
Abstract
Background:
Although rates of complementary food and beverage (CFB) consumption among infants under 4 to 6 months of age have been declining, they remain well above the American Academy of Pediatrics (AAPs) recommendations. It is unclear if women with low income in the United States are more likely than other women to introduce CFBs early. We examined timing of introduction of CFBs to infants of mothers with low income to further illuminate infant feeding practices in this potentially vulnerable population.
Materials and Methods:
We analyzed infant feeding data collected prospectively from 443 mother–infant dyads. Data were obtained by interview at 1, 3, and 6 months postpartum. We used Kaplan–Meier curves to show time to introduction of CFBs overall and by type of CFB, and log-rank tests to compare timing by demographic and clinical characteristics.
Results:
Participants were mostly non-Hispanic black or white, with a high school education or less. By month 3, 48% of infants were fed at least one CFB, increasing to over 83% by month 5. Women who did not work outside the home introduced CFBs significantly earlier than those who worked, as did women who smoked compared with those who did not. Timing did not differ by other participant characteristics.
Conclusions:
Introduction of CFBs before 4–6 months was common. Clinical guidance and intervention programs should support mothers toward the goal of improving infant diets in this at-risk population.
Introduction
Infant feeding practices have gained attention in recent years, due to preliminary evidence that introduction of complementary foods and beverages (CFBs) before 4 months of age may be associated with higher risk of obesity and other health issues.1–5 The National Academies of Sciences, Engineering, and Medicine recently released dietary guidelines for the period from birth to 24 months to address the previous lack of attention paid to this important stage of physical development and formation of dietary patterns. 6 For optimal infant nutrition and health, infants should be fed breastmilk exclusively until about 6 months of age, with nutrient-dense foods introduced thereafter. These guidelines align with those of the American Academy of Pediatrics (AAPs), which also recommend introduction of solid foods as developmentally appropriate after about 6 months, delay of cow's milk until 12 months of age, and continued breastfeeding up to 1 year of age or beyond. 7 They also support updated recommendations from the AAP, the Academy of Nutrition and Dietetics, and the American Academy of Pediatric Dentistry that include allowing sips of water from a cup at mealtimes beginning at 6 months and delaying introduction of juice until 12 months. 8
Although rates of CFB consumption among infants under 4 to 6 months of age have been declining, they remain well above AAP recommendations.9–11 Women with low income in the United States may be more likely than other women to introduce CFBs before 4 to 6 months. Although a few previous studies have focused on this population, they have relied on cross-sectional data and/or arrived at conflicting conclusions.10–15 We analyzed prospectively collected infant feeding data to 6 months of age from a population of women with low income to further describe feeding practices in this potentially vulnerable population.
Materials and Methods
During the Prenatal Education Video Study (PEVS), a multisite trial designed to test the efficacy of a breastfeeding educational video, detailed information on infant feeding practices was collected prospectively from birth through 6 months of age. Participants were women eligible for the Supplemental Nutrition Assistance Program for women, infants, and children (WIC); to be eligible for WIC, women must meet nutrition risk and income threshold criteria. 16 Details about the study have been published previously.16–18 In brief, women were recruited during the third trimester of pregnancy in prenatal clinics at two sites; those with multiple-gestation pregnancies were excluded. The Institutional Review Boards of both sites reviewed and approved the study. Research assistants obtained informed consent from women in the clinic in person. Baseline demographic and clinical data were obtained during enrollment interviews. Data on maternal–infant dyads from the birth hospitalization were abstracted from electronic health records.
Infant feeding data were obtained during telephone interviews at 1, 3, and 6 months postpartum. Women were asked breastmilk and formula feeding frequencies, as well as the following question: “Have you fed your baby anything other than breastmilk or formula?.” If the participant answered yes, she was asked to report the other beverage or food fed and when each food was introduced. Research assistants noted the following prerecorded options: water, sugar water, cow's milk, juice, baby cereal, baby food, and other. For responses other than those listed, participants were asked to specify the beverages and foods, which were recorded by the research assistant verbatim. The age at which the infant was first given each beverage and food was also recorded. Multiple responses were allowed. For analysis, based on prerecorded categories and verbatim responses of participants, we categorized CFBs as follows: cereal, baby food, table food, water, and juice and other liquids (which included sugar water, cow's milk, and other milks). The use of liquid vitamins, medicines, or electrolyte replacement products was not included. Prospective data on working outside the home and smoking were also collected during follow-up interviews.
