
Abstract
Background:
Pasteurized donor human milk (PDHM) supplementation for healthy infants is an emerging practice. Little is known about demographics or breastfeeding outcomes for dyads whose mothers choose PDHM versus formula.
Research Aims:
To identify relationships between in-hospital supplementation choice and (1) dyad characteristics and breastfeeding intent, and (2) breastfeeding outcomes at 1 month.
Materials and Methods:
This exploratory prospective cohort study surveyed healthy dyads requiring medically indicated supplementation. Participants completed questionnaires including demographics, breastfeeding intent, and self-efficacy during hospitalization, and self-efficacy and lactation outcomes at 1 month.
Results:
Of 39 participants, 24 (62%) supplemented with formula and 15 (38%) with PDHM. Formula dyads were more likely than PDHM dyads to have a delivery body mass index (BMI) ≥30 kg/m2 (58% versus 20%, p = 0.02), and less likely to have attained greater than a college degree (33% versus 7%, p = 0.02); formula dyads also reported lower breastfeeding intent scores (12.0 versus 15.5, p = 0.002). Breastfeeding self-efficacy scores were similar but decreased for both groups over 1 month. At 1 month, mothers who chose formula were more likely to continue to provide breast milk to their infants (84% versus 72%). Direct breastfeeding rates were similar (72% versus 68%); of participants directly breastfeeding at 1 month, PDHM dyads were 1.5 times more likely to provide maternal expressed milk.
Conclusions:
Differences in maternal education, BMI, and breastfeeding intent were found between feeding groups. Results suggest an association between PDHM choice and initial breastfeeding intent and breastfeeding self-efficacy and provision of maternal expressed milk at 1 month.
Introduction
Human milk feeding is considered the optimal source of nutrition for healthy growth and development during early life. The American Academy of Pediatrics (AAP), The United Nations International Children's Emergency Fund, and the World Health Organization (WHO) all recommend that infants are fed only human milk for the first 6 months and then breastfed in conjunction with complementary foods through 1 to 2 years of age.1,2 The WHO Baby-Friendly Hospital Initiative (BFHI) promotes the Ten Steps to Successful Breastfeeding to ensure hospital staff provide evidence-based breastfeeding support. 3 Finally, exclusive human milk feeding is one of the Perinatal Core Measures on which hospitals are assessed. 4
Despite bedside support of the maternal–infant dyad from registered nurses, physicians, and International Board Certified Lactation Consultants (IBCLCs), difficulties initiating breastfeeding in the hospital persist. Although nutritional supplementation may be medically indicated, using formula in this setting may interfere with the establishment of breastfeeding.5–7 The use of pasteurized donor human milk (PDHM) in preterm infants has been associated with improved health outcomes 8 ; yet, little is known about PDHM use in healthy term infants.
PDHM is available as an alternative to formula in the hospital setting when supplementation is medically indicated. Acceptance and use of PDHM continues to increase; the Human Milk Banking Association of North America reports that milk banks provided 7.4 million ounces of PDHM to infants in 2019, one million more ounces than the previous year alone. 9 Although theoretical benefits of using PDHM over formula exist for healthy term infants, data regarding its use or related outcomes in this patient population is scarce. Nonetheless, evidence suggests a rise in the use of PDHM in the general newborn population, including at our own institution.10,11
In this study, we aimed to further our understanding of PDHM use in term mother–infant dyads by assessing differences in dyad demographic factors, infant feeding intent, and breastfeeding self-efficacy associated with in-hospital supplementation type (PDHM versus formula), and whether supplementation type is associated with lactation outcomes at 1 month postpartum. We hypothesized that mothers who opted for PDHM would have higher infant feeding intent scores immediately after birth, higher breastfeeding self-efficacy scores at both birth and 1 month postpartum and would be more likely to provide mother's own milk to their infants at 1 month postpartum.
Materials and Methods
Design
We conducted a prospective, longitudinal cohort study, enrolling participants during the postpartum hospitalization and following up with them at 1 month. During the hospitalization, we collected demographic characteristics, assessed breastfeeding, feeding intent, breastfeeding self-efficacy, and medically indicated nutritional supplementation choice. At 1 month after birth, we assessed breastfeeding outcomes and self-efficacy. This study was approved by the hospital Institutional Review Board (protocol #2016P001843).
