
Abstract
Background:
Our level III neonatal intensive care unit (NICU) implemented the use of an exclusive human milk diet (EHD) and sought to determine its effect on the severe co-morbidities of preterm infants as well as the potential cost-savings due to the anticipated reduction in these co-morbidities.
Methods:
A retrospective cohort study was completed to determine if an EHD statistically decreased the rate of co-morbidities including length of stay (LOS), days on total parental nutrition (TPN), rates of late onset sepsis, necrotizing enterocolitis (NEC), bronchopulmonary dysplasia (BPD), and severe retinopathy of prematurity (ROP).
Results:
An EHD significantly decreased the odds of severe ROP (adjusted odds-ratio (aOR)=0.349; 95%CI [0.156, 0.739]; p=0.008) and late onset sepsis (aOR=0.323; 95%CI [0.123, 0.768]; p=0.014). Analysis of cost-effectiveness of an EHD relative to a BSD based on the incremental costs of these co-morbidities determined the net loss in direct hospital costs per patient were estimated to be $420 in 2016 US dollars; however, given the long-term health-care costs and non-pecuniary damages from the co-morbidities of severe ROP and sepsis this net loss appears negligible.
Conclusion:
This study found that an EHD significantly decreased the odds of severe ROP and late onset sepsis; though not significant, there was a positive trend in decreasing cases of medical NEC; our surgical NEC rates dropped to 0. The benefits of human milk are vital, and the costs are nominal.
Introduction
In the United States, the rate of preterm births continues to rise. According to the March of Dimes 2019 report card, it increased for the fourth year in a row accounting for 10.02% of all births in 2018. 1 Being born preterm predisposes infants to a host of morbidities and increased mortality.
One way to potentially reduce the likelihood of morbidities occurring in a premature infant is by administering an exclusive human milk diet (EHD) in contrast to a diet that includes bovine-based products (either preterm formula or a bovine-based fortifier added to mother's own milk [MOM]). The American Academy of Pediatrics advises that premature infants should begin receiving MOM when medically able to receive important health benefits.2,3 Evidence suggests that human milk-based diets may reduce the length of stay (LOS), decrease days on total parenteral nutrition (TPN), 4 improve feeding tolerance, 4 decrease rates of retinopathy of prematurity (ROP), and decrease rates of late onset sepsis, 4 necrotizing enterocolitis (NEC),4–8 and bronchopulmonary dysplasia (BPD)7,9 when compared to diets with bovine-based products. Reductions in these health outcomes can lead to decreased health care costs.3,4,6,10
With the widespread increase in the use of donor milk, many units utilize donor milk with bovine-based fortifier to provide the proper nutrition for preterm infants. This has been shown to have negative implications on NEC cases and severe morbidity when compared to a strict human milk-based diet. 11 Therefore, an EHD offers the best protection against comorbidities4,11 but has also been associated with slower growth in all categories (weight, length, and head circumference). 5
The IRB at the University of Missouri Health Care approved this retrospective cohort study, which examined the effects of an EHD (human donor milk or MOM fortified with human donor milk fortifier) on the medical and economic outcomes compared to a non-EHD (either MOM with bovine-based fortifier or bovine-based preterm formula).
Methods
This IRB approved, retrospective cohort study was completed in our level III neonatal intensive care unit (NICU). We compared 53 infants who were born <30 weeks gestation and/or weighed <1,100 g at birth who received an EHD in 2018 per our protocol to 36 infants who were born <30 weeks gestation and/or weighed <1,100 g at birth but received a bovine supplemented diet (BSD) using MOM with bovine-based fortifier or preterm infant formula in 2016. Due to challenges with creating, implementing, and following the 2017 protocol, only those infants who met the stricter 2018 EHD criteria (<30 weeks and/or <1,100 g) were enrolled as the EHD cohort for this study.
