
Abstract
Objective:
Colostrum, the first form of human milk, is strongly encouraged for infants due to its benefits. During the early postpartum (PP) period, the secreted colostrum volume can be minimal, causing concerns among mothers about sufficient milk supply. Few studies have examined temporal changes in the colostrum. This study aimed to elucidate the trajectory of expressed colostrum volume in the first 48 hours after delivery.
Materials and Methods
: This was a cross-sectional observational study performed at Kagawa National Children's Hospital. One hundred five mothers who did not directly breastfeed in the first 48 hours after delivery were enrolled in the study. Well-trained midwives instructed the mothers on how to express human milk, and mothers started to express as soon as possible after delivery. Mothers were advised to express human milk every 3 hours, and the milk volume was measured.
Results:
Within 3 hours PP, 60% of mothers expressed milk, and the median frequency of expression was 14 (interquartile range, 11–16) times in the first 48 hours. At 0–3 and 3–6 hours PP, the volume of initially expressed milk was 0.4 (0.0–2.0) mL and 1.0 (0.0–6.0) mL, respectively. Subsequently, milk volume decreased. The volume remained low until 30 hours PP and increased dramatically; this phenomenon is termed secretory activation, which began later in primiparous women than in multiparous women.
Conclusion:
The decline in expressed milk volume during the early PP period caused concern among mothers. Therefore, mothers should be informed of the PP trajectory of human milk volume.
Introduction
Breastfeeding is the optimal way to provide complete nutrition to infants, even for those in neonatal intensive care units (NICUs) who are separated from their mothers. 1 In preterm infants, human milk reduces the risk of necrotizing enterocolitis, which can be lethal, and leads to better developmental outcomes.1–5 Colostrum, the first human milk produced within a few days postpartum (PP), is richer in immunoglobulins, cytokines, and immune cells than mature milk. 6 In addition, it has been reported that colostrum secreted by the mothers of extremely small for gestational age infants is rich in growth factors.7,8 Growth factors are involved in the growth and maturation of the gastrointestinal tract and nervous, hematopoietic, and vascular systems, as the newborn adapts to extrauterine life. Oropharyngeal administration of colostrum improves the immune function of the gastrointestinal tract and the systemic anti-infective capability, especially in preterm infants. Furthermore, it has been reported to be positively associated with a shorter time to regain birth weight, time to full enteral feeding, and reduced hospitalization.9–11
Due to the benefits of colostrum, there is a need for colostrum by mothers whose infants are admitted to the NICU and neonatologists. Therefore, the colostrum volume trajectory and its difference based on a mother's characteristics should be ascertained. A few studies have examined temporal changes in colostrum volume during the early PP period; however, many studies have examined the acute onset of secretory activation within a few days PP.12–14 Secretory activation is characterized by a sudden increase in human milk volume several days after birth. Whether it is breastfeeding or human milk expression, human milk volume is very low after delivery before secretory activation.12–15 In Japan, it is culturally acceptable to express human milk by hand during the initial PP phase. Since Japanese culture allows midwives to support the direct expression of human milk by hand, a support system, wherein midwives teach mothers to manually massage their breasts and express milk with direct touch, has been developed in Japan. The collection of a small amount of hand-expressed human milk from the nipple using a syringe is currently performed in many NICUs in Japan. 13
In this study, mothers who were separated from their infants in the NICU received support on how to perform routine collections of hand-expressed human milk and measure the volume of collected milk. This study aimed to elucidate the trajectory of expressed colostrum volume in the first 48 hours after delivery.
Materials and Methods
Design
We conducted a cross-sectional study of expressed milk volume during the first 48 hours after delivery in mothers whose infants were admitted to the NICU right after birth. This study was approved by the Institutional Review Board of National Kagawa Children's Hospital, and all participants provided written informed consent.
Setting
Data were collected from mothers who delivered at National Kagawa Children's Hospital from January 2011 to September 2012. This hospital has a level IV NICU.
