
Abstract
Objective:
To evaluate the impact of the duration of breastfeeding on the intelligence of children.
Materials and Methods:
Eight electronic databases were searched to identify studies that investigated the impact of breastfeeding on the intelligence of children. Data were pooled, and the ratio of means (RoM) and the corresponding 95% confidence interval (95% CI) were calculated using a pairwise meta-analysis and network meta-analysis. Risk of bias was assessed using a tool developed by the CLARITY group. Data were analyzed using R version 3.5.1.
Results:
A total of 15 studies with 12,316 subjects were included in the review. Half of the studies were at low risk of bias. A meta-analysis indicated that breastfed children had a score 1.04-fold higher in intelligence tests compared with those that had never been breastfed (RoM: 1.04, 95% CI: 1.02–1.06, p < 0.05). Evidence from a network meta-analysis indicated that breastfeeding for ≤6 months resulted in score 1.04-fold higher in intelligence tests (RoM: 1.04, 95% CI: 1.03–1.06, p < 0.05) and children breastfed for >6 months had a score 1.06-fold higher (RoM: 1.06, 95% CI: 1.05–1.08, p < 0.05) than children that had never been breastfed. Thus, breastfeeding for >6 months demonstrated a slightly higher score than breastfeeding for ≤6 months (RoM: 1.02, 95% CI: 1.00–1.04, p < 0.05).
Conclusion:
Breastfeeding could significantly improve the intelligence of children, with a duration of >6 months showing a slight but significantly higher intelligence score than for ≤6 months.
Introduction
The association between breastfeeding and child intelligence has been the focus of numerous studies since Hoefer and Hardy initially observed in 1929 that children breastfed for 4 to 9 months had higher performance and educational quotients than those that were bottle-fed or those that experienced shorter or longer periods of breastfeeding. 1 Several studies2–4 have demonstrated a positive association between breastfeeding and health outcomes in children. Two randomized trials5,6 on this issue have previously reported significant benefits of breastfeeding, suggesting that this association was causal. It has been hypothesized by some that the beneficial effects of breastfeeding on the neurodevelopment of children are mediated by long-chain polyunsaturated fatty acids (PUFAs) which are present in human milk, 7 but not in the milk of cows or in the majority of infant formulae. 8 The long-chain PUFAs in breast milk that could perform a role in developing intelligence include docosahexaenoic acid and arachidonic acid. 9
In October 1999, a meta-analysis comprising 20 studies demonstrated that after adjusting for several key confounders, breastfed children scored higher for cognitive development compared with children who had been exclusively bottle-fed (mean difference [MD]: 3.16 points; 95% confidence interval (CI): 2.35–3.98). 10 Evidence also indicated that the increase in cognitive ability was associated with a longer duration of breastfeeding.11–13 Three studies11,14,15 suggested that, in addition, breastfeeding was positively associated with educational attainment. A meta-analysis published in 2013 included 14 observational studies that observed that the impact of breastfeeding on intelligence demonstrated a 3.5 point (95% CI: 1.9–5.0) higher score in intelligence tests compared with nonbreastfed children, and after adjusting for maternal intelligence, breastfeeding was associated with an additional 2.19 intelligence quotient (IQ) points. 16
An additional meta-analysis 17 published in 2015 reported that IQ was 3.44 points (95% CI: 2.30–4.58) higher among subjects who had been breastfed, and this association was observed even among studies that controlled for maternal intelligence. However, these meta-analyses failed to compare the impact of different durations of breastfeeding on intelligence tests. There are risks in uncritically accepting the results of meta-analyses; it is important for users to identify high-quality meta-analyses. 18 They did not perform any risk of bias assessment of studies included in their reviews. Those studies used MDs to analyze their results, but it is important to note that different intelligence tests were compared. Pooled MDs have an unfavorable statistical characteristic of negative bias.
In the present review we conducted a comprehensive systematic review and frequentist network meta-analysis to assess the association of breastfeeding with intelligence in children, particularly the impact of duration of breastfeeding.
Materials and Methods
Search strategy and selection criteria
An extensive systematic search of PubMed, the Cochrane Library, Embase, Web of Science, China National Knowledge Internet (CNKI), VIP database, Wanfang Data Knowledge Service Platform, and China Biomedical Literature Database (CBM) was conducted from their inception to December 2020. The references of articles and relevant systematic reviews and meta-analyses that were identified were also investigated for additional studies. The literature search used the following terms: breastfeeding, breastfeeds, breastfed, lactation combined with the terms for the outcome: cognitive, cognition, psychomotor, sensorimotor, cognitive development, psychological development, neurodevelopment. The precise search strategy is available from the authors upon request.