Protocol implementation
A multidisciplinary team comprised of nurses, nurse practitioners, lactation consultants, registered dietitians, and physicians created a protocol for the use of donor milk in our level III NICU. Before implementation of the protocol in March 2017, all infants received a bovine based formula for enteral nutrition if maternal breast milk was unavailable. When possible, a bovine-based fortifier was used to supplement MOM. The initiation of enteral feeds and the feeding advancement protocols have remained unchanged both pre- and post-EHD implementation. For very low birth weight infants (VLBW), <1,500 g at birth, trophic enteral feeds (<20 mL/kg/day) were initiated on day of life 1–2 with fortification of milk beginning when enteral feeds reached 80 mL/kg/day. In addition, enteral feeds were increased by 20 mL/kg/day.
Due to budget constraints, the EHD protocol was revised in January 2018 to only allow infants who were born <30 weeks gestation and/or <1,100 g at birth to receive an EHD using Prolacta products for both donor milk and donor milk fortifier added to MOM. Varying calorie contents (24–28 kcal/ounce) were utilized depending on the infant's growth trends. When MOM was available, fortifier was added to increase the calories and the nutritional components required for the preterm population. Those infants placed on an EHD were weaned off all donor milk products 4 weeks after attaining ≥20 mL/kg/day of enteral feeds. This was chosen due to our fiscal responsibility and the fact that at our institution, enteral feeds are included in the total fluid goal after reaching ≥20 mL/kg/day. During and after weaning from donor milk products, infants were placed on MOM with bovine-based fortifier or preterm infant formula.
Study cohort
In 2018, 54 infants were fed an EHD, and in 2016, 37 infants were found to have met the 2018 EHD criteria but received formula or bovine-based fortifier added to MOM (i.e., BSD). Infants who died before 7 days of life were excluded as the comorbidities of interest were indeterminate or unmeasurable in infants less than 7 days of age. Figure 1 illustrates the final sample selection (BSD n = 36, EHD n = 53).
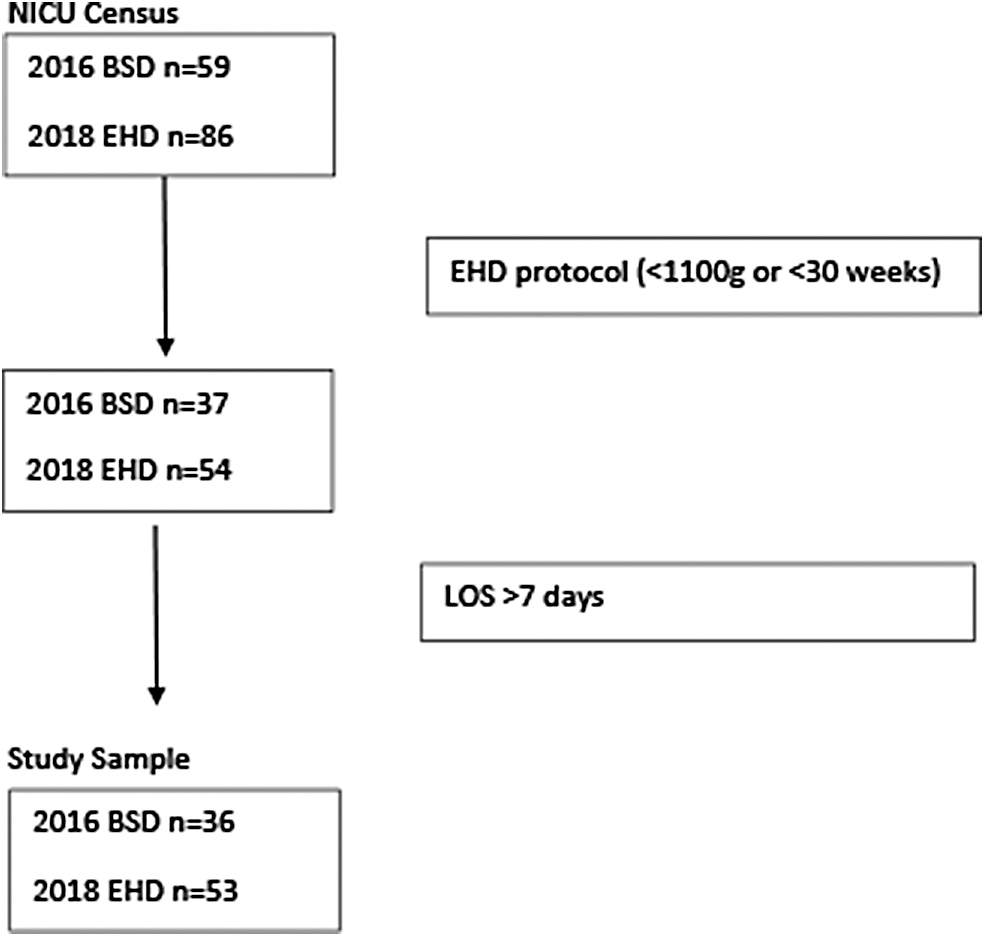
Cohort selection.