Sample
Mothers who delivered at National Kagawa Children's Hospital were assessed for eligibility in this study. The inclusion criterion was mothers separated from their infants who were admitted to the NICU right after birth. In contrast, the exclusion criteria were mothers who directly breastfed during the study period with infants discharged from the NICU before 48 hours PP and those in whom breastfeeding was considered contraindicated due to poor health condition, viral infection (e.g., HIV, HTLV-1), mental disease, or no desire to breastfeed.
Maternal perinatal information and history were obtained through a chart review. Midwives distributed brochures to mothers before or immediately after giving birth to inform them of the benefits of human milk for infants and the necessity for expression every 3 hours to obtain sufficient milk volumes. Hand expression was performed as soon as possible after delivery. The midwives learned how to support mother's expression from an International Board Certified Lactation Consultant in a 12-hour program; mothers were relaxed and made comfortable before expression, and their breasts were massaged if severe engorged. Similarly, hands-on support was initially provided for hand expression. Mothers compressed the breast between their fingers and thumb to move the milk toward their nipples. Next, they released the tension and repeated the procedure, slightly rotating their hands around the breast. Mothers continued to express for at least 10 minutes even if there was no milk secretion and were encouraged to manually express milk independently every 3 hours as much as they could. The midwives checked the expressed milk volume recorded by mothers on the chart every 3 hours during the first 48 hours after delivery and asked mothers to continue expressing until the milk stopped flowing. If hand expression by the mother was deemed inadequate, the midwife helped with an expression directory.
Data collection
