
Abstract
Objectives:
To evaluate the efficacy and safety of domperidone and metoclopramide used by breastfeeding women.
Methods:
A systematic literature search retrieved citations from PubMed, Embase, The Cochrane Library, Medline, EBSCO, Web of Science, ClinicalTrials.gov (from inception to January, 2021) and bibliographies of known articles. Randomized controlled trials exploring the effects of domperidone and metoclopramide in breastfeeding women with term and preterm infants experiencing adequate or low milk supply were identified. Human milk volume and maternal side effects were presented as mean difference (MD) or relative risks (RR) with 95% confidence intervals (CI).
Results:
Sixteen trials involving 729 women were included in the qualitative analysis and 14 trials involving 607 women were included in the meta-analysis. In mothers of preterm infants with low milk supply, domperidone demonstrated a significant increase in daily human milk volume (MD = 90.53 mL/day, 95% CI [65.42 to 115.64], I2 = 9%). However, metoclopramide did not show significant difference in daily human milk volume in women with preterm infants (MD = −1.14 mL/day, 95% CI [−31.42 to 29.14], I2 = 0%). No differences in maternal side effects were noted with domperidone (RR = 1.20, 95% CI [0.74 to 1.97], I2 = 0%) or metoclopramide (RR = 1.05, 95% CI [0.52 to 2.11], I2 = 27%) in women with preterm infants. Regarding the women with term infants, there were insufficient data in the current review.
Conclusions:
Domperidone can be used to treat low milk supply in women with preterm infants without significant side effects based on the current review. More evidence exploring the efficacy and safety of domperidone and metoclopramide are still needed for breastfeeding women in the future.
Introduction
Breastfeeding is the optimal source of enteral nutrition to support the growth and development of term and preterm infants, 1 and it also provides physical and psychological benefits for mothers.2,3 Despite these benefits, a low exclusive breastfeeding rate has been noted worldwide. Global estimates indicate that only 44% of infants are breastfed exclusively in the first 6 months of life. 4 The most common reason for the low rate is that women have been facing many challenges to providing an adequate supply of human milk, 5 with the incidence ranging from 20% to 74%.6,7 The low prevalence rate of breastfeeding is a global health issue 8 and the lack of human milk for infants is a particular nutritional problem. 9
Multiple nonpharmacological interventions have been shown to be effective in promoting human milk supply. 10 However, when nonpharmacological interventions are not effective, therapy with galactagogues is considered. 11 Galactagogues are pharmaceuticals or certain substances believed to assist in the initiation, maintenance, or augmentation of maternal milk supply, 12 thus being used prophylactically or as a treatment for low milk supply in many countries.13,14 The most widely prescribed galactagogues are domperidone and metoclopramide at present. Both are dopamine receptor antagonists that have been demonstrated to be effective treatments for boosting human milk supply. 15 However, no specific galactagogue was recommended by the Academy of Breastfeeding Medicine due to the insufficient supportive evidence.12,16
Although previous systematic reviews have investigated the efficacy of domperidone on promoting milk supply,17,18 some recent trials have been missing from these reviews. Meanwhile, existing trials have demonstrated the contradictory results of metoclopramide in human milk volume, but no meta-analysis has been conducted to further explore these results. Additionally, concerns surround the side effects with the use of domperidone and metoclopramide at present, and the relevance of the side effects to breastfeeding women has been questioned. 19 In light of this, the current review aims to systematically examine previous literature and to evaluate the efficacy and safety of domperidone and metoclopramide used by breastfeeding women with term and preterm infants.
Materials and Methods
Design
This review was conducted complying with the Center for Reviews and Dissemination (CRD) guidelines, 20 and reported following the Preferred Reporting Items for Systematic Review and Meta-analysis (PRISMA) statement. 21 This review was registered on PROSPERO on March 3, 2020, and the registration number is CRD42020171978.
Data sources
A systematic literature search was conducted in seven academic databases (PubMed, Embase, The Cochrane Library, Medline, EBSCO, Web of Science and ClinicalTrials.gov) to identify publications originating from inception to January 6, 2021. The following terms from the National Library of Medical Subject Headings (MeSH), including galactagogues, domperidone, metoclopramide, and breast feeding were combined to identify relevant citations. Other MeSH terms and free text terms in the PubMed database are presented in Supplementary File S1. The search strategy was developed by the researchers of the current study. Reference lists of relevant studies were checked to find any missing studies. Earlier reviews addressing the topic of the current study were also inspected.