Data on comorbidities were collected through chart reviews and cross referenced with the Vermont Oxford Network (VON) database for severe ROP (Stage 3 or greater), late onset sepsis, NEC (medical and surgical), and BPD. The LOS, days on TPN variables, gestational age (GA), birth weight (BW), sex, and race were gathered from the medical charts.
Statistical analysis
Table 1 presents the descriptive statistics of the two cohorts. Patients who died while under observation were included in the analysis where possible, because the primary outcomes of interest were the presentation of severe conditions, which might result in death (BSD n = 1, EHD n = 3).
Patient Characteristics by Diet
p-Values from a one-tailed t-test, and two-sample proportion test.
BSD, bovine supplemented diet; BW, birth weight; EHD, exclusive human milk diet; GA, gestational age.
Due to the unbalanced covariates in our small sample population, presentation of severe conditions (medical NEC [NEC Med], BPD, severe ROP, and late onset sepsis) were assessed using a multiple logistic regression model with milk type (BSD vs. EHD) as the treatment, and adjusted for GA, BW, sex, and race (i.e., African American or Caucasian/Other) using propensity score weighting12,13 Analysis for surgical NEC (NEC Sx) was not performed because not enough cases were observed to provide unbiased estimates, and combining the surgical and medical cases did not meaningfully change the statistical results. A Box-Cox transformed regression models with propensity weights and robust standard errors to account for heteroscedasticity were used for analysis of LOS and TPN days. 14 p-Values are presented for a two-tailed test, and significance was determined with p < 0.05.
Cost effectiveness analysis
Cost savings estimation was based on disease cost estimates for the co morbidities found to be significantly impacted by an EHD. 15 Specifically, the adjusted odds-ratio (aOR) for ROP and sepsis were used to estimate the number of comorbid cases in 36 patients had an EHD been administered instead of a BSD, using the observed rate of cases in 2016. From this estimated case number, the reduction in cases and estimated savings based on the incremental hospital costs were calculated, accounting for the cost of the human donor milk. 15 All costs/savings were adjusted into 2016 U.S. dollars, using the consumer price index provided by U.S. BLS. Sensitivity analysis was performed on the cost adjustment using the consumer price index for medical care [CPIMEDSL] and the producer price index for selected health care industries [PCUASHCASHC]. Cost of the human donor milk and supplement provided in 2018 for 53 patients was adjusted for 36 patients and converted into 2016 dollars.
Results
Statistical analysis
Table 1 presents the mean and standard deviation for quantitative variables, and a percent for binary variables where appropriate. It shows that the two cohorts (BSD in 2016 and EHD in 2018) were statistically similar. The sample cohorts were balanced in terms of race, GA, and BW, but unbalanced in sample size and sex.
Table 2 presents the percentage of our patients who developed any of the comorbidities (NEC Sx, NEC Med, BPD, severe ROP, and late onset sepsis) in our two cohorts. In addition, we determined the mean LOS and the mean number of days on TPN for the two groups and the standard deviations for these variables. Patients who did not survive were not included in the LOS and the days on TPN calculations. p-Values from a one-tailed t-test and two-sample proportion test were calculated comparing the EHD group to the BSD group. We found that those infants fed an EHD had a significant reduction in their rate of severe ROP (p = 0.006), late onset sepsis (p = 0.023), and the number of days on TPN (p = 0.007).
Outcome Measures by Diet
Patients who died are not included in LOS, TPN measurements. p-Values from a one-tailed t-test, and two-sample proportion test.