Hand-expressed colostrum was collected using 2.5-mL syringes (Nipro, Osaka, Japan). The mothers compressed their breasts using one hand and exuded human milk, which was collected using a syringe by the other hand. If the mother seemed unable to exude human milk, the midwives helped them. After each measurement, the collected milk was sent to the NICU and either fed to the infant or frozen and stored until the infant needed it.
Data analysis
Data of expressed human milk were analyzed to examine the overall temporal changes in volume and influence of parity (primiparous or multiparous), gestational age, time of the first expression after delivery, and mode of delivery. JMP 8.0 (SAS Institute, Inc., Cary, NC) was used for all statistical analyses. A Wilcoxon signed-rank test and Kruskal–Wallis test were used to examine differences in the volume of expressed human milk according to expression times after delivery.
Results
In total, 105 participants were included (Fig. 1), and 50.5% of the participants were primiparous. Furthermore, 52.4% of the participants gave birth through vaginal delivery, and preterm delivery (≤36 weeks) accounted for 73.3% of births (Table 1).
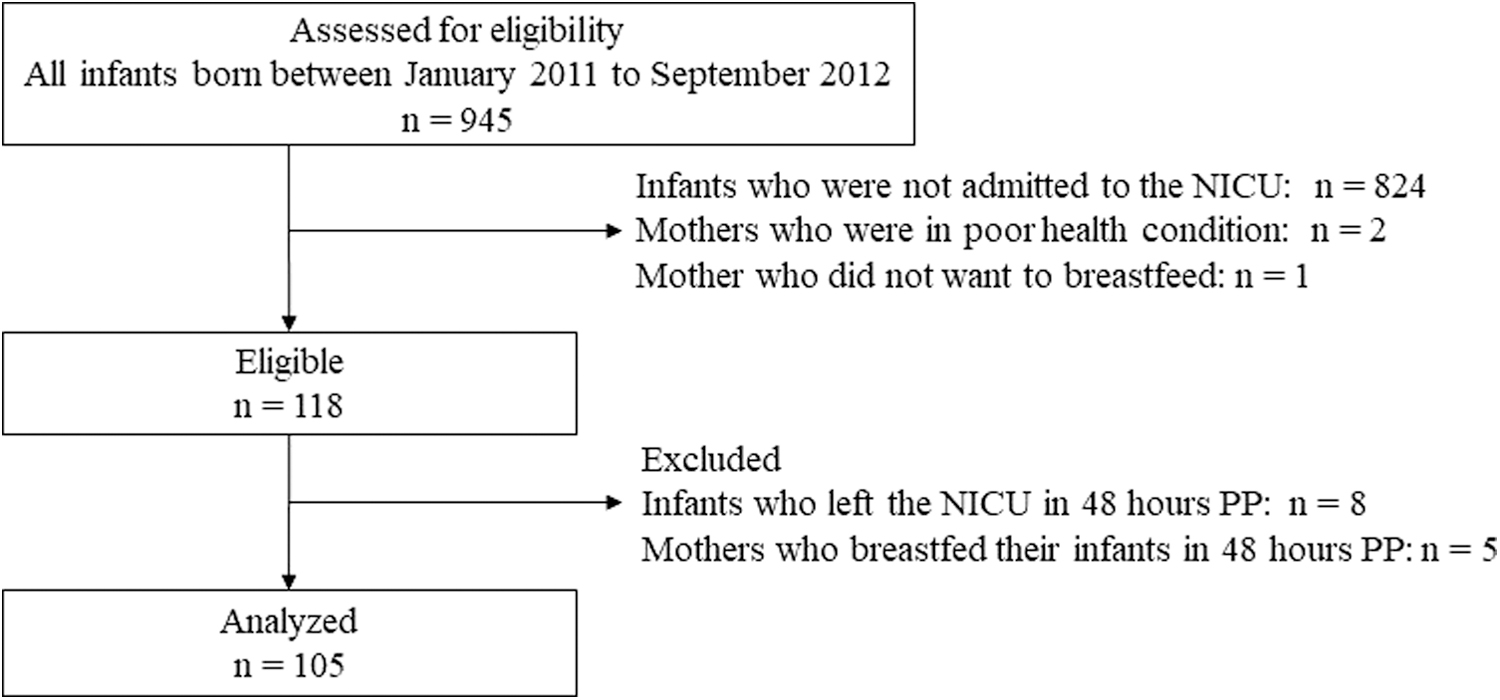
Participant flow diagram.
Characteristics of the Mothers and Their Infants (N = 105)
CS, cesarean section; PP, postpartum.
Sixty-three women (60.0%) began expression within 3 hours PP. The frequency (median [interquartile range]) of expression at 0–24 and 24–48 hours PP was 7 (5–8) and 8 (6–8) times, respectively.
Temporal changes in the volume of expressed human milk
The median volume of expressed human milk was 0.4 (0.0–2.0) mL at 0–3 hours PP and 0.5 (0.5–2.7) mL at 3–6 hours PP. The volume gradually decreased to the lowest amount within 12–15 hours PP. Milk volume did not show a significant difference between women who expressed milk before 30 hours PP and those who expressed milk 12–15 hours PP; however, a sudden increase in volume was observed at 30–33 hours PP (Fig. 2).

Expressed human milk volume curve in the first 48 hours. Milk volumes, measured 3 hourly, are shown as median (
Differences related to parity
In both groups, the expressed milk volume decreased simultaneously and remained low for more than half a day after 12 hours PP. Milk volume increased earlier in multiparous women than in primiparous women (Fig. 3).