Setting
We conducted this study on a 60-bed postpartum unit in a large, academic, urban, tertiary care hospital in the northeastern United States with ∼6,200 annual births. The hospital was on the BFHI pathway for the study duration and achieved designation in January 2019. PDHM has been available to healthy term infants since 2013, with dyads given the option of utilizing either PDHM or formula when the need for medially indicated nutritional supplementation was identified. Although no consent for formula use is required, PDHM requires a physician order after families receive education from a registered nurse or IBCLC and provide written consent. PDHM consent forms were available in both English and Spanish.
Recruitment
This exploratory and observational study relied on convenience sampling to identify and gather responses from participants. A member of the Lactation Support Services team identified and approached 44 eligible dyads who required nutritional supplementation during their hospital stay between December 2016 and October 2017. Of the 44 dyads, 39 (89%) agreed to participate and informed consent was obtained by study staff during their hospital stay when convenient for the participants. Interpreter services were available for all families per standard operating procedures at the hospital and as approved by the IRB.
Sample
The sample comprised dyads whose stated intent upon hospital admission was exclusive breastfeeding. Inclusion criteria were healthy, singleton infants >36 weeks gestation who required nutritional supplementation owing to breastfeeding challenges while in the hospital. Infants <36 weeks at this institution are routinely admitted to the neonatal intensive care unit (NICU). Families intending to feed their infants formula without medical indication and infants admitted to the NICU were excluded from the study.
Data collection
The first questionnaire (Time1) was administered using laptop at the bedside using REDCap™ (Research Electronic Data Capture), an electronic data capture tool for research studies. 12 At this time, the mother's preferred email address for administration of the follow-up questionnaire was obtained. The follow-up questionnaire (Time2) was sent to participants at 1 month postpartum in a unique email link through REDCap. Study staff also collected relevant maternal history and infant feeding data from the electronic medical record.
Measurement
Participants completed a survey with help from medical interpreters if needed during the postpartum hospitalization (Time1) that measured their breastfeeding experience including initiation, duration, supplemental feeding type, feeding route, and breastfeeding support from family and caregivers. Participants also provided relevant socioeconomic information. They completed the Infant Feeding Intention (IFI) scale, a validated five-item Likert scale, which scores degree of maternal initial intention to breastfeed on a scale of 0 (no intent) to 16 (high intent). 13 Standardized Cronbach's alpha results for this population was 0.77, suggesting that the items in the IFI scale have a high internal consistency. An alpha result of 0.82 was calculated when the first question, which asks intent-to-feed formula, was removed, as the participants had already committed to breastfeeding at the time of survey administration. Dennis's validated Breastfeeding Self-Efficacy Scale—Short Form (BFSE-SF), a 14-item Likert scale questionnaire, which determines a mother's perceived ability to carry out breastfeeding, was also administered in-hospital. Scores range from 14 to 70, with higher scores indicating stronger breastfeeding intent. 14 A standardized Cronbach's alpha for this group was calculated at 0.90.
At 1 month postpartum, participants received the second survey through e-mail (Time2). Participants were asked about the timing of lactogenesis II, defined as the onset of copious milk secretion, in addition to infant feeding plan at discharge, breastfeeding supports, and reasons for breastfeeding cessation, if applicable. The second survey contained additional questions for all participants who were still providing maternal milk including current feeding and milk expression practices. The BFSE-SF scale was administered again at 1 month for mothers still providing maternal milk. In this study, breastfeeding was defined as feeding the infant at mother's breast, and supplementing was defined as providing expressed maternal milk, PDHM, or formula through another method of feeding either exclusively or in addition to breastfeeding.
Data analysis
Descriptive statistics of the dyad's demographic and clinical characteristics were calculated for the overall sample and by supplementation type. Differences by supplementation type were tested using χ 2 tests for categorical variables, nonparametric Wilcoxon sign-rank for continuous variables. For analyses of categorical variables with cell sizes <5, Fisher's exact test was used. We performed similar descriptive statistics using the study variables and the breastfeeding outcome data (i.e., breastfeeding decision-making, IFI, BFSE-SF survey summary scores, and the change in BFSE-SF score over time [Time2−Time1]). Analyses were repeated in the 1-month follow-up sample to assess demographic differences with the original, total sample. All analyses were performed using SAS software v9.4 (SAS Institute, Inc., Cary, NC).