BPD, bronchopulmonary dysplasia; BSD, bovine supplemented diet; EHD, exclusive human milk diet; LOS, length of stay; NEC Med, medical necrotizing enterocolitis; NEC Sx, surgical necrotizing enterocolitis; ROP, retinopathy of prematurity; TPN, total parenteral nutrition.
Table 3 provides the estimated effect of an EHD relative to a BSD on LOS and TPN days. For LOS, the effect of utilizing an EHD appeared to provide a positive impact compared to a BSD; however, this effect was not statistically significant. For TPN days, an EHD decreased the number of days the infants required TPN compared to those on a BSD; but again, this effect failed to be statistically significant.
Effect of Human Donor Milk Relative to Bovine Milk
Box-Cox transformed dependent variable. Generalized linear model with robust standard errors and adjusted for BW, GA, race, and sex through propensity score weighting. Robust standard errors given in parenthesis.
Logistic model adjusted for BW, GA, race, and sex through propensity score weighting.
Significant at α = 0.05.
aOR, adjusted odds-ratio; BPD, bronchopulmonary dysplasia; BSD, bovine supplemented diet; BW, birth weight; CI, confidence interval; EHD, exclusive human milk diet; GA, gestational age; LOS, length of stay; NEC Med, medical necrotizing enterocolitis; NEC Sx, surgical necrotizing enterocolitis; ROP, retinopathy of prematurity; TPN, total parenteral nutrition.
Table 3 provides the aOR of presentation of a severe condition from an EHD relative to a BSD for the sample, including and excluding deaths. Analysis for surgical NEC was not performed because there were not enough cases; however, we noted a decrease in these cases from 2.78% to 0% as provided in Table 2. For three of the four conditions analyzed (medical NEC, severe ROP, and late onset sepsis), the aOR showed that the EHD was associated with a decreased odds of a severe outcome. For medical NEC, the odds decreased by 6.7% (deaths included); however, the aOR estimates were not statistically significant with p = 0.93 and 95% CI [0.188 to 4.527]. For BPD, the aOR was 1.263 with p = 0.461 and 95% CI [0.679 to 2.363]. For severe ROP, the aOR was 0.349 with p = 0.008 and 95% CI [0.156 to 0.739]. Finally, for late onset sepsis, the aOR was 0.323 with p = 0.014 and 95% CI [0.123 to 0.768].
Cost-effectiveness analysis
The cost savings from providing patients an EHD rather than a BSD are presented in Table 4. Based on the rates of severe ROP and late onset sepsis in the 2016 cohort and the aOR provided in Table 3, we determined the expected number of cases for each condition in 36 patients had they received an EHD instead of a BSD. Based on these calculations, 6.65 fewer cases of severe ROP and 4.96 fewer cases of late onset sepsis would have occurred. The cost associated with these conditions was derived from Black et al., who stratified the cost of morbidities based on the GA at birth. After adjusting to 2016 dollars, the incremental cost of severe ROP was $39,344 for an infant with a GA of 27 weeks, and for sepsis the cost was $17,822. 15 We determined that the net loss of providing an EHD to 36 patients was $420 per patient. Sensitivity analysis of the cost adjustment also revealed the sensitivity of the cost analysis to the inflation adjustment index, with the producer price index for selected health care industries estimating a net loss of $685 per patient and the consumer price index for selected medical care estimating a net savings of $873 per patient.
Cost Savings Analysis from Reduced Morbidity Cases (2016 U.S. Dollars)
All costs/savings are adjusted into 2016 U.S. dollars, using the U.S. Bureau of Labor Statistics Consumer Price Index by Industry [CPIAUCSL], retrieved from FRED, Federal Reserve Bank of St. Louis; https://fred.stlouisfed.org/series/CPIAUCSL, March 5, 2021.
Estimated percent under EHD is calculated from the statistically significant aOR which includes deaths, and the observed percent of cases under BHD.
Incremental cost of hospitalization for ROP severe and sepsis acquired from Black (2015) at $35,749 per ROP case and $16,194 per sepsis case, assuming GA of 27 and 2010 U.S. dollars.