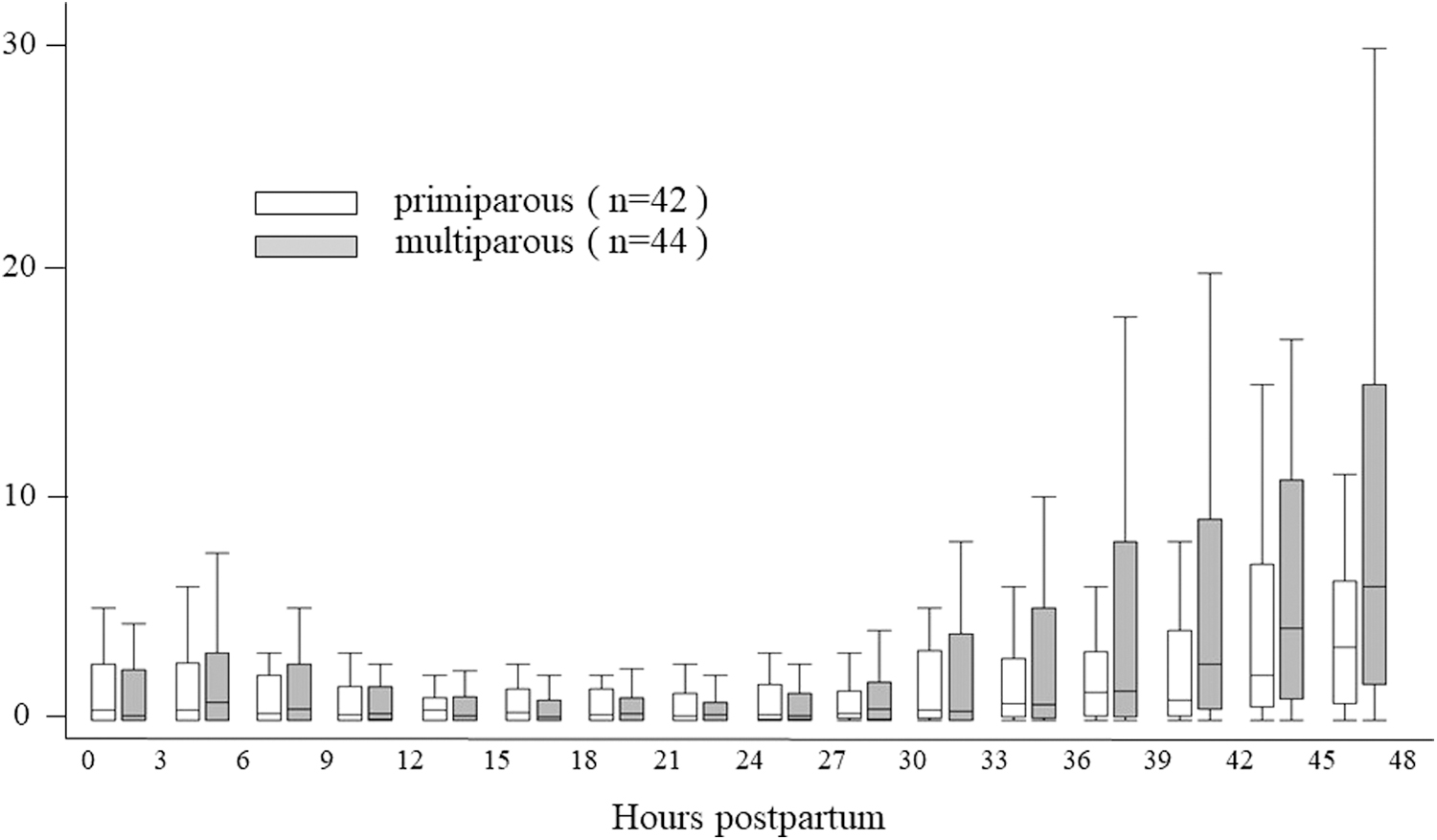
Relationship between human milk volume and parity. The frequency of expression in the first 48 hours PP by primiparous and multiparous women was 15 (13–16) times and 15 (12–16) times, respectively. The total milk volume from primiparous and multiparous women was 13.7 (6.5–42.0) mL and 20.3 (3.9–80.0) mL, respectively.