We used Kaplan–Meier curves to estimate the distribution of time to introduction of each food, due to censoring of data for participants who were lost to follow-up. For example, the time to introduction of a given CFB for a woman who did not complete the 6-month interview, but who had reported not having introduced that CFB at her previous interview, was censored at the time of the last interview. We used log-rank tests to compare the time to introduction of CFBs by demographic and clinical characteristics of study participants. We determined statistical significance by a p-value of <0.05.
Results
Prospective infant feeding data were available for 443 of the 521 women enrolled in the trial. These mothers were 25 years of age, on average, and mostly Non-Hispanic Black or White (Table 1). Most had a high school education or less. Approximately two-thirds were married or living with a partner, and a small minority had no other adults living at home. Forty percent worked outside the home by 6 months postpartum. Of note, over 80% of participants were overweight or obese, based on the prepregnancy body mass index (BMI) recorded in the electronic health record.
Demographic and Clinical Characteristics of Study Participants, n = 443
Maternal complications included placental abruption, uterine atony, preeclampsia, chorioamnionitis, methadone use, and others.
Infant complications included hypoglycemia, transient tachypnea of the newborn, other breathing problems, cardiac problem, hyperbilirubinemia, and others.
BMI, body mass index; ICN, intensive care unit; NICU, neonatal intensive care unit; SD, standard deviation.
Among infants, the majority were full term, and a small minority were low birthweight (Table 1). Over half had some form of minor medical diagnosis during the newborn stay, including hypoglycemia, transient tachypnea, and/or hyperbilirubinemia; however, only a small proportion were admitted to the neonatal intensive care unit (NICU) or intensive care unit (ICN).