Additionally, e-mail alerts from the first six databases were created to discover any new study published before this review being conducted. The remaining database (ClinicalTrials.gov) was reviewed once a month by the researchers (Q.S. and M.-C.D.). The search strategy saved in the platform of these databases was rerun before final analysis (January 6, 2021). No time and language restrictions were applied in the search stage.
Eligibility criteria
The PICOS principle (Population, Intervention, Comparison, Outcomes, and Study design) was used to construct the clinical question and evaluate the eligibility of potentially relevant studies. The population of interest was breastfeeding women with term and preterm infants experiencing adequate or low milk supply or lactation failure. All definitions of low milk supply and lactation failure were included, and the most common definition was human milk supply failing to meet the needs of infants' daily oral feeding requirements. The intervention group received domperidone or metoclopramide prophylactically or as a treatment for low milk supply or lactation failure. The control group accepted placebo or other compounds being considered as galactagogue. The primary outcomes were a change in daily human milk volume as well as maternal and neonatal side effects after domperidone and metoclopramide intervention. Secondary outcomes were differences in daily human milk volume as well as maternal and neonatal side effects between the domperidone and metoclopramide groups. The measurements of human milk volume included using a breast pump to obtain the secretory human milk and weighing the infant before and after feeds in the current review. The side effects were reported by the mothers and infants during the intervention.
Moreover, other relevant outcomes, including breastfeeding duration, milk components, and infant weight gain were initially planned in the current review, but these outcomes were deemed unattainable due to the inadequate and unavailable data of the original trials. Regarding the study design, only randomized controlled trials (RCTs) were included in this study. However, RCTs published in other formats (e.g., conference abstract, letter) were also eligible for inclusion after obtaining sufficient data when we communicated with the corresponding author of the research. Trials without published data and sufficient data after attempting to contact authors were excluded. Trials involving animals were excluded.
Study selection and data extraction
The study selection was conducted based on a three-step screening process: literature retrieval, preliminary review, and full-text review. Literature retrieval was independently conducted by two researchers (Q.S. and M.-C.D.) and all selected articles were exported into EndNote (version X9, 2018). Subsequently, the same researchers preliminarily filtered the selected articles by reviewing titles and abstracts after identifying duplication. Finally, full texts were retrieved and reviewed following the eligibility criteria. Disagreements in selection were resolved through consulting with a third researcher (W.-W.D.).
A standardized data extraction sheet was used to obtain the following data: first author, publication year, country, participants' characteristics, intervention methods, control methods, and main outcomes. Meta-analysis was conducted based on daily human milk volume as well as maternal side effects. Meanwhile, meta-analysis of neonatal side effects was not performed due to the limited reporting in the original trials. The outcome of human milk volume was considered as the changes between the final value and baseline value, or the final value only when the baseline value was missing after communicating with the authors of the trial. The changes in human milk volume were employed by the two comparisons, including domperidone versus placebo and domperidone versus metoclopramide. The final value in human milk volume was used in the comparison between metoclopramide and placebo. Additionally, formulas calculating the changes in human milk volume were adopted from the previous relevant review, 18 which are presented in Supplementary File S2. Events of maternal side effects were considered as the incidence of side effects in mothers. Disagreements in extracted data were resolved by discussion of the research team.
Risk of bias assessment
The risk of bias for each included study was evaluated using the Cochrane Collaboration bias risk assessment tool and each item was assessed as “low risk,” “unclear risk,” or “high risk.” 22 Disagreements between researchers were resolved in discussion with the third reviewer (K.S.K.).