Differences related to expression starting time
The initial volume of expressed human milk from women who began expression within 3 hours PP was 0.4 (0.0–2.0) mL, while the volume from women who began expression at 3–6 hours PP was 1.0 (0.0–6.0) mL. In both groups, the minimum volume of expressed human milk was recorded at 12–15 hours PP. A significant increase in the volume of expressed human milk compared to 12–15 hours PP was observed at 30–33 hours PP for women who began expression within 3 hours PP and 33–36 hours PP for women who began expression at 3–6 hours PP. Milk volume increased earlier in women who began expression within 3 hours PP than in women who began expression at 3–6 hours PP (Fig. 4).
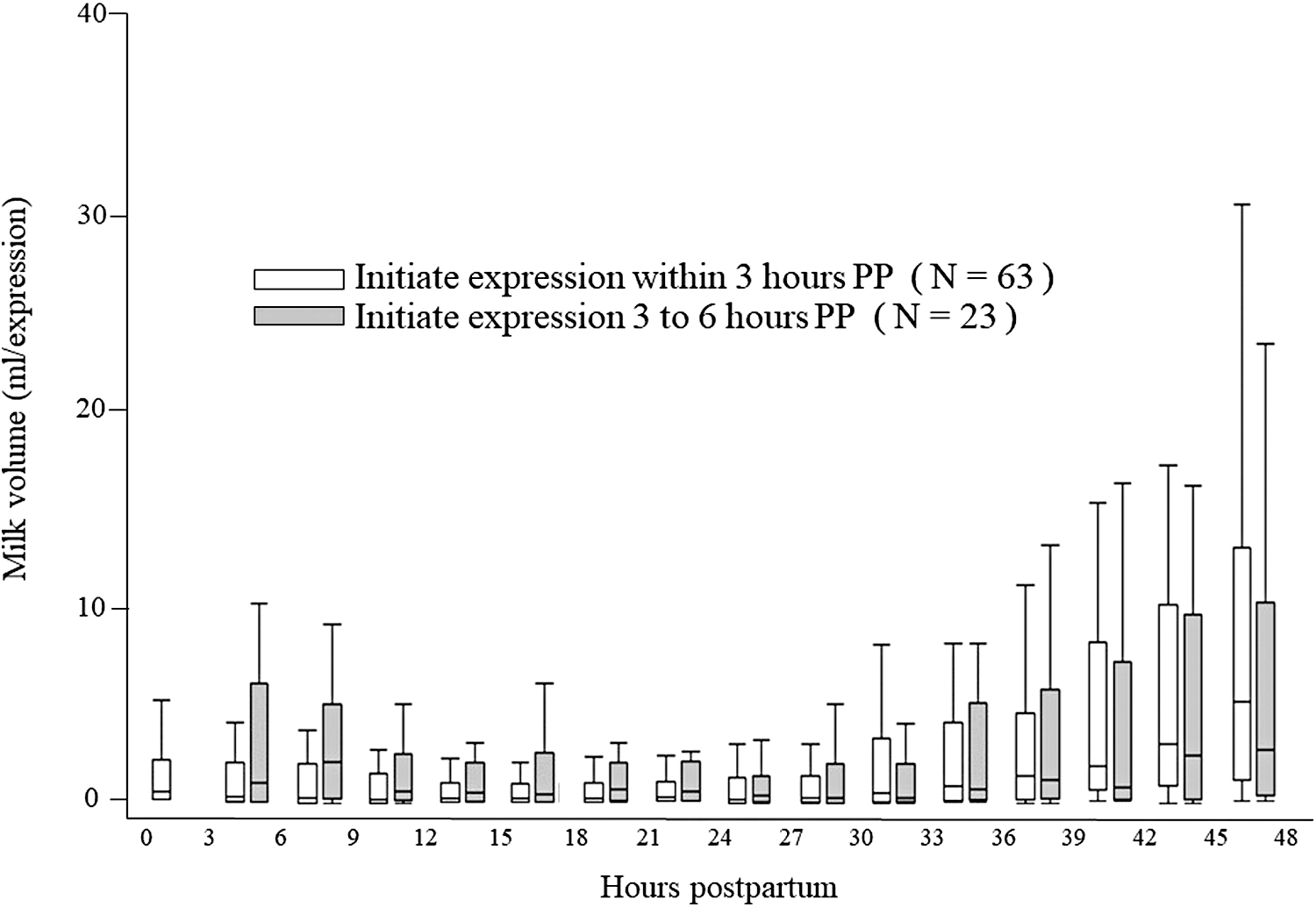
Relationship between human milk volume and time of initiation of milk expression. The frequency of expression in the first 48 hours PP by women who started human milk expression at 0–3 hours PP and 3–6 hours PP was 16 (14–16) times and 14 (11–15) times, respectively. The total milk volume from women who started human milk expression at 0–3 hours PP and 3–6 hours PP was 17.5 (4.3–59.5) mL and 13.1 (5.2–75) mL, respectively.