By 3 months of age, 48% of infants were fed at least one CFB (Fig. 1). That percentage increased to 65% by 4 months, 83% by 5 months, and over 99% by 6 months. Before 3 months, baby cereal, water, and juice or other liquids were most frequently introduced, each in a small proportion of infants. At 3 months, baby cereal became the most common CFB and remained most common up to 6 months. At 4 months, baby food became the second most common CFB and remained second-most common up to 6 months. In each month beginning at 3 months, there was a sizable increase in the proportion of infants being fed baby cereal and baby foods. By 6 months, ∼20% of infants were receiving juice or other liquids. As previously reported for this study population, rates of exclusive breastfeeding were low. 17 Of note, only 15% (95% confidence interval [CI]: 11–18) of infants were exclusively breastfed at 3 months, and this dropped to 10% (95% CI: 7–13) by 6 months.
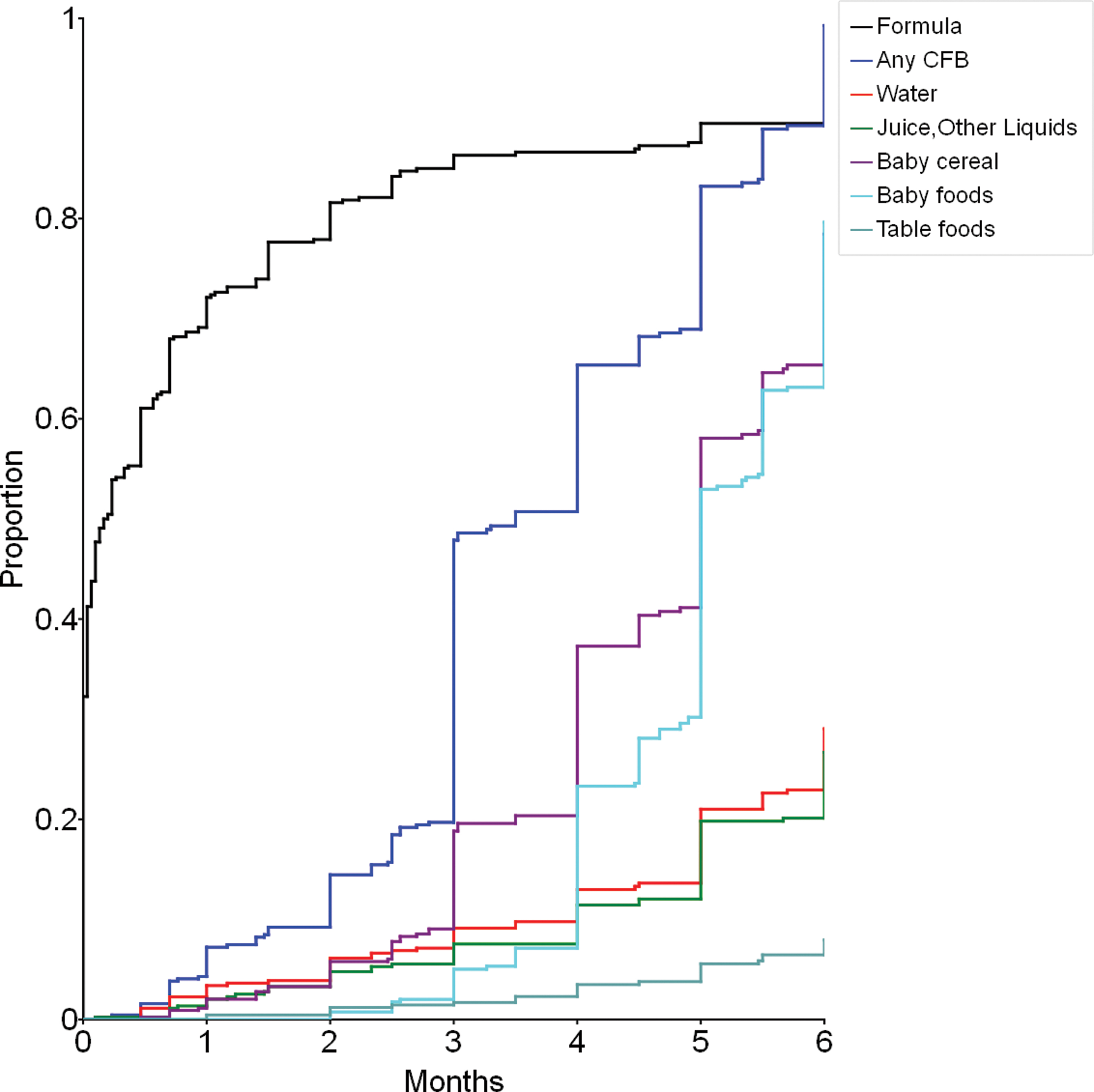
Reported time to introduction of CFBs among mother–infant dyads, n = 443 (Note: time to introduction of formula 19 is shown for reference.) CFBs, complementary foods and beverages. Color images are available online.
We found significant differences in median time to introduction of CFBs by work outside the home and smoking status. The estimated median time to introduction of CFBs among women who did not work outside the home was 3 months compared with 4 months among those who worked outside the home (p = 0.012, log-rank test) (Fig. 2). Similarly, women who reported smoking introduced CFBs earlier than women who reported that they did not smoke (3 months versus 4 months, p = 0.028) (Fig. 3).

Reported time to introduction of CFBs by mother's working outside the home status, n = 443.
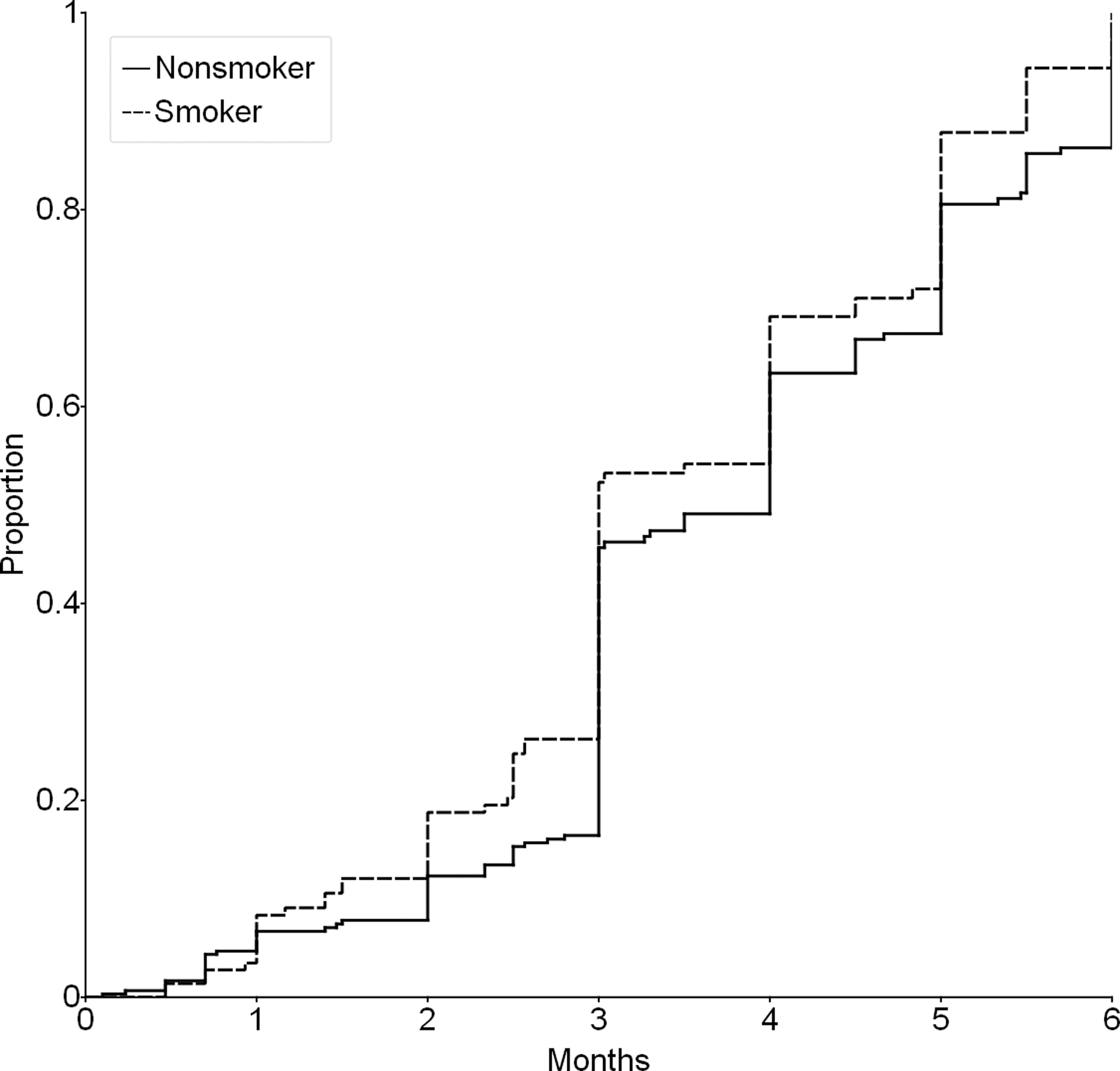
Reported time to introduction of CFBs by mother's smoking status, n = 443.
To assess whether early infant health status may have impacted CFB feeding practices, we compared infants admitted to the ICU or NICU to those not admitted. Timing of introduction of CFBs did not differ between these two groups. Likewise, we assessed whether contact with WIC impacted CFB feeding practices. Since we enrolled women who were eligible, but not necessarily currently enrolled in the program, we asked if women had received any feeding information from WIC. Just over half of participants (288 of 443) indicated during the enrollment or follow-up interviews that they had received such information. We found no difference in timing of introduction of any CFBs when comparing women who had received information from WIC to those who had not.