Results
Maternal–infant factors and supplementation type
Of 39 dyads who participated in our study, 15 (39%) supplemented with PDHM and 24 (62%) supplemented with formula during hospitalization (Table 1). Overall, infants were early term gestation, with appropriate weights for gestational age and equally distributed modes of delivery. No significant clinical differences were found between the two infant groups. Maternal participants were largely married, Caucasian, had an educational attainment above a college degree, and were evenly distributed between primiparous and multiparous women. The median maternal BMI was in the overweight category of 25.0–29.9. Demographics were similar by supplementation type with the exceptions that mothers who chose PDHM were significantly less likely to be obese (20% versus 58%, p = 0.02) and more likely to have educational attainment above a college degree (67% versus 33%, p < 0.02) than mothers choosing formula.
Demographic and Clinical Characteristics of Mother–Infant Dyads
Supplementation types compared using nonparametric Wilcoxon (continuous variables) or chi-square tests (categorical). Among the categorical variables, for those analyses with cell sizes <5, Fisher's exact was used.
p < 0.05.
BMI, body mass index; GA, gestational age; IQR, interquartile range; SD, standard deviation; WIC, special supplemental nutrition program for women, infants, and children.
Table 2 shows survey responses at Time1 about milk expression initiation while in the hospital, initial breastfeeding success, establishment of full milk supply, plans for returning to work, and breastfeeding goals upon return. No statistically significant differences were identified between groups. The breastfeeding prevalence at the time of the in-hospital questionnaire was 79% overall and were similar between the two groups (PDHM: 80% versus formula: 79%). Most dyads had initiated milk expression at the time of the in-hospital interview (87%), but with greater rates among the PDHM compared with the formula mothers (93% versus 83%). Mothers choosing PDHM were also more likely to have plans to return to work within 1 year compared with mothers opting for formula (93% versus 79%). Among mothers planning to return to work (n = 33, 85%), those choosing PDHM were more likely to plan to continue to breastfeed upon return compared with those who chose formula (100% versus 84%).
Breast Milk Provision Status and Longer-Term Breastfeeding Decision-Making at Time 1 (T1) and Time 2 (T2)
Size of analytic samples reported. N = 39 (total cohort); n = 33 (T2 follow-up sample); n = 26 (T2 follow-up sample breastfeeding and/or providing maternal milk, infants not weaned; only this sample responded to the T2 Breastfeeding Efficacy Scale survey). None of the comparison by supplementation type met statistical significance, p < 0.05.
Statistically significant differences were noted between groups on both the IFI and BFSE-SF scores. Mothers who chose PDHM reported greater breastfeeding self-efficacy as well as intent than mothers who chose formula, with mothers choosing PDHM scoring significantly higher on the IFI scale (15.5 versus 12.0, p = 0.002) as given in Table 3. Median BFSE-SF scores overall were 46 (interquartile range [IQR] = 35–49) in the PDHM group with 41.5 (IQR = 37–49) in the formula group, but this result was not statistically significant.
Breastfeeding Survey (Breastfeeding Self-Efficacy Short Form and Infant Feeding Intent) by Supplementation Type
Size of analytic samples reported. N = 39 (total cohort); n = 33 (T2 follow-up sample); n = 26 (T2 follow-up sample providing maternal milk, infants not weaned; only this sample responded to the T2 BFSE survey). Supplementation types compared using nonparametric Wilcoxon test.
p < 0.05.
BFSE-SF, Breastfeeding Self-Efficacy Scale—Short Form; IQR, interquartile range.