Differences related to mode of delivery
There were no differences between the vaginal delivery and cesarean section groups in temporal volume changes or total volume [14.7 (3.4–44.3) mL versus 19.1 (4.2–51.8) mL, respectively] of expressed human milk.
Differences related to gestational age at delivery
There were no differences in the volume of expressed human milk when stratifying subjects by gestational age at delivery between those with term birth, gestational age of 32–36 weeks, and gestational age of 22–31 weeks (Fig. 5).

Relationship between human milk volume and gestational age.
Discussion
In this study, 60% of participants started human milk expression within 3 hours PP, and 75% of participants began expressing human milk within 6 hours PP. Previous studies have shown that it is important for mothers who are separated from their infants and unable to breastfeed them to start human milk expression during the early PP period and maintain an appropriate schedule to establish lactogenesis.16,17
It has been reported that hand expression in the early PP period appears to improve eventual breastfeeding rates at 2 months after birth compared with breast pumping. 18 Hand expression has been shown to be beneficial in obtaining a small amount of human milk, especially the colostrum. 13 In this study, well-trained midwives provided initial hands-on support for manual expression and subsequently encouraged the collection of hand-expressed human milk every 3 hours. This enabled collection and measurement of the total volume of secreted colostrum using a syringe.
Most studies examining the volume of expressed human milk compared total daily volume because of the extremely small amount of expressed human milk and significant variations in the mean frequency of breastfeeding.15,19–23 The mean or median expressed total milk volume at 1 and 2 days PP ranged from 0–28 to 0.5–99 mL, respectively, in previous reports.16,20,24,25 This significant variation in the total milk volume likely depended on the support system and maternal background. In this study, the median volume of expressed human milk collected within 24 and 24–48 hours PP was 2.8 (0.1–11.2) mL and 10.3 (2.1–40.0) mL, respectively. In addition, Ohyama et al. 13 found that the volume of expressed human milk collected at a single time using manual expression or a breast pump within 48 hours PP was 2 (median; range, 0–12.6) mL and 0.6 (0–7.2) mL, respectively.
In this study, the volume of expressed human milk gradually reduced after the first or second session and reached the minimum at 12–27 hours PP. In agreement with the study by Ohyama et al., 13 a decline in milk volume with manual and electric expression during the first 48 hours PP was noted following the initial collection of substantial volumes. While the mechanism is unknown, the secretion of oxytocin during delivery and discharge of milk stored in the breast before the first expression may play a role. Regardless of breastfeeding start time, mode of delivery, gestational week at delivery, or parity, the volume of expressed human milk reduced initially, showing the importance of informing mothers of the trajectory of human milk volume.