To be eligible, studies were required to satisfy the following criteria: (1) the authors had focused on healthy term infants and not those at increased biological risk of delays in development (e.g., prematurity or intrauterine growth restriction); (2) the primary outcome was intelligence of children measured using validated methods or standard tests (e.g., Stanford–Binet Intelligence Scale, Wechsler Intelligence Scale (WISC) for Children revised); (3) estimates were adjusted for stimulation or interaction with the child; and (4) it was a cohort study.
Studies were excluded if: (1) the study group included preterm or babies that were small for their gestational age; (2) evaluation of intelligence did not use standardized tests or used only a nonreliable or subjective tool (such as school grades or maternal report); and (3) insufficient data had been reported.
EndNote X8 literature management software was utilized to manage the bibliographic records searched. Titles and abstracts of all the retrieved bibliographic records were screened independently by two reviewers (L.Y.H., Y.F.L.) according to the eligibility criteria. Any potential eligible studies were further evaluated by reviewing the full text. Any conflict on inclusion/exclusion was resolved by consensus or through consultation with a third reviewer (L.G.).
Data analysis
The following data were extracted from eligible articles: first author, year of publication, study design, country, sample size, gender, categorization of breastfeeding, assessment tool, and age at assessment. Data included were means ± standard deviations (SDs) at the end of each study. If such values were not available, data were imputed according to the Cochrane Handbook. 19 Also extracted were the key confounders reported in each study (Supplementary Appendix Table SAT1). This information was collected by two independent reviewers, with discrepancies being settled by discussion and consensus.
Two reviewers independently assessed the risk of bias of studies included in the review using a tool developed by the CLARITY group, 20 which included the selection of exposed and nonexposed cohorts, assessment of exposure, outcomes of interest at the start of the study, statistical analysis adjusted for prognostic variables, assessment of the presence or absence of prognostic factors, and assessment of outcomes. Each parameter was scored as “definitely or probably yes” (assigned a low risk of bias) or “definitely or probably no” (assigned a high risk of bias). Individual studies were categorized as high quality if ≥4 of 6 items were scored as low risk of bias, otherwise they were considered low quality. Any conflict in final categorization was resolved by consultation with the third reviewer (L.G.).
Published SDs were used, where available. If a standard error was presented rather than SD, it was converted to a SD.
21
SDs were estimated from CIs in the study of Bernard et al.
22
using the Cochrane method. The SDs of each group were imputed from the SD of the MDs, which were reported in Johnson et al.,
23
in addition to the SD between groups. The missing SDs were imputed for two studies (Eickmann et al.
24
and Lee et al.
25
) using pooled SDs from other studies included in our meta-analysis using the following formula
26
:
A pairwise meta-analysis was performed to compare breastfed children with those that had never been breastfed. For the breastfed group, some multiarm studies reported different durations of breastfeeding versus never breastfed. The different durations were merged or the never breastfed group split in accordance with the following steps: (1) Different durations of breastfeeding were merged using the inverse variance method if no significant difference existed between them. For example, Morrow-Tlucak et al. 13 was a three-arm study that compared breastfeeding for ≤4 months and for >4 months to nonbreastfed children. The breastfed for ≤4 and >4 months groups were merged into a single breastfed group because no significant difference was observed between them (p = 0.85). (2) Never breastfed groups were split to adapt groups of different duration if there was no significant difference between different durations of breastfeeding, for example, Gomez-Sanchiz et al. 27 published a three-arm study that compared breastfeeding for ≤4 months and for >4 months to never breastfed children. The never breastfed group was averaged into both breastfed groups because a significant difference between breastfeeding for ≤4 months and for >4 months was found (p < 0.001), that is, Gomez-Sanchiz et al. were split into two separate two-arm studies, that is, breastfeeding for ≤4 months versus never breastfed and breastfeeding for >4 months versus never breastfed.