Breastfeeding outcomes and supplementation type
Six dyads (15%) were lost to follow-up at 1 month postpartum; they were largely from the formula group [formula: n = 5 (21%) versus PDHM: n = 1 (7%), p < 0.05]. Compared with the 33 dyads (84.6%) followed-up at 1 month, those lost to follow-up were more likely to participate in the Special Supplemental Nutrition Program for Women, Infants, and Children (WIC) (40% versus 6%, p = 0.08), to be of Hispanic ethnicity (80% versus 9%, p = 0.003), not planning to return to work within 1 year after birth (33% versus 6%, p = 0.12), had not yet initiated milk expression at hospital interview (33% versus 6%, p = 0.11), to be younger than those who returned for follow-up (mean 28.5 [standard deviation (SD) = 5.4] versus 34.4 [SD = 5.1], p = 0.015), as well as of lower median income ($40,000 [IQR = $35,000–$100,000] versus $150,000 [IQR = $100,000–$225,000], p = 0.10), and to have less than a college education (40% versus 18%, p = 0.30). Among those not lost to follow-up (n = 33), the differences between the dyads who chose PDHM versus formula were similar to those observed among the 39 dyads with the exception that those who chose PDHM were more likely Caucasian (86% versus 58%, p = 0.13).
Fourteen dyads who chose PDHM and 19 dyads who chose formula completed the survey at Time2 (93% versus 81%) as given in Figure 1. Among the follow-up respondents, a greater percent of the PDHM dyads had ceased breastfeeding compared with the formula group (29% versus 16%). Despite significantly higher breastfeeding intent scores among dyads who chose PDHM in the subsample (n = 33, 15.5 