Cost of human donor milk for 53 infants in 2018 was $562,562. This cost was adjusted for 36 patients to 2016 dollars.
aOR, adjusted odds-ratio; BSD, bovine supplemented diet; EHD, exclusive human milk diet; GA, gestational age; ROP, retinopathy of prematurity.
Discussion
Human milk provides nutrition, bioactive compounds, and immune properties.4,7 Due to these benefits, human milk is the preferred nutritional source for patients in NICUs and particularly for VLBW infants who are at greatest risk for complications.4,16,17 Introduction of formula in the first 14 days of life was found to increase the risk of NEC by more than three times. 6 In addition, infants fed an EHD showed improved feeding tolerance demonstrated by fewer held feedings and decreased time to achieve full enteral feeds. 4 Infants who received higher amounts of MOM during the first month of life also had significantly reduced NICU costs. 18
The benefit of using an EHD means the VLBW infant is not exposed to bovine-based products during the first weeks of life. This time period is critical in the development of comorbidities throughout the infant's stay.5,10 Premature infants have immature gut hormones and mucosal barriers.19,20 These factors, coupled with increased activation of inflammatory mediators, cause dysregulation of intestinal microcirculation, predisposing them to NEC and other infections.19,20 In multiple studies, exclusive human milk-based diets have been shown to decrease the occurrence rate and severity of NEC, which have significant effects on clinical and economic outcomes. 21 Unfortunately, we were unable to replicate this finding, likely due to our small sample size and the fact that we only kept our patients on an EHD for about 4 weeks.
Our study includes two analyses on the comorbidities, including and excluding survivors (Table 3), because some comorbidities may have occurred in nonsurvivors had they survived. However, including nonsurvivors is more accurate because for many of the comorbidities, death is an outcome. A significant reduction in the odds of severe ROP by 65.1% was seen in our infants who received an EHD compared to those fed a BSD after adjusting for sex, race, GA, and BW. Although supplemental oxygen is a necessity in NICUs, it can trigger the development of ROP and BPD. ROP has become a leading cause of childhood blindness and vision loss;22,23 while BPD refers to lung damage, often created by necessary ventilator support, causing an oxygen requirement at 36 weeks post menstrual age. Both these comorbidities can be partially attributed to oxidative stress and oxygen-free radicals.22,24 Sufficient nutrition is a key treatment for BPD, 24 while poor nutrition can be a causative factor in ROP. 22 Current research found that the antioxidant and the immune-protective properties of human milk was protective against ROP and BPD.7,22 In addition, we note that the increased observed incidence of BPD may be due to a reduction in mortality. 25
Late onset sepsis continues to be one of the most common morbidities in the VLBW population, driving up cost, and LOS. 10 Due to preterm delivery, the infant's intestinal tract, including the villi and mucosal barriers, is not fully developed, predisposing these infants to infection. 26 After birth, gut colonization is impacted by microbes from the maternal birth canal and colostrum. The microbiome of the gut influences the intestinal barrier and can either help prevent infection or make the infant more susceptible. 26 The administration of human milk allows the infant to receive human milk oligosaccharides, preventing pathogens from binding to the intestines and helping host bifidobacteria, a beneficial organism, fluorish. 26 Human milk transfers secretory IgA to the infant assisting with the immune defense of a neonate, whereby decreasing the risk of sepsis. 26 Our results provide evidence that the administration of an EHD during the first few weeks of life decreased the odds of late onset sepsis by 67.7% compared to those infants fed a BSD. The number of days an infant required TPN decreased but was not statistically significant. This may indicate an improved tolerance to enteral feeds, allowing for appropriate advancement of the feeds, thus reducing the need for TPN.
This study contributes to the economic analysis and cost-effectiveness literature, which has demonstrated cost savings from breastfeeding, 16 MOM, and an EHD. 27 Several cost analysis studies focused on the cost savings of an EHD by examining the hospital and physician charges from surgical and medical NEC and associated LOS. 28 While these studies focused on societal costs, long-term costs, or additional medical costs beyond birth,16,28,29 this study provides an analysis of hospital costs accounting for comorbidities. Providing a probabilistic cost analysis for comorbidities, van Katwyk et al. demonstrated that hospital cost savings from an EHD occurred for infants under 750 g. With a net loss of $420 per patient, this study failed to find cost savings from an EHD that can occur with a more inclusive protocol for infants <1,100 g and/or a GA <30 weeks. However, given the long-term health care costs and nonpecuniary damages of comorbidities for severe ROP and sepsis, this net loss appears negligible.