In general, when the same measurement unit was used for outcomes of interest among studies, the MD was considered a treatment effect for analysis of the results, or a standardized MD (SMD) was considered. However, when studies in meta-analyses were weighted by the inverse of the variance of the effect measure, the pooled SMD had the unfavorable statistical characteristic of negative bias. 28 In our analysis, we included different intelligence assessment measures. We used the ratio of means (RoM) to measure an intervention effect in the breastfed group relative to the never breastfed group, 29 which accounted for the baseline difference being roughly comparable through different measurement units.
We used the meta package of R software version 3.5.1 (R Foundation for Statistical Computing, Vienna, Austria) to calculate the RoM between the breastfed and never breastfed groups and perform a pairwise meta-analysis using the inverse of variance method. The results were presented as forest plots.
We categorized different durations of breastfeeding to ≤6 and >6 months and compared their relative effects using a network meta-analysis. Different durations within the same category were processed using the same steps as described in pairwise meta-analysis. For example, Quinn et al. 30 compared breastfeeding for <4, 4–6, and >6 months. The data in the breastfed for <4 and 4–6 months groups were processed using the steps above.
A frequentist network meta-analysis was conducted using the netmeta package of R software version 3.5.1. The RoM was used to measure an intervention effect in the different breastfeeding groups relative to the never breastfed group. The “forest.netmeta” module in version 3.4.0 of R was used to produce network plots that described and presented the geometry of breastfeeding for ≤6, >6 months, and never breastfed. Nodes were used to represent different interventions and edges for head-to-head comparisons between interventions. The “decomp.design” package assessed homogeneity in the whole network and within designs and homogeneity/consistency between designs. Node splitting was used to evaluate any inconsistency between direct and indirect comparisons if a closed loop existed. 31
We additionally performed a sensitivity analysis to compare the robustness of results using different statistical models (random versus fixed-effects).
Results
A total of 18,026 studies were initially identified as being potentially eligible for inclusion in this review. After excluding duplicates and reviewing article titles and abstracts, 108 studies remained, for which the full text was retrieved. Of these, 35 were conference abstracts, 11 used an incompatible study design, 26 presented ineligible outcomes, 12 studied an inappropriate participant, and 9 presented insufficient data. Finally, 15 studies were selected for inclusion in this analysis. The detailed selection process is described in Figure 1.

Flow diagram.
Fifteen studies involving 12,316 participants were included, evaluating cognition from the ages of 12 months to 10 years. Most studies were from developed countries (15, 88.2%). Only two studies24,32 focused on developing countries. Reliable validated intelligence assessment tools or standard tests designed to provide an estimate of total intelligence were used. The most commonly used measures were the Peabody Picture Vocabulary Test (PPVT), WISC, the Bayley's Scales of Infant Development (BSID), and the Wechsler Preschool and Primary Scales of Intelligence (WPPSI)-R (Table 1).
Characteristics of Included Studies
ASQ, the Ages and Stages Questionnaire; BSID, the Bayley's Scales of Infant Development; BSID-II, the Bayley's Scales of Infant Development-II; K-BSID-II, the Korean version of the Bayley Scales of Infant Development II; MDI, mental development index; PPVT-III, the Peabody Picture Vocabulary Test-III; PPVT-R, the Peabody Picture Vocabulary Test-Revised; WISC, the Wechsler Intelligence Scale; WISC-R, the Wechsler Intelligence Scale-Revised; WPPSI-III, the Wechsler Preschool and Primary Scales of Intelligence-III; WPPSI-R, the Wechsler Preschool and Primary Scales of Intelligence-Revised.
The results of risk of bias assessment are provided in Table 2. Three articles were judged to have a high risk of bias in the assessment of exposure,13,32,33 four studies exhibited high risk of bias in statistical analysis adjustment for prognostic variables,25,27,34 and two displayed high risk of bias in the assessment of outcome.25,35 Overall, nine studies (56.3%) were assessed as being of high quality.
Results of Risk of Bias
We included 11 studies with 15 estimates comparing the impact of breastfeeding with never being breastfed on intelligence in children. We excluded four studies, one because of insufficient data (Gibson-Davis and Brooks-Gunn 33 ) and three where there was no comparison with children that had never been breastfed (Angelsen et al., 34 Clark etal., 32 and Zhou etal. 36 ).
Figure 2 demonstrates that breastfed subjects exhibited a score 1.04-fold greater in intelligence tests compared with never breastfed subjects using a random effects model (RoM: 1.04; 95% CI: 1.02–1.06; p = 0.000). The results obtained when a fixed-effects model was used were similar (RoM: 1.05, 95% CI: 1.04–1.06).