Statistical analyses
All included studies were analyzed qualitatively to summarize the outcome of human milk volume and side effects. Qualitative analysis was an approach of systematically reviewing and synthesizing the results from included studies, which primarily relied on the use of words and text to summarize and explain the synthesized results. 23
The meta-analysis was conducted by the Review Manager (Version 5.3, the Cochrane Collaboration, Copenhagen, 2014), with a significance level of 0.05. Relative risks (RR) with 95% confidence intervals (CI) were utilized for dichotomous variables, and mean difference (MD) with 95% CI were reported for continuous variables. The inverse variance and Mantel–Haenszel methods were applied to estimate the pooled results with a random effects model. A random effects model was employed since the data were not similar (e.g., inconsistent definition of inadequate milk supply and lactation failure). Heterogeneity was quantified using chi-square combined with I2 statistics in each pooled analysis. Heterogeneity was not regarded as important if I2 was less than 40% or the p-value of chi-square test was greater than 0.1. 24 Subgroup analysis was performed on the basis of the women with term or preterm infants as well as women with adequate or low milk supply. Sensitivity analyses were conducted to explore the impact of an individual study on the overall result following the sequential exclusion of each individual study, which was considered as a critical approach given that a random effects model was chosen. 21
Results
Study selection and study characteristics
In total, 16 studies met inclusion criteria after 2,138 articles were identified from PubMed (n = 251), Embase (n = 615), The Cochrane Library (n = 145), Medline (n = 300), EBSCO (n = 580), Web of Science (n = 231), ClinicalTrials.gov (n = 13), and other sources (hand searching of references) (n = 3). After the 3-step screening process, 2,122 articles were excluded and 16 articles on domperidone and metoclopramide were retained for qualitative synthesis. The summary of the reasons for excluding studies during full-text review is presented in Supplementary File S3. No eligible trial was found after rerunning the literature retrieval in the seven databases before the final analysis (January 6, 2021). Therefore, 16 studies were ultimately retained for qualitative synthesis,25–40 and 14 trials were entered into the meta-analysis (Fig. 1).25–29,31–36,38–40
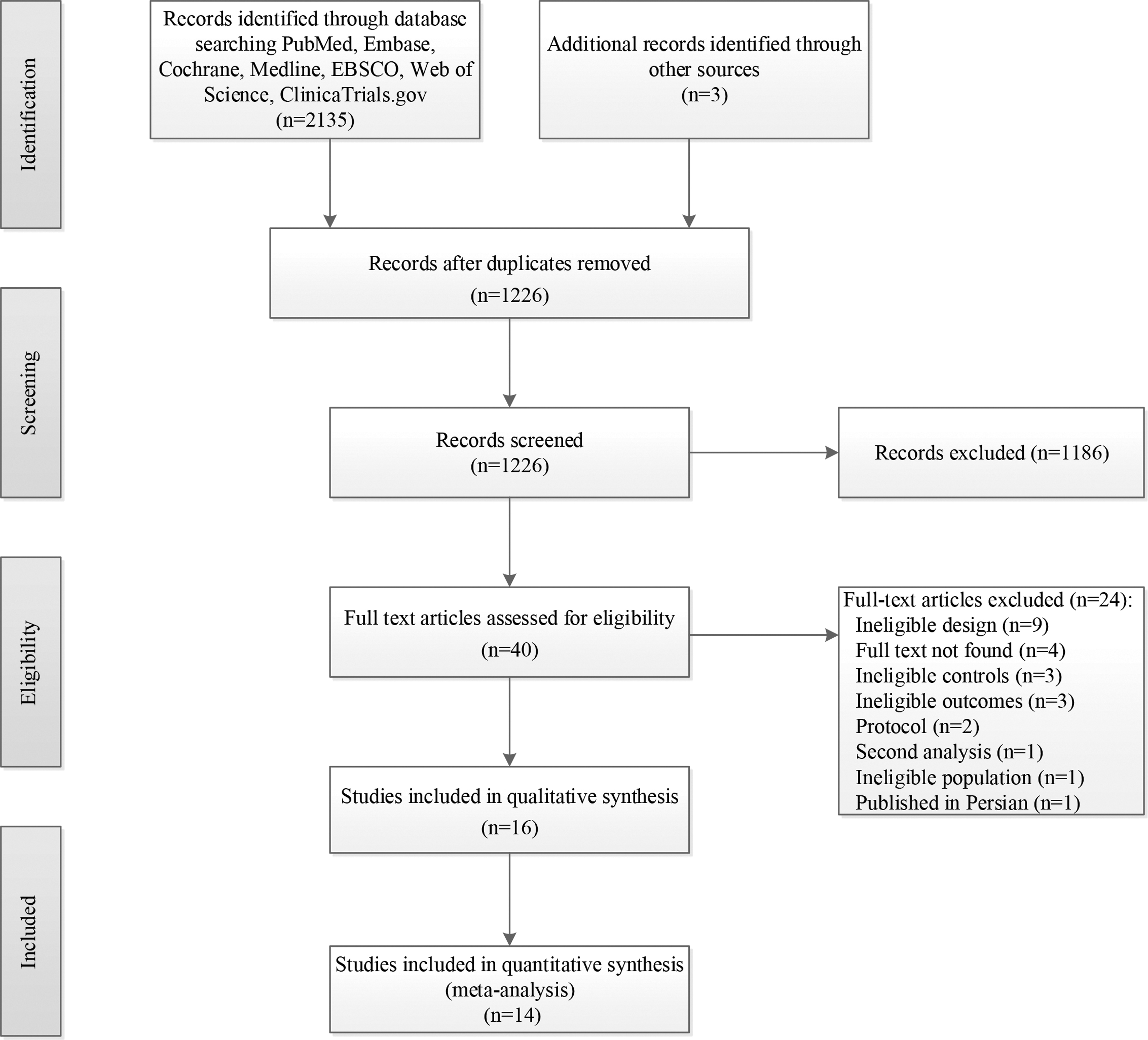
PRISMA flow diagram. PRISMA, Preferred Reporting Items for Systematic Review and Meta-analysis.