In addition, we found no significant differences in time to introduction of CFBs based on education, race/ethnicity, whether a partner resided in the home, maternal BMI, intention to breastfeed, or previous breastfeeding experience. Finally, assignment to the intervention or comparison group during the original trial did not impact time to introduction of CFB.
Discussion
Introduction of CFBs before 4 to 6 months of age was common among this population of women with low income. The prevalence of infants who were being fed at least one CFB by 4 months (65%) and by 5 months of age (83%) were each higher than the nationally representative estimates from NHANES (16% for <4 months and 38% for <5 months)9,10 and higher than that reported from a nationally representative WIC population (20% for <4 months). 11 Our findings are consistent, however, with reports of higher rates of use of CFBs among formula-fed infants. 19 Findings from previous research about the role of low income and/or WIC status in timing of introduction of CFBs have been somewhat inconsistent. Whereas a few studies have found these factors to be positively associated with early introduction,10,13,14 others have reported no association 12 or a negative association. 15 Our findings suggest that this population deserves special attention for programming to improve infant feeding practices.
Women who did not work outside the home reported introducing CFBs earlier than those who worked; it is not clear whether this is due to greater familiarity with existing recommendations among working women, convenience, or the practices of childcare centers or other childcare providers. Childcare workers have been shown to differ from mothers in their infant feeding practices. 20 Women who reported smoking also introduced CFBs earlier compared with women who did not report smoking. This is similar to findings from past studies that have shown higher rates of early use of CFBs by smoking status, both in the United States10,21 and elsewhere, 22 and is consistent with research showing that women who smoke are less likely to follow recommended breastfeeding practices. 23 Unlike some previous, nationally representative research,10,24,25 we did not find differences in use of CFBs by level of education or race/ethnicity; however, our study population was more narrowly defined.