Results of pairwise meta-analysis.
Figure 3 displays a network plot of identified evidence. Twelve studies with 17 estimates involving 8,513 subjects reported on the duration of breastfeeding and intelligence in children. Of these, 8 studies with 4,067 participants compared breastfeeding for ≤6 months to never being breastfed, six studies with 3,366 participants compared a duration of >6 months to never being breastfed, and three studies with 1,080 participants studied breastfeeding for >6 months versus breastfeeding for ≤6 months. Three studies22,25,37 were not included in the network meta-analysis because no clear duration of breastfeeding was reported.
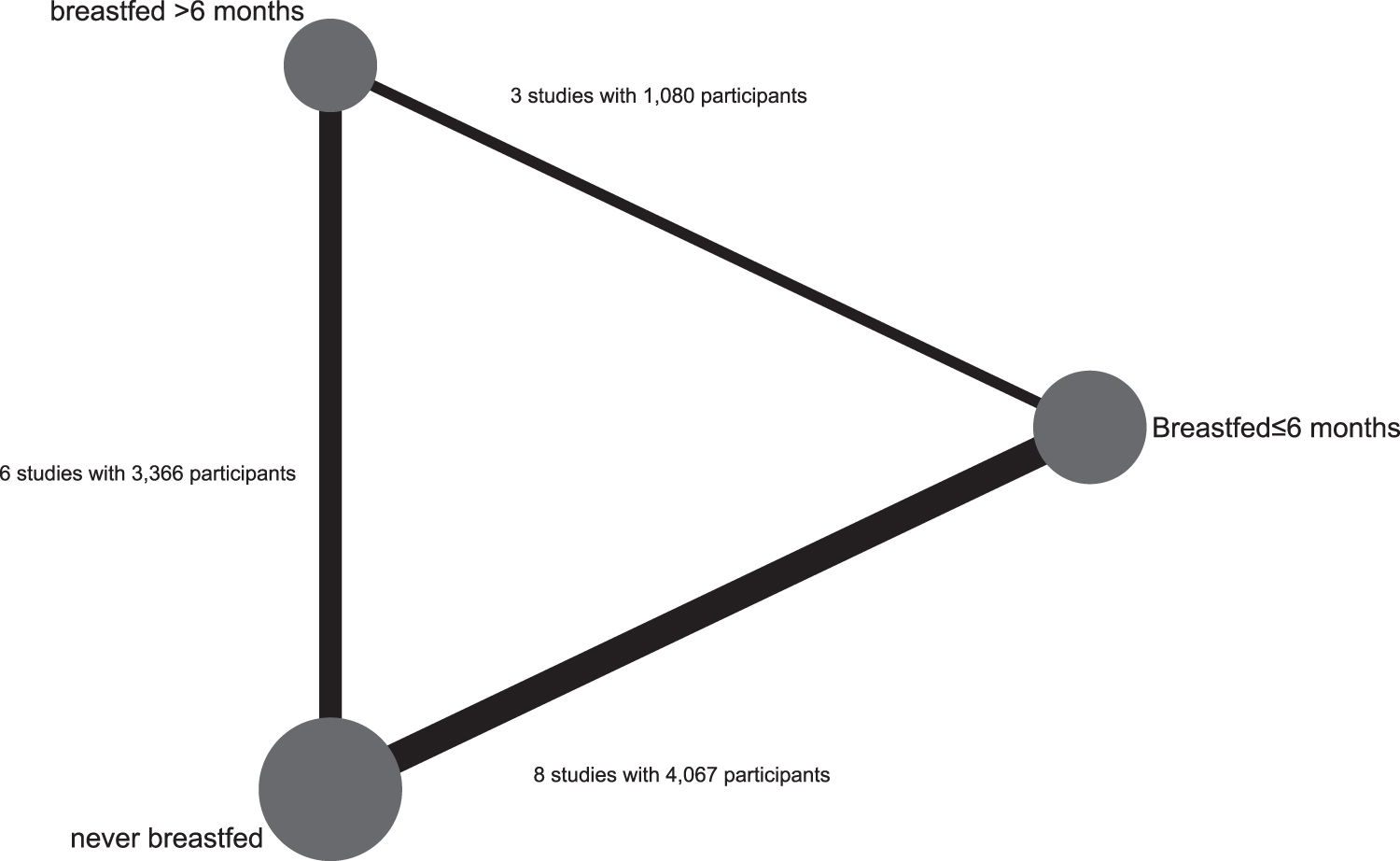
Network plot.