Sixteen RCTs involving 729 women were included in the current review. Ten trials were conducted in high-income countries: three in Canada,26,27,32 two in the United States,38,39 one each in Australia, 25 United Kingdom, 28 Belgium, 35 Finland, 36 and Hungary. 37 The remaining six trials were conducted in the low- and middle-income countries, with two in Thailand,29,34 one each in Pakistan, 30 India, 31 Indonesia, 33 and Iran. 40 The detailed characteristics of the included studies are summarized in Table 1.
Characteristics of Included Studies
The human milk volume was less than 250 mL/day.
The human milk volume was measured by using a breast pump.
The human milk volume did not meet the infant's daily nutritional needs.
Lactation failure was defined by meeting at least one of the following criteria: (1) a decreasing milk supply by 30% from peak volume (based on maternal account); and (2) inability to provide adequate breast milk to meet the infant's daily nutritional needs.
The human milk volume was less than 160 mL/kg/day (based on their infant's birth weight).
The human milk volume was less than 10 mL milk volume per single expression (both breasts) at sixth postnatal day.
The efficacy on human milk volume was presented by a categorical variable (Yes/No) (the “YES” was defined as more than 50 mL human milk volume per single expression (both breasts) after 7 days use of domperidone or placebo).
Not stated.
The human milk volume was less than 150 mL/kg/day (based on their infant's birth weight) during the 72-hour period before study entry or a maternal report of milk volume reduction by more than one-third from a peak volume of the previous 72 hours.
Lactation failure was defined as decreased human milk supply (more than 30% of maximum human milk volume) and/or inability to produce an adequate amount of human milk to meet the infant's daily nutritional needs.
The human milk volume was less than 350 mL/day during 14 days postpartum or human milk does not meet the neonate's daily feeding requirements after 7 days of life.
The human milk volume was measured by weighting the infant before and after each feeding.
The human milk volume was less than 500 mL/day.
Quality of individual studies
The risk of bias assessment of included studies is summarized in Table 2, and a detailed description and justification is outlined in Supplementary File S4. Overall, the main area of possible bias in the original studies was related to three aspects. An “unclear risk of selection biases” was observed in eight studies, with lack of the clear demonstration of randomization process 26 or allocation concealment25,30,33,40 or both.35–37 Moreover, six studies were related to a “high risk of attrition biases” due to the moderate attrition rate (≥10% attrition rate),25,26,28,34,36,39 and an “unclear risk of attribution biases” in one study was owing to a lack of reasons for participants' withdrawal. 38 Additionally, an inadequate reporting of the study protocol results in “unclear risk of reporting biases” in most of the studies.25,26,28–31,34–40
Risk of Bias Among Included Studies
H, high risk of bias; L, low risk of bias; U, unclear risk of bias.
Results of individual studies
Human milk volume: qualitative review
Nine studies of domperidone reported outcomes related to the human milk volume.25–27,29–34 Eight studies of domperidone reported human milk volume as continuous variables, which showed a statistically significant higher human milk volume irrespective of whether it was used in mothers of preterm infants with low milk supply25–27,31–33 or mothers of term infants 29 or mothers of both preterm and term infants with low milk supply. 34 Meanwhile, the remaining one study 30 reported human milk volume as dichotomous variables, which also demonstrated a statistically significant higher human milk volume in mothers of term infants with low milk supply.
Regarding metoclopramide, all studies reported human milk volume as continuous variables.35–40 However, conflicting results in human milk volume were reported with the use of metoclopramide. Two studies reported that metoclopramide significantly increased human milk volume in mothers of term infants with adequate maternal milk supply.35,37 Meanwhile, the other study also showed that metoclopramide increased human milk volume in breastfeeding women with low milk supply, 36 but this study did not clarify whether it included women with term or preterm infants or both. Moreover, the other three studies involving mothers of preterm infants38,39 and term infants 40 showed that the use of metoclopramide was not associated with increased human milk volume. Additionally, two studies involving mothers of both preterm and term infants reported that domperidone produced a higher milk volume than metoclopramide in treating low milk supply, although no statistically significant difference was observed.25,28
Side effects: qualitative review
Nine studies of domperidone assessed maternal25,28,29,31,33,34 or neonatal side effects or both.26,27,32 Of the nine studies, five studies showed no adverse side effects in domperidone intervention.26,27,31,33,34 The remaining four studies reported the adverse side effects during domperidone intervention, and the specific incidence and types of side effects are presented in Table 3. The cardiac adverse events in mothers and infants were only evaluated in Asztalos et al.'s study. 32 No evidence of prolongation of Q-Tc interval was reported in all women. Meanwhile, a total of five infants reported long Q-Tc interval, with two in the domperidone group and three in the placebo group, but all infants were clinically asymptomatic and no intervention was needed.