As has been documented in prior research,10,12,15,26 we found that the most common CFBs introduced before 3 months were baby cereal and water, followed by juice or other liquids. We found that 20% of participants had introduced juice by 6 months compared with 5–7% for the general U.S. population.9,26 Introduction of sugar water, cow's milk, and other milks was also reported, but in a minority of cases compared with juice. No participant reported use of soda or sweetened tea. Clinical guidance should focus on these foods and beverages specifically, as early as possible during times of patient interaction. Recent research has highlighted the potential relationship between introduction of CFBs before 3 months and altered gut microbiota, which could be a risk factor for obesity or metabolic conditions. 27 In addition, evidence suggests that early introduction of CFBs is related to greater intake of fatty and/or sugary foods as the infant grows. 15
In addition to clinical guidance, existing public health programs such as the USDA's national breastfeeding promotion campaign, Loving Support Makes Breastfeeding Work, 27 could be strengthened to include more specific guidance about introduction of CFBs. Programs for mothers who work outside the home, such as the U.S. DHHS Office on Women's Health Business Case for Breastfeeding, 28 could be enhanced to include educational resources for introduction of CFBs, in addition to promoting exclusive breastfeeding. Given the evidence linking breastfeeding and/or lack of formula use to appropriate timing for introduction of CFBs,5,10,13,24,26 programs to encourage and support exclusive breastfeeding could be beneficial.
It is of critical importance that health interventions be delivered in a culturally sensitive and appropriate manner for the recipients. WIC participants have been shown to rely on family and friends or caregivers who exhibit certain characteristics (e.g., respect and empathy) for infant feeding advice28,29 and have described how they may receive conflicting advice from health care providers, WIC staff, and family members. 30 Accurate information received from social networks 31 and home visits conducted by doulas or peer mentors32,33 have been shown to improve infant feeding practices. Interventions that impact social norms, create peer support programs, and facilitate active participation by recipients should be developed and tested. Preliminary findings from the use of text messaging are encouraging. 34 Programs to improve health literacy would likely also prove beneficial. 35
This study had several limitations. Our study population consisted of women from four clinics at two sites in Virginia, and thus is not representative of all women with low income. We did not have complete data to 6 months for all participants; data were available for at least 3 months for 375 women (85%), and data were available for 6 months for 170 (38%). We do not have information on reasons for loss to follow-up, but we attempted to minimize it by instructing interviewers to contact women a minimum of five times and to call at various times of day. However, this attrition likely resulted in under-ascertainment of the proportion of infants receiving CFBs before 4 to 6 months rather than the opposite. In addition, data were collected by interview, which may have resulted in information bias and overestimated times for use of CFBs if participants responded inaccurately due to their perception of the social acceptability of the use of various CFBs. We do not have information about whether CFBs were given by bottle, cup, spoon, or other route; some women may have been advised to add cereal to bottles, for example. Our ability to assess variation by participant characteristics was limited for some variables, such as ethnicity (due to a small number of Hispanic participants) and education (due to a small number of women with college education or higher). Finally, we were unable to look at differences in timing of introduction of CFBs by breastfeeding status due to the censoring of data and the small proportion of women who were exclusively breastfeeding (15% and 10% at 3 and 6 months, respectively). However, our analysis of prospectively collected infant feeding data provides a more complete description of the timing of CFB introduction than previous cross-sectional studies.
Conclusion
Children born into low-income households face numerous health challenges. Early intervention to facilitate optimal dietary habits is therefore critically important. Future research efforts are needed to better understand health implications of CFBs in terms of specific timing of introduction and how demographic and cultural influences may or may not mediate these relationships. Such information would enable physicians, registered dietitians and qualified nutritionists, and other health care providers to more effectively counsel and support families to follow the new federal guidelines for optimal dietary practices, including timing of introduction of CFBs and breastfeeding practices, from birth to 24 months. 6 Intervention programs using best practices found to be effective for other health-related behavior change should be developed and tested, and special attention should be given to women within this at-risk population.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported in part through a contract with the Virginia Department of Health.