Delayed onset of secretory activation has been reported to affect human milk volume and subsequent breastfeeding rates.25,26 Therefore, it is essential to monitor the onset of secretory activation. Secretory activation has been evaluated by measuring the total volume of expressed human milk over 1 day and mothers' perceptions of sudden breast fullness.25,27–30 In this study, the volume of expressed human milk reached the minimum at 12–15 hours PP with no significant rise until 30 hours PP. The sudden increase after 30 hours PP is consistent with the findings of previous studies.25–29 Risk factors for delayed onset of secretory activation have been reported to be primipara, cesarean delivery, diabetes mellitus, administration of analgesics, maternal age, breastfeeding start time, and stress at delivery.25–29 Similar to previous studies,27,28 the sudden increase in the volume of expressed human milk was greater in multiparous women than in primiparous women (Fig. 3). We recommend that due to the relatively late onset of secretory activation, inexperienced primiparous women, with concerns about whether the expressed human milk volume is sufficient, should be informed of the trajectory of expressed human milk volume.
Parker et al. 16 reported the importance of starting human milk expression as soon as possible after delivery, and the effectiveness of starting human milk expression within 1 hour PP. Similarly, they reported that women who started human milk expression within 1 hour PP showed a significantly higher human milk volume during the initial expression session (0.1 mL [0–0.3] versus 0 mL [0–0.1] versus 0 mL [0–0], p = 0.002), an earlier onset of secretory activation, higher volume of expressed human milk, and higher rates of breastfeeding at 3 and 6 weeks PP when compared to women who started human milk expression between 1–6 or >6 hours PP, respectively.
In this study, it was possible to study the onset of secretory activation by evaluating the amount of expressed human milk every 3 hours during the first 48 hours PP. Moreover, the initial volume expressed in this study was significantly higher than that reported in the study by Parker et al., 16 possibly because well-trained midwives provided initial hands-on support for manual expression, and hand-expressed human milk was effectively and directly collected from the nipple using a syringe without losing too much milk. Whether human milk volume is higher from women who initiated human milk expression within 1 hour PP than from women who initiated human milk expression after 1 hour PP needs to be further examined.
Henderson et al. 15 reported the effects of gestational age on the volume of expressed human milk and breastfeeding rates. We did not show any significant differences or temporal changes in the volume of expressed human milk by gestational age (Fig. 4). Some studies have shown that the mode of delivery can cause delayed onset of secretory activation and reduced rate of breastfeeding after cesarean delivery.16,24 Our study showed that the mode of delivery had no effect on the total volume or temporal changes in the volume of expressed human milk. This may be because in this study, human milk expression was performed with the support of well-trained midwives who controlled the expression start time and frequency and method of expression.
Limitations
One limitation of our study was that we could not show any statistical significance related to the expression start time due to the small sample size of mothers who started expressing human milk after 3 hours PP. Furthermore, we could not examine mothers who started expression within 1 hour PP. Finally, since our study was not a randomized controlled trial, we could not adjust for maternal background (e.g., academic background, mental condition, body weight, and antenatal corticosteroid treatment) or endocrinological or anatomical status. Thus, we could not elucidate the mechanism underlying decreased colostrum volume. Furthermore, we did not examine the relationship between colostrum volume changes and future breastfeeding rates. Therefore, future studies that include these aspects of breastfeeding should be conducted.
Conclusion
The volume of expressed human milk gradually reduced to a minimum at 12–27 hours PP. Milk volume showed a substantial increase after 30 hours PP (secretory activation). Although the onset of secretory activation was delayed in primiparous women, no significant effect of delivery mode or gestational age at delivery was observed on the onset of secretory activation. These findings suggest that caregivers should reassure mothers, especially primipara, that an early physiological decrease in colostrum is normal and the timing of secretory activation may vary, with milk volumes commonly increasing after ∼30 hours PP. Despite the small volume of colostrum, it is essential to provide support by considering these temporal changes in milk volume.
Footnotes
Authors' Contributions
All persons who meet authorship criteria are listed as authors, and all authors certify that they have participated sufficiently in the work to take public responsibility for the content, including participation in the concept, design, analysis, and writing of the article. Furthermore, each author certifies that this material or similar material has not been and will not be submitted to or published in any other publication.
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.