Maternal Side Effects of Domperidone and Metoclopramide
Only Asztalos et al.'s study 32 reported neonatal side effects, including pulmonary/gastrointestinal/neurological/genitourinary symptoms, long Q-Tc interval (>500 ms), infection, death (due to respiratory failure and extreme prematurity). The ratio of neonatal side effects in intervention versus control was 14/45:14/45.
Regarding metoclopramide, six studies assessed maternal side effects25,28,36,39,40 or neonatal side effects or both. 35 Of the six studies, only one study reported no maternal and neonatal side effects during metoclopramide intervention. 35 The adverse maternal side effects were noted in other five studies, which are listed in Table 3. The central nervous system symptoms (e.g., headache) and the psychological symptoms (e.g., anxiety, depression) were the commonly reported maternal side effects.28,36,39,40
Data synthesis
Human milk volume associated with domperidone and metoclopramide
Eight RCTs of domperidone involving 247 mothers of preterm infants with low milk supply25–27,31–33 and 45 mothers of term infants 29 and 34 mothers of both preterm and term infants with low milk supply 34 provided data on the changes of daily human milk volume. The overall pooled result showed that domperidone increased daily human milk volume by 94.11 mL/day (95% CI [74.02 to 114.20], p < 0.001) in breastfeeding mothers, with no statistical heterogeneity (I 2 = 0%, p = 0.48) (Fig. 2). Specifically, the subgroup analysis in mothers of preterm infants with low milk supply revealed that domperidone increased daily human milk volume by 90.53 mL/day (95% CI [65.42 to 115.64], p < 0.001), with an acceptable statistical heterogeneity (I 2 = 9%, p = 0.36). Data on the human milk volume in mothers of term infants 27 and mothers of both term and preterm infants with low milk supply 34 were not synthesized since only one study was included in the subgroups. Sensitivity analysis revealed that the exclusion of these individual studies did not substantially influence the overall pooled result in maternal human milk volume among breastfeeding mothers who received domperidone intervention (Supplementary File S5).
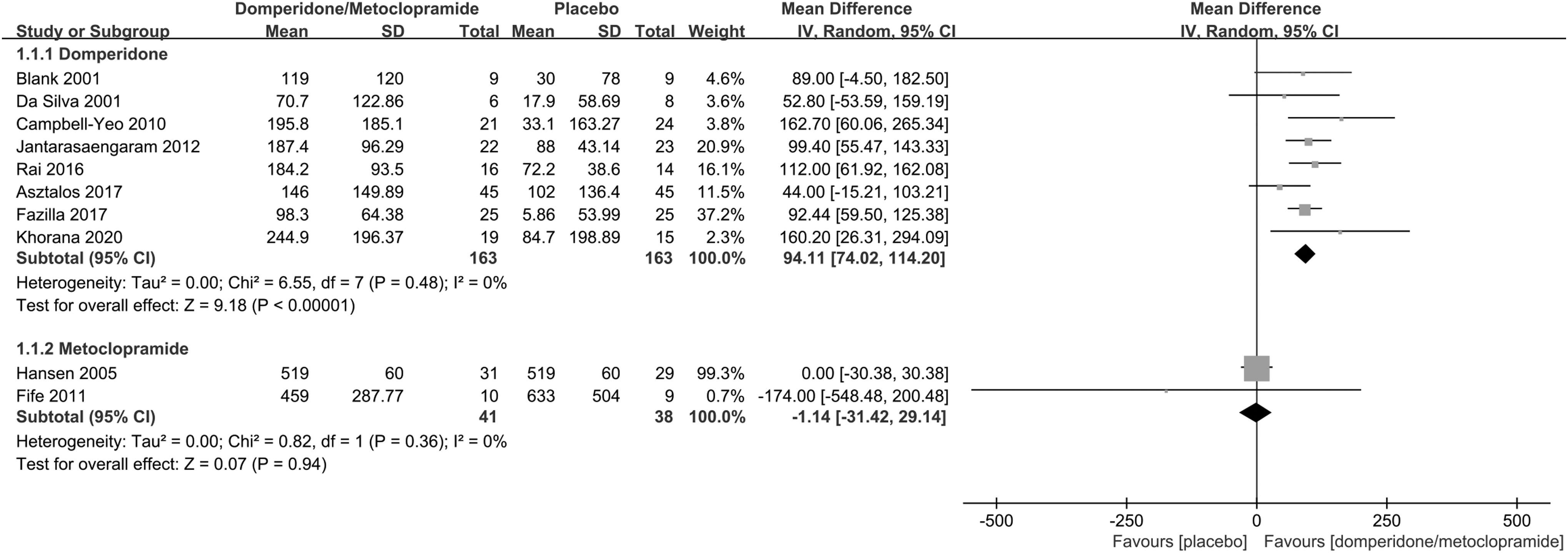
Forest plot of domperidone and metoclopramide compared with placebo in human milk volume among breastfeeding women.
