceptives may be different, thus limiting generalizability of study findings. Because delayed secretory activation is common in mothers delivering VLBW infants and may delay feeding initiation or necessitate the use of donor human milk or formula, our finding of a longer time to onset of secretory activation in mothers who received DMPA may be particularly important.
Although regression models were adjusted for these characteristics, statistically significant demographic differences existed between groups, which may have affected results. Women who received DMPA were more likely to be African American, unemployed, and with a lower socioeconomic status. This finding is consistent with previous research reporting racial and socioeconomic disparities surrounding the use of both DMPA and long-acting reversible contraceptives as well as successful lactation.28–31 Due to a higher risk of unintended pregnancies in these population groups, health care providers may be more likely to offer DMPA before hospital discharge28,32,33 even though women may not originally plan to use this form of contraception. 34 Women who received DMPA were also less likely to receive a lactation consult and participated in less skin-to-skin care, which may have affected results.35,36 Furthermore, while not statistically significant, they also expressed milk less frequently, which may be particularly important because expression frequency is known to affect milk production in mothers of VLBW infants. 37 In addition, previous research suggests that expression frequency is a significant mediator for differences in lactation success between African American and Caucasian mothers. 38 It is possible that these racial and socioeconomic disparities could be, at least in part, due to institutional racism and further investigation is needed.
Individualized and patient-focused contraception counseling, which acknowledges each woman's unique life circumstances and personal wishes, should begin antenatally whenever possible. 39 This allows mothers and their partners sufficient time to consider their postpartum contraceptive options. Waiting to provide contraceptive counseling until after delivery can be problematic, especially for mothers delivering a VLBW infant who requires admission to the NICU when physical and emotional stress may limit their ability to make informed decisions. 40
While our results do not indicate that postpartum administration of DMPA negatively affects overall milk production in women delivering VLBW infants, neither group achieved the minimum volume of milk production by 14 days, which could predict lactation success, nor did they express milk the recommended 8–12 times per day. 41 It is possible that postpartum administration of DMPA could have a different effect in women at less risk of lactation difficulties. Furthermore, it is possible that individual mothers may experience decreased milk production after receiving DMPA, which may be important to mothers providing milk for their premature infant and who, given the choice, may prioritize sufficient milk production over contraception. 42
Study limitations
This study had several limitations. We did not follow participants after 3 weeks postpartum, thus the potential effect of DMPA on milk production beyond this point is unknown. In addition, we used maternal self-report of secretory activation. While this measure is reliable for mothers of term infants, it has not been studied in mothers delivering preterm. This was a secondary analysis of data and thus the sample size was small, original data were not collected to address the study aims, and there was lack of randomization and a priori power analysis. Moreover, excluding women who reached secretory activation before DMPA administration may have selected for women with delayed secretory activation among the DMPA group. Finally, 15 women in the non-DMPA group had a prescription written for progestin-only contraceptives, and while it is unknown whether these prescriptions were filled or whether they used the oral contraceptives, had they not experienced secretory activation before hospital discharge, this may have affected study results.
Conclusions
Establishment of lactation depends upon a decrease in progesterone occurring immediately postpartum. It is thus biologically plausible that providing an exogenous source of progestin could negatively affect this process. This study found that postpartum DMPA administration (before hospital discharge) was associated with a later onset of secretory activation, but did not negatively affect milk production or lactation duration in mothers of VLBW infants. However, it should be noted that this was an exploratory study and further investigation, including an adequately powered randomized trial comparing women who initiate DMPA postpartum with those who initiate 6 weeks following delivery, is needed to provide more definitive results regarding the potential effect of postpartum DMPA on lactation success in mothers delivering preterm VLBW infants and to determine the best timing for administration.
Footnotes
Authors' Contributions
L.A.P. made substantial contributions to the conception, design, and interpretation of data; drafted the original version and revised it critically; provided final approval of the final version; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. S.S. made substantial contributions to the conception, design, and interpretation of data; critically revised the manuscript; provided final approval of the final version; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. N.C. made substantial contributions to the conception, design, and interpretation of data; critically revised the manuscript; provided final approval of the final version; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. C.K. made substantial contributions to the conception, design, and interpretation of data; critically revised the manuscript; provided final approval of the final version; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. M.M. made substantial contributions to the design, analysis, and interpretation of data; critically revised the manuscript; provided final approval of the final version; and agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Disclaimer
The sponsor had no role in the study design; collection, analysis, or interpretation of data; writing of the report; or the decision to submit the report for publication.
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by a grant, 1 R15 NR013566-01A1, from the National Institute of Nursing Research.