Evidence from a random effects network meta-analysis indicated that breastfeeding for ≤6 months resulted in a score 1.04-fold higher in intelligence tests (RoM: 1.04; 95% CI: 1.03–1.06) and for >6 months 1.06-fold higher (RoM: 1.06; 95% CI: 1.05–1.08) than babies that had never been breastfed. Breastfeeding for >6 months resulted in a score slightly higher than breastfeeding for ≤6 months (RoM: 1.02; 95% CI: 1.00–1.04). The results of a fixed-effects network meta-analysis were similar (Table 3).
League Table of Network Meta-Analysis
Assessment of inconsistency between direct and indirect comparisons using a node-splitting model indicated that there were no inconsistencies in any comparisons (p > 0.05) (Table 4).
Results of Direct, Indirect, and Network Meta-Analyses
Direct: estimated treatment effect (ROM) derived from direct evidence; Indirect: estimated treatment effect (ROM) derived from indirect evidence; NMA: estimated treatment effect (ROM) in network meta-analysis; Inconsistency p-value: p-value of test for disagreement (direct versus indirect).
CI, confidence interval; RoM, ratio of means.
Discussion
Our review investigated the impact of different durations of breastfeeding on the intelligence of children using a network meta-analysis. We included 12 studies of the impact of duration of breastfeeding on the intelligence of children through evaluation of performance in intelligence tests. We observed that breastfeeding was positively associated with intelligence in children and that subjects who had been breastfed for >6 months exhibited scores higher than children that had never been breastfed and those that had been breastfed for ≤6 months [1.06 (95% CI: 1.05; 1.08), 1.02 (95% CI: 1.00; 1.04), respectively].
The study published by Gibson-Davis and Brooks-Gunn, 33 while not included in our meta-analysis because of insufficient data, is described here only qualitatively. They conducted a longitudinal birth cohort involving 1,645 American-born children and compared cognition using the Peabody Picture Vocabulary Test-III (PPVT-III) in children who had been breastfed for at least 1 month with those that had never been breastfed. They demonstrated that breastfed children had PPVT scores that were 6.6 points higher than never breastfed children in unadjusted mean comparisons, although after controlling for maternal performance in PPVT-III, stimulation at home, and socioeconomic and demographic variables, the difference between breastfed and never breastfed children fell to 1.72 points (standard error: 0.60). A few relevant randomized trials were identified, but they were excluded from this meta-analysis because both intervention and comparison groups included subjects that had been breastfed and those that had never been breastfed. Kramer et al. 6 conducted a cluster randomized trial on the promotion of breastfeeding in 31 Belarusian maternity hospitals and affiliated polyclinics. They found that babies that had been exclusively breastfed for 6 months or more were associated with an increase of 5.2 points (95% CI: 3.7–6.7) on the Wechsler Abbreviated Scale of Intelligence in the intervention group at 6.5 years of age. This result reinforces the evidence of observational studies that breastfeeding may have long-term consequences on intelligence. Lucas et al. 12 focused on preterm infants and assessed 300 children with an abbreviated version of the WISC for Children. Their results indicated that breastfed children had an 8.3 point advantage in intelligence at 7.5–8 years over children that had never been breastfed even after adjusting for their mother's education and social class (p < 0.0001). They also demonstrated that breastfeeding provided a beneficial effect on subsequent intelligence of preterm infants.
Previous research on breastfeeding and intelligence included reviews published in 2007, 2013, 2015, and 2018. A systematic review and meta-analysis published in 2007 by Horta et al. suggested that breastfeeding was associated with increased cognitive development in childhood, in studies that controlled for the confounders of socioeconomic status and stimulation at home. 38 Six years later, they updated the review and reported similar results, concluding that even among those studies that adjusted for maternal intelligence, breastfeeding was associated with an additional 2.19 IQ points. 39 In 2015, an updated meta-analysis not only reported a similar association but also suggested that this association was causal for the positive effect of breastfeeding on cognition, also observed in a randomized trial. 17 The most recent relevant review published in 2018 identified new evidence that reinforced the hypothesis that breastfeeding has long-term consequences on performance in intelligence tests and that the positive association also had an impact on human capital and earning ability. 40 More than half of the five systematic reviews are reported as updates of previously completed reviews. Most of them have updated the number of included studies. All five reviews focused on studies that assessed performance in intelligence tests, and they included mental, psychomotor performance development, and other relevant outcomes instead of a single factor.