Data on metoclopramide were reported in three RCTs involving 136 mothers of term infants,35,37,40 two RCTs, including 79 mothers of preterm infants,38,39 and one RCT involving 29 mothers of preterm infants with low milk supply. 25 The overall pooled result of metoclopramide in breastfeeding mothers was not displayed due to a substantial statistical heterogeneity (MD = 25.59, 95% CI [−5.05 to 56.23], p = 0.10; I2 = 75%, p < 0.01). The subgroup analysis revealed that the use of metoclopramide was nonsignificant (MD = −1.14 mL/day, 95% CI [−31.42 to 29.14], p = 0.94) in human milk volume among mothers of preterm infants, and no statistical heterogeneity was observed (I 2 = 0%, p = 0.36) (Fig. 2). Meanwhile, the pooled analysis of metoclopramide versus placebo in mothers of term infants was also not displayed considering a substantial statistical heterogeneity (MD = 38.91, 95% CI [−11.83 to 89.66], p = 0.13; I2 = 88%, p < 0.001). Data on the human milk volume in mothers of preterm infants with low milk supply were not synthesized since only one study 25 was included in the subgroup.
Maternal side effects of domperidone and metoclopramide
Maternal side effects of domperidone were assessed in 8 RCTs,25–27,29,31–34 including 328 participants. No statistically significant difference in the incidence of maternal side effects was found between the domperidone group and the placebo group (RR = 1.30, 95% CI [0.48 to 3.50], p = 0.61) with the acceptable heterogeneity of 37% (p = 0.19) (Fig. 3). The result of subgroup analysis was also nonsignificant in mothers of preterm infants (RR = 1.20, 95% CI [0.74 to 1.97], p = 0.46), with no statistical heterogeneity (I 2 = 0%, p = 0.53). Data on the maternal side effects in mothers of term infants were not synthesized since only one study 29 was included in the subgroup. Sensitivity analysis revealed that the omission of these individual studies did not substantially influence the overall pooled result in maternal side effects among breastfeeding mothers who received domperidone intervention (Supplementary File S5).

Forest plot of domperidone and metoclopramide compared with placebo regarding maternal side effects in breastfeeding women.
Regarding metoclopramide, 5 RCTs involving 185 women reported the incidence of side effects.25,35,36,39,40 There were no significant differences in the incidence of maternal side effects between the metoclopramide and placebo groups (RR = 1.04, 95% CI [0.59 to 1.84], p = 0.89). A medium heterogeneity of 53% was observed (p = 0.10) (Fig. 3), and the reason for the heterogeneity may be due to the different participant's characteristics (women with preterm or term infants). A similar effect was observed in mothers of preterm infants (RR = 1.05, 95% CI [0.52 to 2.11], p = 0.89), and the heterogeneity was reported to be 27% (p = 0.24). Data on the maternal side effects in mothers of term infants were not synthesized since only one study 40 was included in the subgroup. Sensitivity analysis revealed that the omission of these individual studies did not substantially influence the overall pooled result in maternal side effects among breastfeeding mothers who received metoclopramide intervention (Supplementary File S5).
Human milk volume and side effects between domperidone and metoclopramide
Data on human milk volume of domperidone versus metoclopramide were found in 2 RCTs involving 20 mothers of preterm infants with low milk supply 25 and 65 mothers of both preterm and term infants with low milk supply. 28 The use of domperidone resulted in a higher volume of expressed human milk compared with metoclopramide, but no significant difference was found (MD = 33.36 mL/day, 95% CI [−17.74 to 84.47], p = 0.20). No heterogeneity was observed in these two studies (I 2 = 0%, p = 0.96) (Fig. 4). The subgroup analysis on human milk volume was not conducted in the subgroups due to the limited number of RCTs.

Forest plot of domperidone versus metoclopramide regarding milk volume.