The long-term financial effect of ROP, including the direct cost of raising a blind child is estimated at $84,586 with indirect costs of $817,996 per child accounting for parental workdays lost due to caring for a blind child through retirement. The impact on society due to the loss of productivity of a blind person is estimated at $357,019 per person; therefore, making the long-term disability costs of ROP up to an estimated $1,259,601 per person. 30 Thankfully, early intervention for infants suffering from ROP can save vision, but the subsequent life-long care, including ophthalmology examination and vision enhancement, is not without significant cost. In addition, the negative cost savings found in this study could easily turn positive if the effects of an EHD on ROP and late onset sepsis are larger than we estimated. For example, Zhou et al. in a meta-analysis found a similar ORs for any stage ROP (OR = 0.29) when comparing an EHD with any formula and a reduction in the odds (OR = 0.11) of severe ROP with an EHD. 22
While no statistical difference between the BSD and the EHD groups was noted for NEC and BPD, other articles have found an effect. Hair et al., and Quigley et al. reported a significant reduction in the likelihood of NEC from an EHD; and Spiegler et al. reported a reduction in BPD, although these studies highlighted the need for much larger sample sizes to determine significance.7,8,14
Throughout the implementation of an EHD in our NICU, the percent of infants discharged on MOM declined, suggesting an unintended consequence that having the option of human donor milk negatively impacted the desire to provide MOM, increasing the overall cost of feeding our infants. According to the Vermont Oxford database, in 2016, 52.6% of VLBW infants in our unit were discharged on some portion of MOM. In 2018, this number decreased to 44.7%. MOM has been shown to be the nutritional source providing the most protection against various comorbidities in the NICU, and it is less expensive than human donor milk.31,32 Staff and specifically lactation support should continue to be an integral part of caring for VLBW infants, through encouragement and support of breastfeeding/pumping. This could potentially lead to a significant cost-savings to the institution and individual families.
Conclusion
This study found that an EHD significantly decreased the odds of severe ROP and late onset sepsis. The benefits of human milk are important and the costs savings exist when considering either the cost of morbidities experienced by VLBW infants, life-long cost of care, and nonpecuniary costs. 33 It should be noted that the decrease in comorbidities and associated costs provide evidence to support the purchasing of an EHD and this can be utilized when negotiating a budget. In our institution, we were able to expand the donor milk program after our analysis described in this article to include all infants ≤1,250 g, and we are now continuing the EHD until they attain 34 weeks gestation. The VLBW population is medically fragile and predisposed to a variety of morbidities which an EHD impacts. Thus, an EHD can truly positively impact the infant's quality of life.
An unexpected outcome we noticed after implementation of the EHD protocol was a drop in the percentage of mothers who were providing breast milk to their babies in our NICU. MOM is the preferred source of nutrition for newborns providing the most protection against various comorbidities in the NICU.31,32 Optimizing NICU specific lactation support in an effort to increase the duration and frequency of the use of MOM should be an ongoing goal. Mothers need prompt and continued access to hospital grade pumps with a goal to be pumping within 1 hour of birth. They should be taught hand expression in conjunction with pumping.2,21 The overall importance and advantage of utilizing MOM over the use of donor milk needs to be touted to our mothers; breast milk is similar to a medication that a mother makes specifically for her child.
Although this article demonstrated several benefits of an EHD, more research is needed to describe the optimal supplementation (fortifier, cream, and sodium) to continue to improve growth promotion in VLBW infants and determine other impacts of an EHD.
Limitations in our project include our small sample size, which is constrained by the retrospective nature of the study and the protocol changes occurring after 2018 for administrative reasons. We note that a large sample size in several studies was required to detect a significant effect. If we had a larger sample size, maybe we would have also seen a significant decrease in more of the comorbidities with an EHD.3,7,8,14
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received.