Our analysis updated two new studies. Lee et al. 25 investigated 697 infants from the Mothers' and Children's Environmental Health (MOCEH) study in Korea, assessing the mental development index (MDI) score in infants during their first 3 years using the Korean version of the Bayley Scales of Infant Development II (K-BSID-II). The results indicated that even after adjusting for covariates, breastfeeding for longer than 9 months resulted in significantly improved cognitive development of Korean infants, positive effects that persisted until the infants were 3 years old. Bernard et al. 22 studied a French population-based cohort and observed that duration of breastfeeding (each month) was positively associated with improvement in full-scale IQ among those children who were breastfed [0.20 (95% CI: 0.00–0.41)]. Their study also demonstrated an association between intelligence of the children at 5–6 years of age and duration of breastfeeding and levels of PUFAs in the colostrum. These results reinforce that the longer breastfeeding is provided, it improves intelligence in children. Since the updated systematic reviews can summarize new evidence 41 and even changed the previous conclusions, more attention should be given to updating reviews. 42
Although we only identified two new studies, compared with previous reviews, our study focused on the duration of breastfeeding rather than whether breastfeeding was provided or not. We also used the RoM to measure the intervention effect of the studies in the breastfed group relative to the never breastfed group because different tests for intellectual performance were performed. More importantly, we used a network meta-analysis to compare breastfeeding for >6 months with breastfeeding for ≤6 months and never breastfeeding, demonstrating that the benefits of breastfeeding to intelligence increase with longer duration of breastfeeding. However, the majority of previous reviews have focused on high-income Western societies with few studies examining Asian countries. We have added additional evidence from Korea, which should make our results more generally applicable. What's more, as previous study reported, Chinese databases were searched rarely in systematic reviews. 43 However, previous study indicated that Chinese biomedical databases should be searched when performing systematic reviews. 44 Actually, we searched Chinese database according to Cochrane Handbook recommendation. In addition, as risk of bias is among the most frequent reasons for downgrading the quality of evidence, 45 we assessed risk of bias in studies included in the review using a tool developed by the CLARITY group.
There are some limitations to our analysis. First, studies were carried out only on subjects who were born healthy and at term. Thus, our findings cannot be applied to breastfed interventions, including other preterm infants or children with certain health problems. Second, due to the absence of evidence from randomized controlled trails, our conclusions were based on evidence from observational studies only, and inherent biases because of confounding and shortcomings of these studies may threaten the validity of the entire network meta-analysis. For example, we were unable to adjust for maternal IQ as this was not available in our review. Unmeasured confounding factors are inevitable, but may have led us to overestimate the true effect of breastfeeding on intelligence. Another important issue to consider is whether the nonrandomized studies address the same research questions or estimate the same treatment effects as the randomized controlled trials. Due to the complexity of the data and the studies' under-reporting, differences in never breastfeed could not be accounted for, and it was assumed that never breastfeed were comparable across included studies. Moreover, never breastfed children were fed with other sources of nutrients, in particular infant formulas, which are not similar across studies. Depending on analytic methods used, nonrandomized studies that compare the same treatment alternatives may produce treatment effects that are valid but different from that estimated in the RCT. Third, since few studies collected systematic data on the duration of exclusive breastfeeding, it was not possible to consider this factor in our analysis. Finally, our literature search requires improvement, although no supplemental search method was conducted in more than 50% of the network meta-analyses. 46
Conclusions
In conclusion, our analysis of intelligence suggests that breastfeeding has a positive impact on the results of intelligence tests of children, although the magnitude of this effect seems to be modest (1.04-fold). In addition, we demonstrated that breastfeeding for longer than 6 months further improved intelligence.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This study was supported by the Fundamental Research Funds for the Central Universities (18LZUJBWZX006, 2019JBKYJC002): Evidence - based sociology research, China Medical Board Open Project Funding (CMB #17–279): Tracking and Evaluating Quality (TEQ) of Rural Health Services in NW China: Tool kits for rural clinic quality management and capacity building and Special Fund for Soft Science in Gansu Province (18CX1ZA043): Study on the Measures to Improve the Quality of Rural Health Services in Gansu Province.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.