versus 11.0, Table 3), rates of direct breastfeeding were similar between groups (71% versus 68%) (Fig. 1). Three dyads (15.8%) in the formula group only were exclusively expressing milk but also required formula for supplementation. Almost 30% more dyads in the PDHM groups were expressing maternal milk in conjunction with breastfeeding when compared with the formula group (90% versus 62%). Among these breastfeeding and expressing mothers, three dyads in the PDHM group (33%) and two in the formula group (25%) were also supplementing with formula and one participant (11%) continued to supplement with PDHM without expressing milk at all. One participant in the formula group was exclusively breastfeeding her infant (Fig. 1). Differences in the 1-month outcomes between the supplementation types, while clinically different, were not statistically significant (Table 1).
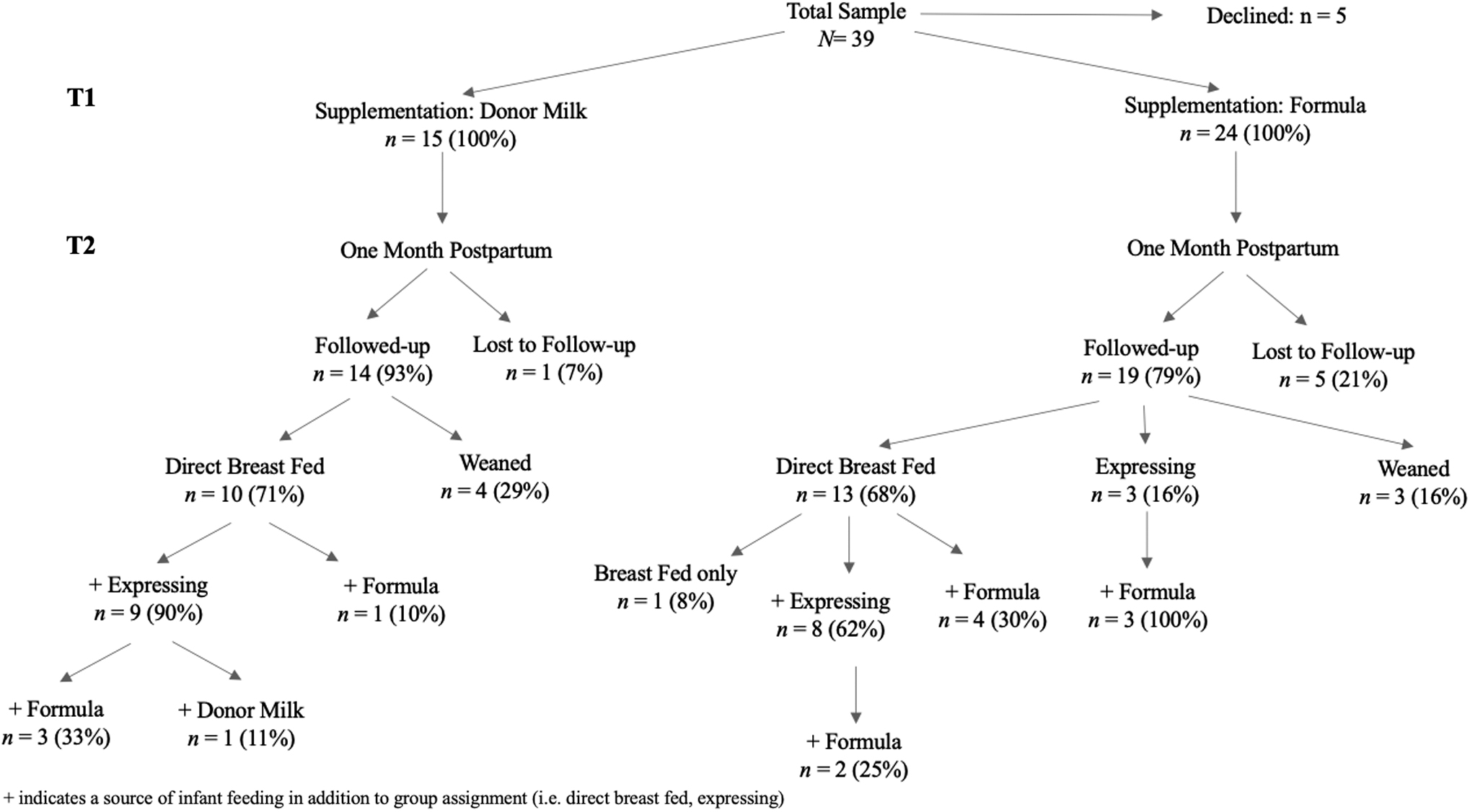
Study flowchart of N = 39 mother–infant dyads by supplementation type followed prospectively from in-hospital postdelivery (T1) to 1-month postpartum (T2).
Overall, BFSE-SF scores decreased between Time1 and Time2 for all respondents who were still providing mother's own milk (42.5–33.5) as given in Figure 2. Greater decreases in scores were observed among the formula (median score change = 7 [IQR = −2 to 11.5]) compared with the PDHM dyads (median score change = 0.5 [IQR = −6 to 8]), but this finding was not statistically significant.
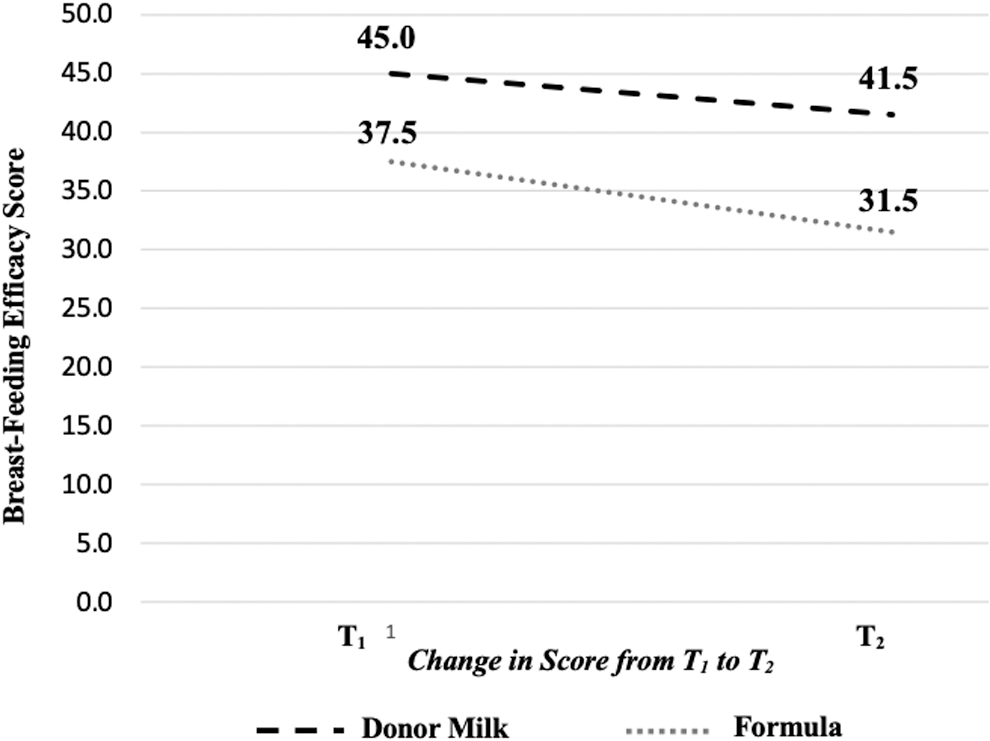
Change in mean scores from the Breastfeeding Self-Efficacy Scale by supplementation type from birth (T1) to 1-month postpartum (T2).