Data on the incidence of maternal side effects of domperidone versus metoclopramide were found in 2 RCTs involving 20 mothers of preterm infants with low milk supply 25 and 65 mothers of both preterm and term infants with low milk supply. 28 No significant difference was found in the incidence of maternal side effects between the domperidone group and the metoclopramide group (RR = 0.65, 95% CI [0.23 to 1.81], p = 0.41). There was no heterogeneity in these two studies (I 2 = 0%, p = 0.38) (Fig. 5). The subgroup analysis on maternal side effects was not conducted in the subgroups due to the limited number of RCTs.

Forest plot of domperidone versus metoclopramide regarding maternal side effects.
Discussion
The current review demonstrated that domperidone could significantly increase human milk volume in mothers of preterm infants with low milk supply. However, metoclopramide did not demonstrate a statistically significant increase in human milk volume among women with preterm infants. Moreover, compared with placebo, no significant differences in the incidence of maternal side effects were observed in domperidone and metoclopramide, and no serious maternal and neonatal side effects were reported in the current review. Additionally, no significant differences in human milk volume and maternal side effects were observed between the domperidone and metoclopramide groups in breastfeeding mothers with low milk supply. However, full analysis was not performed to explore the efficacy and safety of galactagogues in mothers of term infants due to the limited number of RCTs in the current review.
Effects of domperidone and metoclopramide on milk volume
Most trials of domperidone were conducted in mothers of preterm infants with low milk supply in the current review, and the positive effect on the human milk volume was consistent with a previous meta-analysis. 15 This finding could be attributed to the mechanism of domperidone, which is a dopamine antagonist improving milk supply through stimulating prolactin release. 11 Regarding term infants, a recent Cochrane review 41 reached the same conclusion as the current review. Although a meta-analysis cannot be performed in this subgroup given the limited available data, the two studies included in this review demonstrated a positive effect on human milk volume. Therefore, high-quality RCTs are needed to explore the effects of domperidone on human milk volume among women with term infants.
Although metoclopramide is also a dopamine antagonist, no significant increases were observed in human milk volume among mothers of preterm infants in the current review. A recent trial involving 112 breastfeeding women drew the same conclusion as the current review. 40 This finding may be attributed to a shorter duration of the intervention. The intervention duration was 5 days in Tabrizi et al.'s study, 40 which was similar to the current study (6.8 days on average). However, a previous study reported different results with metoclopramide on human milk volume in mothers of term infants with low milk supply. 40 The variation in intervention duration should be taken into consideration to explain the difference. The intervention duration was 14 days in Kauppila et al.'s study, 42 but 6.8 days on average in the current study. Another consideration might be the different characteristics of the participants. Kauppila et al.'s study 42 included women with term infants, whereas participants in the current study were women with preterm infants. Additionally, the purposes of using metoclopramide (prophylaxis or treatment) should also be considered to interpret this difference. Women in Kauppila et al.'s study 42 received metoclopramide as a treatment for lactation deficiency, whereas women in the current meta-analysis could have used metoclopramide prophylactically when we communicated with authors of the original trials and consulted with two experts in galactagogues. However, no studies were conducted to explore the difference in milk production in women with these different characteristics (e.g., different duration, preterm or term infants, prophylactic or treatment setting) during the metoclopramide treatment.
The side effects of domperidone and metoclopramide
There were no significant differences in the incidence of maternal side effects in domperidone (versus placebo) and metoclopramide (versus placebo). This result could be interpreted that no increased risk of incidence of maternal side effects has been identified during domperidone and metoclopramide treatment based on the current meta-analysis. However, it should be noted that this result was from a small sample size of the current meta-analysis (a litter over 100 in domperidone and less than 100 in metoclopramide), which needs further exploration in a large sample of breastfeeding women. Regarding the types of maternal side effects, concerns have been raised about the cardiotoxicity while using domperidone in recent years. 43 A population-based cohort study involving 247,349 women showed that no ventricular arrhythmias or sudden cardiac deaths was occurred among 1,438 domperidone users. 14 Meanwhile, another retrospective population-based cohort study involving 225,532 postpartum women reported that the ventricular arrhythmia just occurred in domperidone users with a previous history of ventricular arrhythmia, 44 which implied that no cases of ventricular arrhythmia were identified among domperidone users with no prior history. Therefore, domperidone should be prescribed with caution, especially in women with a history of cardiac disease.