Discussion
In this study, differences in maternal education, BMI, and breastfeeding intent were found between PDHM and formula feeding groups. These results suggest an association between PDHM choice and initial breastfeeding intent measured at delivery. An association was also identified between higher breastfeeding self-efficacy at delivery and provision of maternal expressed milk at 1 month postpartum.
Our first aim was to examine differences in maternal–infant characteristics between supplementation groups. We found that the choice of PDHM for supplementation was associated with greater maternal education attainment. We also discovered that of participants who identified as Hispanic, only one of the seven mothers opted for PDHM. This finding was also identified by Kair et al. who found disparities in PDHM use in the term infant population. 15 They hypothesized that numerous factors, including institutional barriers, lack of access to interpreter services, public insurance coverage, and previous personal or family experience with formula use could impact maternal choice. McKittrick et al. also noted that term infants of English speaking and Caucasian were more likely to receive PDHM supplementation while in the hospital, and considered parental perceptions, approaches in provider counseling, and hospital practices as possible influences. 16 We did not measure patient or provider perceptions or assumptions regarding use of PDHM or formula. Thus, we must acknowledge that families or providers may have bias toward one type of supplementation over another based on the normalized use of formula versus the exploratory use of PDHM, which requires written consent. The finding that PDHM use and accessibility is higher in the Caucasian, English-speaking population in these studies demonstrates an urgent need to examine its role in the continuum of breastfeeding support and feeding outcomes for all families.
Maternal participants who chose PDHM supplementation had a median BMI of 26.6 kg/m2, whereas those who chose formula had a median of 30.4 kg/m2. Elevated BMI can contribute to breastfeeding difficulties including delayed lactogenesis II,17,18 and it is unclear why these mothers were more likely to opt for formula supplementation. The combined risk factors of obesity and delayed lactogenesis II could lead to longer supplementation timeframes and suboptimal breastfeeding outcomes for dyads regardless of supplementation choice. More research is needed to understand provider recommendations and maternal decision-making as it pertains to infant feeding across maternal sociodemographic groups.
Mothers who chose PDHM scored significantly higher on the measure of infant feeding intent than those who opted for formula. The need for nutritional supplementation in the hospital could influence a mother's intent to achieve exclusive breastfeeding when measured in the postpartum period. Utilizing PDHM in the healthy term infant population could provide mothers with more optimism that they can make a bountiful milk supply as demonstrated by milk donors, and qualitative work by Kair and Flaherman and Rabinowitz et al. identified themes of mothers viewing PDHM as “natural,” healthier,” and “temporary”.19,20
Our second aim was to compare 1-month breastfeeding outcomes between groups. Of dyads that supplemented with PDHM, 90% continued to provide breast milk through direct breastfeeding, providing pumped milk, or both directly breastfeeding and expressing milk at 1 month postpartum, as compared with 62% of those who supplemented with formula (see Fig. 1 for other relevant comparisons). Although these differences were not statistically different, the magnitude of the difference may be clinically significant. Direct breastfeeding at 1 month was similar between groups despite higher baseline breastfeeding intent and self-efficacy among PDHM dyads. We speculate that these data may reflect a greater commitment among PDHM dyads to exhaust every option to provide their infants maternal milk, as these mothers were more likely to provide a combination of breastfeeding and expressed maternal milk. Although we identified tendencies in commitment to providing mother's own milk in proportions >10% between follow-up groups, these results were not statistically significant.
Although mothers who are both breastfeeding and expressing milk may cease breastfeeding sooner,21,22 evidence suggests that direct breastfeeding is associated with longer breastfeeding duration. 23 Kair et al. performed a randomized study assigning half their infant participants with weight loss ≥4.5% to supplement with PDHM and compared this group with infants who were not supplemented. 24 They found the use of PDHM had no effect on breastfeeding outcomes through 3 months postpartum. Mannel and Peck retrospectively examined hospital supplementation practices for late preterm infants and found that mothers with the intent to exclusively breastfeed who supplemented with formula were 16% less likely to be providing any human milk at hospital discharge. 25 Merjaneh et al. examined differences in breastfeeding outcomes at 6 months postpartum and found a fivefold increase in likelihood of breastfeeding for infants supplemented with PDHM for medical reasons while in the hospital. 26 The small sample sizes and varied study design are possible reasons for these conflicting results.