Regarding metoclopramide, the particular concern in metoclopramide is the increased risk of depression, and women in the postpartum period are more vulnerable to depression. 5 A larger survey of women taking metoclopramide for lactation enhancement found that 12.1% of women reported depression. 45 Meanwhile, Ingram et al. reported 6.9% of women experiencing depression but after the trial intervention period. 28 Therefore, women with a history of depression should avoid using metoclopramide, and women should avoid prolonged use during this period of high susceptibility. 46
Additionally, neonatal side effects were rarely reported in the review. The possible reason may be due to the lower detected serum galactagogue concentration in infants. The absolute infant dose of serum domperidone concentrations was 0.04 (95% CI 0.03 to 0.07) μg/kg/day at a maternal dose of 30 mg daily, and 0.07 (95% CI 0.05 to 0.11) μg/kg/day at a maternal dose of 60 mg daily. 47 However, compared with domperidone, there are greater amounts of metoclopramide secreted into the human milk at a maternal dose of 30 mg daily. The reported maximum absolute infant dose ranged from 6 to 24 μg/kg/day during the early postpartum period and from 1 to 13 μg/kg/day during the late postpartum period. 48 Although the relative infant doses in the galactagogues are below the acceptable relative infant dose (10%), 49 the potential risk of infant toxicity should not be ignored due to some reported cases of neonatal side effects during intervention. 32 In summary, considering the maternal and neonatal side effects, a benefit/risk analysis should be performed in breastfeeding mothers who received domperidone and metoclopramide for improving human milk supply. It is suggested that health care providers should consider nonpharmacological interventions in advance before using any galactagogues for breastfeeding women, especially in women who received a galactagogue prophylactically. 12 Nonpharmacological interventions are very effective in improving breastfeeding success.10,32,34
The comparative efficacy and safety between domperidone and metoclopramide
No significant difference in human milk volume was found between the domperidone and metoclopramide groups in breastfeeding mothers with low milk supply. This finding can be attributed to the fact that both domperidone and metoclopramide are dopamine D2 receptor antagonists, thus having a similar mechanism to treat low milk supply. 12 However, the contradictory results of metoclopramide in human milk volume should be noted in the current review, which are the negative result on human milk volume in metoclopramide (versus placebo) and the nonsignificant result on human milk volume in metoclopramide (versus domperidone). The current researchers surmised that this result could be possibly due to the different purposes of metoclopramide (prophylactic versus treatment for low milk supply), which may constitute an important issue that needs further exploration. When it comes to the maternal side effects, no significant difference in the incidence of maternal side effects was found between domperidone and metoclopramide groups in the current review. This finding was inconsistent with an observational study involving 1,990 mothers, which identified that women who received domperidone were 3.6 times more likely to report no adverse side effects compared with those who received metoclopramide. 45 Therefore, the comparison of metoclopramide and domperidone in the safety issue needs being further verified in large-sample multicenter studies.
Strengths and limitations
The comparisons between domperidone and metoclopramide on human milk volume and side effects in the current meta-analysis are the first reported comparisons. The pooled results on the efficacy and safety of metoclopramide are also the first explored analyses. Additionally, the current meta-analysis of domperidone included all eligible trials, which was helpful to provide more comprehensive and robust findings.
However, some limitations need to be acknowledged in this review. First, the homogeneity of the included studies varies in some aspects: participant characteristics (e.g., delivery mode) and the definition of low milk supply. These differences may lead to doubtful results, implying the need for more standard designed trials. Second, the meta-analysis of human milk volume in domperidone and metoclopramide was found in mothers of preterm infants, so it cannot be generalized to mothers of term infants. Third, the small number of studies and participants are an important limitation, but the researchers have systematically reviewed and synthesized all eligible trials compared with other reviews. Fourth, older and low-to-moderate quality original studies were included in the current review to obtain a more systematic and comprehensive understanding of domperidone and metoclopramide. Higher quality and multicenter original trials to explore the efficacy and safety of domperidone and metoclopramide are recommended in future research. Fifth, the substantial heterogeneity in the subgroup analysis of metoclopramide versus placebo on human milk volume in mothers of term infants cannot be explained due to the unclear reporting in the original trials. Finally, selection bias may exist in the current review because only articles published in English were included.
Conclusions
There was evidence to support that domperidone can be used to treat low milk supply in breastfeeding women with preterm infants. Moreover, due to the limited evidence in the current review, large sample size, high-quality trials exploring the efficacy and safety of domperidone and metoclopramide are needed for improving the therapeutic management of inadequate milk supply in breastfeeding women with both term and preterm infants.
Footnotes
Author Contributions
All authors contributed to the conception or design of the work. Q.S., K.S.K., M.-C.D., and W.-W.D. contributed to data acquisition, analysis, and interpretation. Q.S. drafted the article. Q.S., K.S.K., and Y.-Q.O. critically revised the article. All authors agreed on the final version of the article and take responsibility for its content.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.