Mothers in both groups had a mean lower score on the BFSE from in-hospital report to 1 month postpartum. Of note, only nine participants reported that they sought postdischarge lactation support, and 23 did not identify a single support person (obstetrical or pediatric provider, IBCLC, family, friend, or doula) who assisted them with breastfeeding after discharge. Despite this lack of support and lower self-efficacy, 70% of all respondents at Time2 (n = 33) were still providing maternal milk, demonstrating significant commitment despite facing challenges and lacking support. Dennis found that mothers who were partially breastfeeding (breastfeeding and supplementing with formula) their infants at 4 weeks had lower breastfeeding self-efficacy scores than those exclusively breastfeeding. 14 Our findings were similar. Of note, of the 26 participants who reported that they were still providing maternal milk only one was directly breastfeeding exclusively without any other feeding method reported. The most common reasons for supplementation provided by the 26 respondents were report of low milk supply (n = 9, 35%) and infant appears hungry after feedings (n = 8, 31%). This decline in breastfeeding self-efficacy at Time2 highlights the challenges mothers face in achieving their infant feeding goals and the importance of breastfeeding support after discharge. The lack of lactation care and breastfeeding support after hospital discharge is a known gap in care that many mothers and infants experience, contributing to suboptimal breastfeeding outcomes. Addressing this gap is an important public health priority.
Decision-making around the initiation of a hospital PDHM program for term infants is influenced by a variety of factors, which include increasing breastfeeding exclusivity rates and providing an environment that nurtures and supports breastfeeding mothers. 10 For example, Kair et al. found that hospitals with breastfeeding initiation rates ≥80% and those designated as Baby Friendly are more likely to offer PDHM as a supplementation choice. 27 Despite an enthusiasm for PDHM supplementation to support human milk feeding goals, further study of PDHM use in healthy infants using randomized, controlled study designs and larger sample sizes is needed to detect statistically significant differences. Research on this topic is emerging and demonstrates varied breastfeeding outcomes for dyads supplementing with PDHM. Our findings underscore the need for maternal education on optimal feeding practices among all mothers and effective lactation support both in the hospital and after discharge to improve breastfeeding self-efficacy.
Our study compares breastfeeding outcomes between healthy term mother infant dyads using PDHM and formula during the hospital stay. This is a growing practice worldwide and merits further examination. Owing to the observational nature of this single site study in a hospital with a 97% breastfeeding initiation rate in a highly educated population and the lack of randomization, we cannot eliminate the potential influence of residual confounding and results should be interpreted with caution. The small sample size further limited the ability to control for typical confounders and therefore, effect estimates may be biased.
We found more participants with lower educational attainment, age, income, and breastfeeding intent were lost to follow-up, which further limits the generalizability of our findings. Further study involving multiple study sites and a larger, more diverse sample is warranted to adequately test future research hypotheses on the use of PDHM in the term infant population.
Conclusions
This study found that dyads opting to use PDHM while in the hospital had lower BMI, higher educational attainment, and higher infant feeding intent than dyads who chose formula when nutritional supplementation was required. We observed small, but clinically meaningful, differences by supplementation type of between 10% and 30% in outcome rates. Because of the exploratory nature and limited sample size, we did not find statistically significant associations between in-hospital supplementation type and breastfeeding outcomes at 1 month postpartum. Further investigation is needed to better understand parental decision-making as it relates to nutritional supplementation and the potential influence of using PDHM in healthy infants on breastfeeding outcomes.
Footnotes
Acknowledgments
The authors thank all the families who took the time to participate in this study. The authors also thank Nicolette Overton and Colleen Shelly for their editorial assistance.
Disclosure Statement
No competing financial interests exist. The authors have no financial conflicts of interest to disclose.
Funding Information
All phases of this study were supported by Brigham and Women's Hospital. Ms. Riley and Dr. Gregory were awarded a Karsh Nursing Research Award from Brigham and Women's Hospital to conduct this work.